Academic Emergency Medicine
- Myocardial Infarction Can Be Safely Excluded by High-sensitivity Troponin I Testing 3 Hours After Emergency Department Presentation
- Randomized Double-blind Trial of Intramuscular Droperidol, Ziprasidone, and Lorazepam for Acute Undifferentiated Agitation in the Emergency Department.
- Another study showing the superiority of Droperidol for agitation: adequate sedation in 15 minutes better with Droperidol (64%) than Ziprasidone (35%) or Lorazepam (29%) and lower incidence of respiratory depression with Droperidol (12%) than with Ziprasidone (36%) or Lorazepam (48%).
- Nice review of Droperidol with Reuben Strayer on EMRAP.
- Listen to Strayer’s EMCRIT podcast on managing agitation summarized here.
American Journal of Emergency Medicine
- Complication of vasopressor infusion through peripheral venous catheter: A systematic review and meta-analysis
- another systematic review of peripheral vasopressors showing the incredibly low rate of major complications from this approach
- only 5 major complications (peripheral venous thrombosis) out of 1835 patients.
Annals of Emergency Medicine
- What Is the Accuracy of the Aortic Dissection Detection Risk Score?
- Systematic review of all studies using the ADD-RS score with or without D-Dimer to rule out aortic dissection.
- 8 retrospective studies and 1 prospective study (Diagnostic Accuracy of the Aortic Dissection Detection Risk Score Plus D-Dimer for Acute Aortic Syndromes. The ADvISED Prospective Multicenter Study. Circulation. 2017)
- In a low prevalence setting (pretest probability 5%) ADD-RS >/=1 has a failure rate of 0.8% and an ADD-RS of 2 plus a normal D-dimer has a failure rate of 0.1%.
- For a higher prevalence of AD (20% pretest probability), failure rate of ADD-RS alone would be 3.8%, but when adding a negative D-Dimer, the failure rate of 1 is 0.2% and 2 is 0.5%.
- In summary, in a 5% pretest probability group, ADD-RS=0 rules out AD or ADD-RS=1 plus a negative D-Dimer rules out AD and in a 20% pretest probability group, an ADD-RS=0 or 1 plus a negative D-Dimer rules out AD.
- What Is the Efficacy of the European Society of Cardiology 0/1-Hour Algorithm for Diagnosing Acute Myocardial Infarction? High-sensitivity troponin.
- HS-troponin will replace traditional older troponin assays.
- This synopsis of a study in Heart showed better than 98% sensitivity for MI with a 0/1 hour protocol if pain was ❤ hours or a single troponin if pain was >3 hours.
- The authors cite that a 2% miss rate may not be acceptable in the US but it is just one more study which reinforces the inevitable move toward high-sensitivity troponin.
- Should Nonsteroidal Anti-Inflammatory Drugs Be Used to Provide Analgesia for Fractures?
- Pro and con pieces on whether to use NSAIDS.
- Both pieces agree NSAIDS work well for pain, equivalent to opiates in multiple studies.
- Both agree that risk of fracture healing is not significant when NSAIDS are used for first 72 hours.
- Pro NSAID article argues the risk of fracture healing occurs if NSAIDS are used for>30 days, Con article says risk occurs after 3 days.

- Annals explanation: “Tubercular lymphadenitis presents as a nontender, slowly progressive, unilateral swelling most commonly in the cervical region, classically named scrofula. Because of softer cartilage in children’s airways, mediastinal lymphadenitis can cause significant morbidity and even mortality owing to mass effect on the esophagus and tracheobronchial tree.”

- Annals explanation: “Pott’s puffy tumor. A subperiosteal abscess with associated osteomyelitis of the frontal bone, often referred to as a Pott’s puffy tumor, is a rare entity in children. It can affect children of all ages, but most frequently affects adolescents. It is often a complication of acute bacterial rhinosinusitis, but has also been associated with trauma, surgery, drug use, mastoiditis, and dental infections. Clinical features include fever, headache, and forehead or scalp swelling and tenderness. Patients may also present with vomiting, lethargy, seizures, or altered mental status, depending on the extent of intracranial involvement. Diagnosis is clinical and radiographic, most commonly with CT, magnetic resonance imaging, or both. Management includes antimicrobials in addition to surgical drainage of the abscess, which is commonly polymicrobial with streptococcal, staphylococcal, and anaerobic organisms. The patient underwent operative drainage shortly after diagnosis and was maintained with broad-spectrum antibiotics for several days. She has since made a full recovery.”
BMJ
- Virology, transmission, and pathogenesis of SARS-CoV-2
- Using antibiotics wisely for respiratory tract infection in the era of covid-19
- Diabetic ketoacidosis with SGLT2 inhibitors
Chest
Fluid Response Evaluation in Sepsis Hypotension and Shock A Randomized Clinical Trial
- Randomized trial where control group got usual fluid care strategy and intervention arm got a restrictive fluid strategy driven by passive leg raise and measurement of stroke volume with a noninvasive bioreactance electrode system. The restrictive fluid group had half as many patients requiring mechanical ventilation and one third as many patients requiring dialysis.
- Currently many EDs don’t have the SV technology but it is a good reminder that less fluid is probably better.
- Poor man’s PLR is to measure the pulse pressure (systolic bp-diastolic bp) 30-90 seconds after performing PLR. PLR done by starting patient in 45 degree upright position and then laying them flat and raising legs to 45 degrees.
Clinical Infectious Disease
- Latest recommendations from IDSA on how to protect healthcare workers.
- Nothing new except they no longer have a recommendation to wear double gloves and shoe coverings.
EMRAP
- Cardiology Corner: Pulmonary Embolism Updates- Mattu
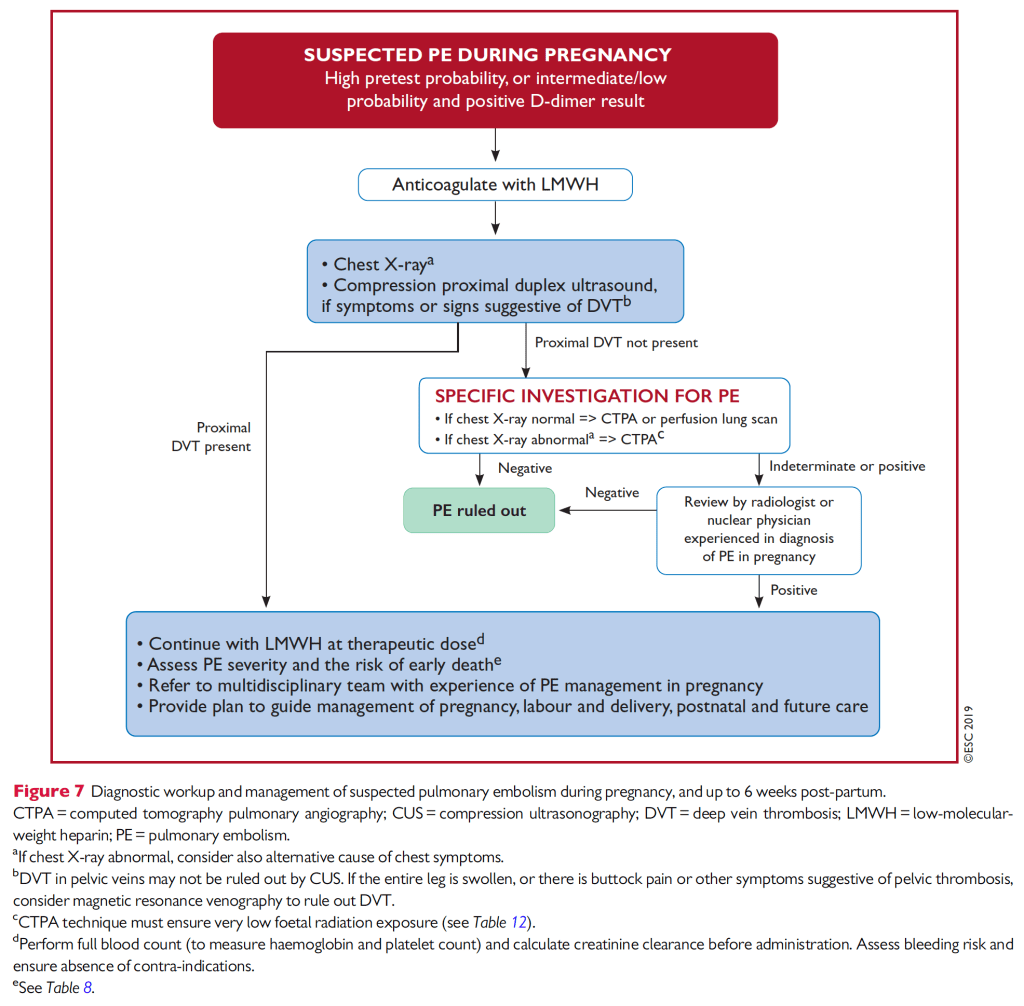
- Mattu spotlights the 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS) published in Jan 2020 which recommends:
- Use YEARS (Lancet 2017) clinical score on MDCALC to rule out PE with a low probability score and D-Dimer<1000. Simplified diagnostic management of suspected pulmonary embolism (the YEARS study): a prospective, multicentre, cohort study, Lancet 2017.
- Use Pregnancy-Adapted YEARS (NEJM 2019) to rule out PE with a low probability and D-Dimer <1000. Pregnancy-Adapted YEARS Algorithm for Diagnosis of Suspected Pulmonary Embolism. Adjusted D-Dimer allowed reduced CT utilization (61%) compared to a similar algorithm without an adjusted D-dimer (84%)- (Righini M, Robert-Ebadi H, Elias A, et al. Diagnosis of pulmonary embolism during pregnancy: a multicenter prospective management outcome study. Ann In- tern Med 2018;169:766-73).
- Critical-care-mailbag-tube-exchange
- Weingart breaks down how to replace an endotracheal tube with a cuff rupture or some type of obstruction.
- High-flow-nasal-cannula-oxygen
- only works for type 1 hypoxemia respiratory failure, not type 2 hypercarbic respiratory failure.
- Mallemat recommends starting at highest settings 60LPM, 100% FiO2, then weaning down as needed.
JAMA
- Another study showing the benefit of hypertonic saline bolus to treat symptomatic hyponatremia. Unfortunately many hospitals do not allow hypertonic saline boluses, instead insisting on slow infusions of hypertonic saline not to exceed 30ml/hr, or they insist on using a central line despite studies cited by UPTODATE showing peripheral infusion is safe (Incidence of Adverse Events During Peripheral Administration of Sodium Chloride J Intensive Care Med. 2018 and Safety of Continuous Peripheral Infusion of 3% Sodium Chloride Solution in Neurocritical Care Patients Am J Crit Care. 2016).
- I was able to get my hospital to agree to the 100cc hypertonic saline bolus after citing the articles and blog posts referenced here, citing that UPTODATE recommends rapid intermittent bolus therapy for severe symptomatic hyponatremia, and explaining that without the bolus option physicians are forced to use normal saline which can paradoxically lower the already low sodium concentration in SIADH patients because the saline infusion induces a diuresis of concentrated urine which (read the explanation in this UPTODATE chapter).
NEJM
- Migraine
- Review article more geared to primary care but has a nice tables of three classes of migraine and algorithm for outpatient treatment and prevention.
- My one page summary.
- Esophageal Motility Disordersand Gastroesophageal Reflux Disease
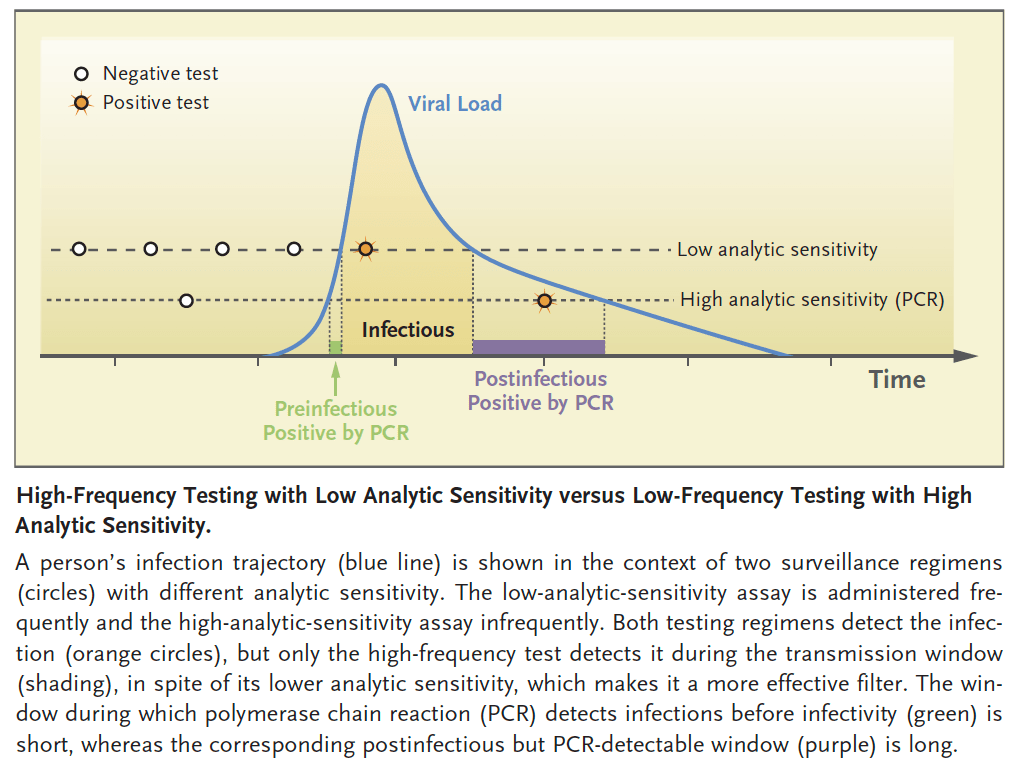
- Rethinking Covid-19 Test Sensitivity — A Strategy for Containment
- rather than focus on super sensitive PCR tests that are more expensive and have a slower turnaround, choose less sensitive antigen tests which cost <$5 and can be done at home or point of care with quick results.
- the key is frequent testing to catch someone early in their period of transmissibility to break chain of spread.
- since the trajectory of virus replication is exponential at beginning, the difference in time between when a low sensitivity and high sensitivity test become positive could be a matter of hours.
- “You Are Now Entering a Guilt-free Zone”
- Proactively stating, “before we go on, I need to tell you something about me, I don’t do guilt,” can help ease a patient’s anxiety about answering questions of health behaviors (e.g. drugs, tobacco, alcohol, etc).
Resuscitation
