Academic Emergency Medicine
Evaluation of Potentially Inappropriate Medications for Elderly Patients
- ED-initiated XR-BUP was associated with substantial reductions in opioid and polysubstance use during the first week post-discharge, supporting its role in early overdose risk mitigation and highlighting its value as an ED-based intervention for opioid use disorder.
Annals of Emergency Medicine
Two-bag Versus One-bag Method for Adult and Pediatric Diabetic Ketoacidosis Management
- Conclusion: The two-bag method is associated with reduced incidence of hypoglycemia and time to DKA resolution in both adult and pediatric populations.
EMCRIT
PulmCrit: Catheter-directed lysis = Peripheral lysis for PE (STRATIFY trial!)
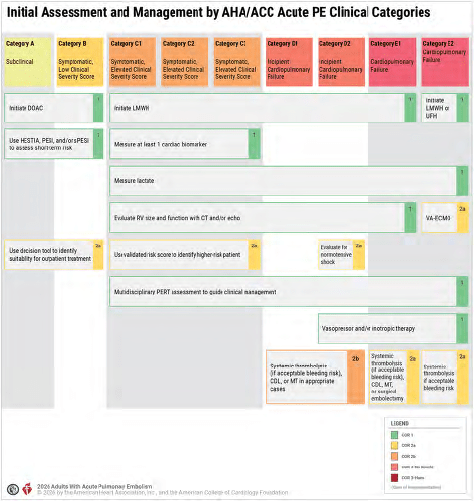
PulmCrit: Four fatal flaws in the new AHA/ACC risk-stratification system for PE
- Failure to delineate low-risk PE which is low sPESI plus no rv dilation or trop elevation
- Vagueness about biomarkers: they add BNP to troponin, most risk strat tools don’t use BNP
- Transient hypotension could be an inaccurate reading
- Nonsensical definition of normotensive shock
Better to use ESC 2019 categorization system
EMRAP
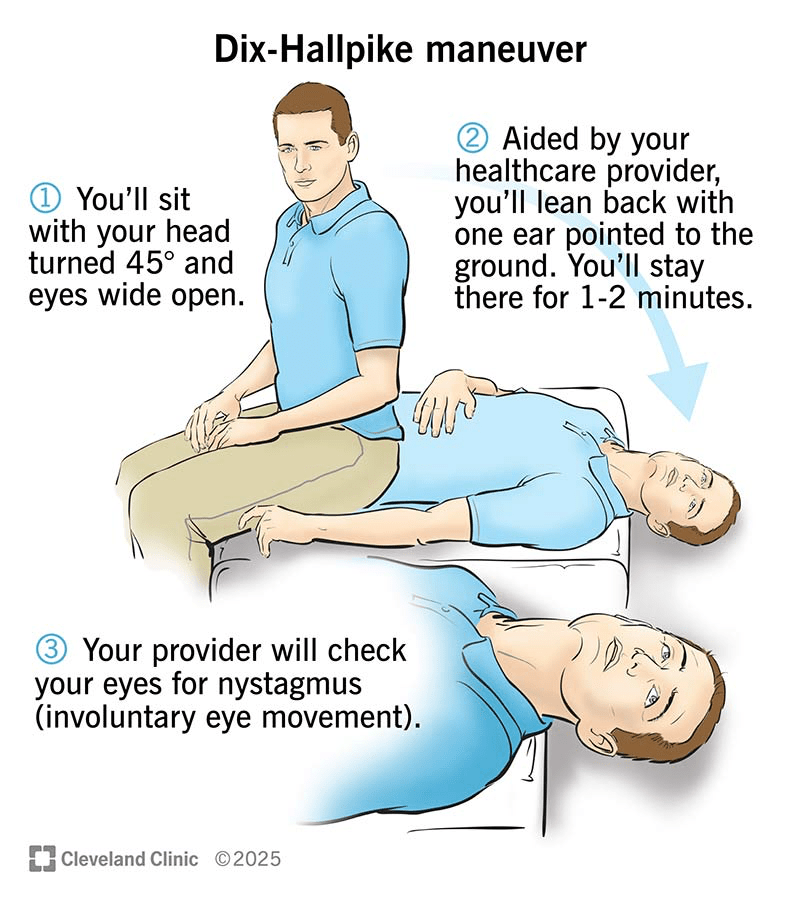
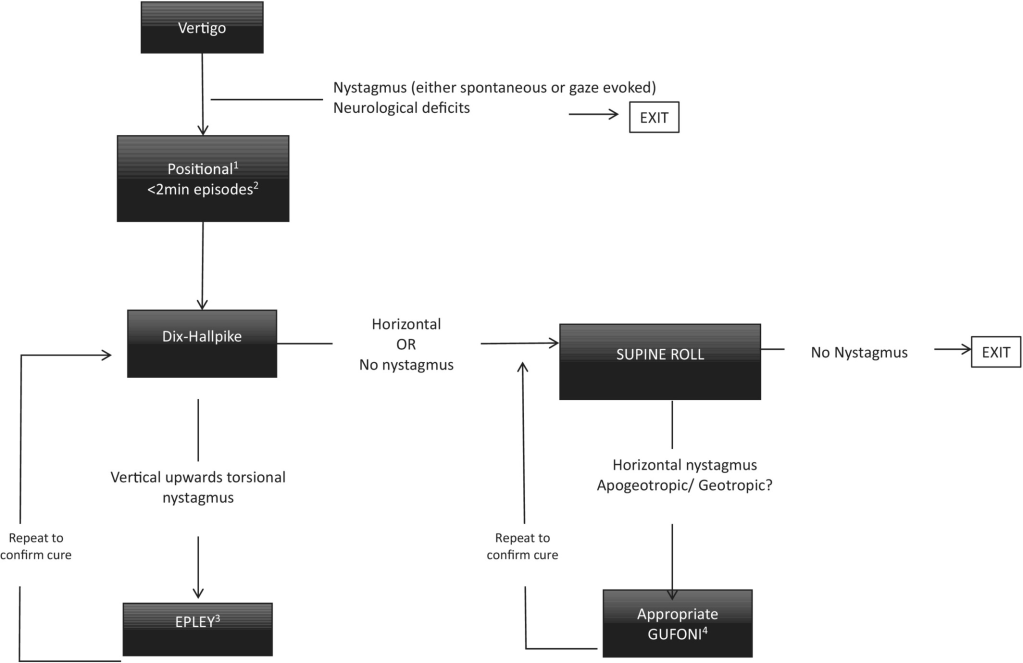
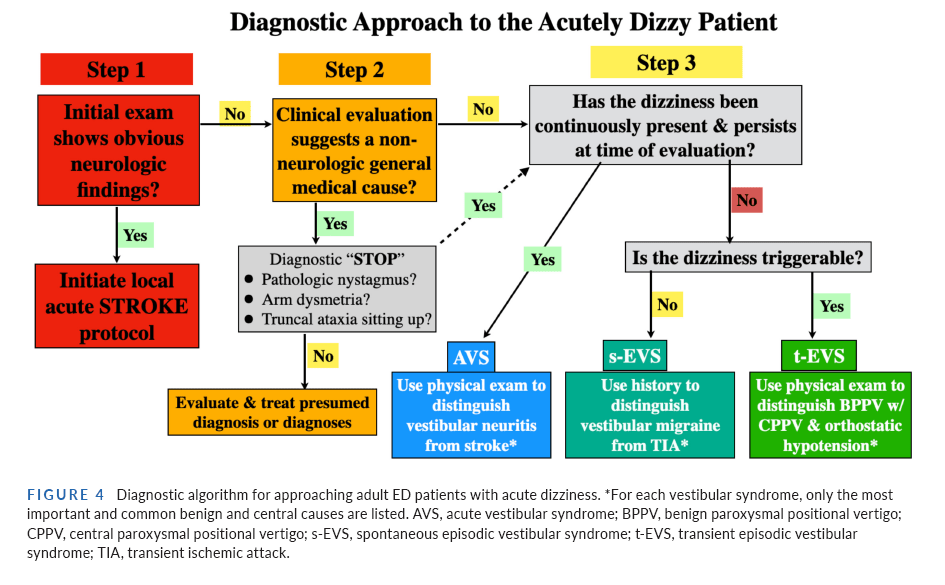
Cumulative incidence of stroke disability and mortality following emergency department discharge for dizziness: a cohort study Kerber KA, Sangha N, Burke JF, et al. Ann Emerg Med. Published online November 18, 2025. doi:10.1016/j.annemergmed.2025.09.029
- Essentially, the study indicated a very low incidence, on the order of 1 in 1,000, of subsequent stroke diagnosis, thus suggesting that missed stroke is uncommon in patients presenting with dizziness who are discharged from the ED.
Bleeding Tracheostomy
Jessica Mason, MD, and Laura Bontempo, MD
- Prepare for the worst when receiving a patient with a report of a bleeding tracheostomy (trach). The dreaded complication is a tracheoinnominate artery fistula.
- Have all difficult airway equipment available and a resuscitation team at the bedside.
- In this case, we have a 58-year-old woman tachycardic to the 120s, BP 130/92 mm Hg, saturating 92% with supplemental oxygen to the trach.
- There is oozing around the trach and what appears to be granulation tissue.
- Her trach was placed 2.5 months prior for chronic respiratory failure from chronic obstructive pulmonary disease (COPD).
- She had visited the ED 2 weeks earlier for a similar presentation, and a CT pulmonary angiogram at that time was negative for pulmonary embolism (PE).
- She is on apixaban for atrial fibrillation.
- Tracheoinnominate artery fistulas can have a sentinel bleed and then a period of stability that can be falsely reassuring.
- These are most common within 3 to 4 weeks after the tracheostomy is placed, but there are reports of cases occurring years later.
- Consider the differential diagnosis of a bleeding tracheostomy:
- Hemoptysis from PE, pneumonia, or lung mass
- Friable granulation tissue at the stoma (most common)
- Imaging
- A CT angiogram (CTA) of the neck is the most helpful study to rule out a tracheoinnominate artery fistula. Since the patient had a recent CTA of the lungs, you can see if this captured images high enough in the neck.
- Tracheostomy tube sizes
- If, for some reason, you need to exchange a tracheostomy, remember that sizes are different among manufacturers.
- Use the outer cannula diameter to guide which size tube to use, since this will be consistent across brands, and allow for proper fit in the patient’s stoma.
- For bleeding granulation tissue, you can apply topical hemostatics, direct pressure, or consider cautery with silver nitrate.
- If the consultant who placed the tracheostomy is available, they should be involved in the care.
- If the patient has a laryngectomy (not a tracheostomy), tracheoinnominate artery fistulas are less common, but there can still be bleeding complications, which should be approached the same way.
Don’t Get FLOXED!!!
Mizuho Morrison, DO, and Sean Nordt, MD, PharmD
Miz and Sean discuss the term “FLOXED,” fluoroquinolone adverse effects, and the role of fluoroquinolones in patient care.
What does getting “FLOXED” mean?
- FLOXED is an informal term for an injury from a fluoroquinolone.
- It describes a person with persistent multi-system symptoms after fluoroquinolone exposure.
- Fluoroquinolone-associated disability (FQAD) is a regulatory term for disabling effects after fluoroquinolone use.
- It poses a medical-legal risk.
Mechanism of action of fluoroquinolones:
- Bacteriocidal by attacking DNA gyrase
- Mitochondrial toxin → oxidative stress, decreased ATP production
- Chelates Ca, Mg, Fe → impaired collagen synthesis and tendon integrity
- Increases matrix metalloproteinases → connective tissue degradation
- Gamma-aminobutyric acid (GABA)-A receptor antagonism → central nervous system (CNS) excitation, neuropsychiatric effects
Fluoroquinolones are effective, but have detrimental side effects:
- Tendon ruptures or tendinopathy
- Aortic dissection and aneurysms
- Peripheral neuropathy
- QT prolongation and torsades
- Drug-drug interactions and food interactions
- Cannot be taken with dairy products or tetracyclines
*Several boxed warnings exist for the above side effects
What symptoms are included with being “FLOXED”?
- Cognitive impairment
- Fatigue
- Trouble sleeping
- Headaches
- Tendon pain
- Anxiety
- Muscle pain
*Symptoms associated with being “FLOXED” may encompass those beyond the known concern with the fluoroquinolone drug class. These nonspecific symptoms are being attributed to the fluoroquinolone drug, which poses a huge medical-legal risk.
Do not use fluoroquinolones routinely.
The Infectious Diseases Society of America (IDSA) states that fluoroquinolones should not be used as first-line therapy for
- Acute bacterial sinusitis
- Acute exacerbation of chronic bronchitis/COPD
- Uncomplicated urinary tract infection
- Community-acquired pneumonia
- Skin and soft tissue infections
- Outpatient diverticulitis
When to use a fluoroquinolone?
Fluoroquinolones should only be used as third- or fourth-line therapy in the following:
- Complicated urinary tract infections (cUTI) and pyelonephritis only when culture shows resistance to safer agents
- Bacterial prostatitis when culture and susceptibility indicate fluoroquinolone sensitivity and alternatives are unsuitable
- Must take the fluoroquinolone for 3-4 weeks, which can increase risk of adverse effects
- Anthrax: Post-exposure prophylaxis and treatment
- Plague (Yersinia pestis): Ciprofloxacin or levofloxacin when preferred agents are not available
- Severe multidrug-resistant gram-negative infections where susceptibility is proven and no better oral options exist
- Travelers’ diarrhea in select high-risk cases, especially with multidrug-resistant pathogens
- Meningococcus post-exposure prophylaxis:
- Ceftriaxone 250 mg intramuscularly once
- Preferred in pregnancy and can be used in all ages
- Rifampin 600 mg orally every 12 hours for 2 days (total of 4 doses)
- Ciprofloxacin 500 mg orally once
- Avoid in pregnant women and children; contraindicated in areas with documented ciprofloxacin-resistant Neisseria meningitidis
- Ceftriaxone 250 mg intramuscularly once
If there is an equally efficacious medication for the patient, try to prescribe the alternative agent. However, if the best option is a fluoroquinolone, these medications can be prescribed with caution.
- Counsel the patient prior to administering a fluoroquinolone.
- Document the conversation and consent.
- Consider getting written consent.
- Discuss return precautions with the patient.
Factors that increase risk for fluoroquinolone adverse effects:
- Patients >60 years of age
- Concomitant systemic corticosteroid use
- History of tendon disorders
- Organ transplant recipients
- Intensive physical activity
- Chronic renal failure or dialysis
- Known aortic aneurysm/dissection
- Connective tissue disorders
- Hypertension
- Peripheral vascular disease
PEARLS: Try to avoid prescriptions for fluoroquinolones and consider alternative medical therapy. However, if fluoroquinolones are the best therapy for the patient, have a shared decision-making conversation and consider obtaining formal consent. Do not prescribe fluoroquinolones with a course of steroids.
Medetomidine Toxicity and Withdrawal
Stuart Swadron, MD, Sean Patrick Nordt, MD, PharmD
- Medetomidine, a potent veterinary α₂-adrenergic agonist, has emerged as an adulterant in fentanyl markets, with early reports of high prevalence in Philadelphia and parts of the Mid-Atlantic and Midwest.
- Unlike classic opioid overdose, the most clinically dangerous manifestation may be severe withdrawal rather than intoxication.
- The clinical features include the mixed opioid–α₂ agonist toxidrome and subsequently, the potentially life-threatening withdrawal syndrome.
Pharmacology
- Veterinary α₂-adrenergic agonist used for sedation and analgesia and not approved for human use.
- Racemic mixture of dexmedetomidine (active) and levomedetomidine (inactive) and estimated to be 10–100 times more potent than xylazine at α₂ receptors.
- Presynaptic α₂ activation decreases norepinephrine release and suppresses sympathetic outflow, producing sedation, bradycardia, and hypotension.
- Chronic exposure can produce physiologic dependence, and abrupt discontinuation may cause rebound sympathetic activation.
Illicit drug supply
- Most commonly detected in fentanyl-containing products, and can be found with xylazine.
- Clinical diagnosis
Mixed Opioid–α₂ Agonist Toxidrome
- Sedation or coma, slurred speech, respiratory depression, miosis, bradycardia, hypotension or early paradoxical hypertension, hypothermia, reduced sympathetic tone.
- Sedation often persists after naloxone reverses respiratory depression. Bradycardia and hypotension are a clue. History may include fentanyl or heroin use in regions with known adulteration.
Medetomidine Withdrawal
- Chronic α₂-agonist exposure causes receptor adaptation and tolerance.
- Abrupt discontinuation produces a catecholamine surge and sympathetic overactivity, resulting in severe autonomic instability.
- Onset: typically 6–24 hours after last exposure, occasionally earlier, peak: usually within 24–72 hours.
- Duration: mild cases resolve in several days, severe cases may persist up to one to two weeks.
Clinical features
- Severe hypertension, marked tachycardia, tremor, diaphoresis, agitation, delirium, encephalopathy-like presentations, nausea, vomiting, dysrhythmias.
- May resemble alcohol or benzodiazepine withdrawal.
- Benzodiazepines and phenobarbital often provide limited control.
- Clinical improvement with α₂-agonist therapy supports the diagnosis.
Management
- Primary management focuses on supportive care and α₂-agonist therapy to suppress sympathetic overactivity and stabilize withdrawal (eg, clonidine for mild to moderate, dexmedetomidine for severe).
- Supportive care includes intravenous fluids, antiemetics, treatment of agitation with antipsychotics when needed.
- Intensive care monitoring may be required for severe hypertension, persistent vomiting, altered mental status, or failure of oral therapy.
Disposition
- Patients who stabilize may be discharged with a short outpatient taper of α₂-agonist therapy (eg, clonidine).
- Outpatient management should only be considered in clinically stable patients without severe hypertension, delirium, persistent vomiting, chest pain or syncope, or significant laboratory abnormalities.
Medetomidine Toxicity and Withdrawal
Stuart Swadron, MD, Sean Patrick Nordt, MD, PharmD
- Medetomidine, a potent veterinary α₂-adrenergic agonist, has emerged as an adulterant in fentanyl markets, with early reports of high prevalence in Philadelphia and parts of the Mid-Atlantic and Midwest.
- Unlike classic opioid overdose, the most clinically dangerous manifestation may be severe withdrawal rather than intoxication.
- The clinical features include the mixed opioid–α₂ agonist toxidrome and subsequently, the potentially life-threatening withdrawal syndrome.
Pharmacology
- Veterinary α₂-adrenergic agonist used for sedation and analgesia and not approved for human use.
- Racemic mixture of dexmedetomidine (active) and levomedetomidine (inactive) and estimated to be 10–100 times more potent than xylazine at α₂ receptors.
- Presynaptic α₂ activation decreases norepinephrine release and suppresses sympathetic outflow, producing sedation, bradycardia, and hypotension.
- Chronic exposure can produce physiologic dependence, and abrupt discontinuation may cause rebound sympathetic activation.
Illicit drug supply
- Most commonly detected in fentanyl-containing products, and can be found with xylazine.
- Clinical diagnosis
Mixed Opioid–α₂ Agonist Toxidrome
- Sedation or coma, slurred speech, respiratory depression, miosis, bradycardia, hypotension or early paradoxical hypertension, hypothermia, reduced sympathetic tone.
- Sedation often persists after naloxone reverses respiratory depression. Bradycardia and hypotension are a clue. History may include fentanyl or heroin use in regions with known adulteration.
Medetomidine Withdrawal
- Chronic α₂-agonist exposure causes receptor adaptation and tolerance.
- Abrupt discontinuation produces a catecholamine surge and sympathetic overactivity, resulting in severe autonomic instability.
- Onset: typically 6–24 hours after last exposure, occasionally earlier, peak: usually within 24–72 hours.
- Duration: mild cases resolve in several days, severe cases may persist up to one to two weeks.
Clinical features
- Severe hypertension, marked tachycardia, tremor, diaphoresis, agitation, delirium, encephalopathy-like presentations, nausea, vomiting, dysrhythmias.
- May resemble alcohol or benzodiazepine withdrawal.
- Benzodiazepines and phenobarbital often provide limited control.
- Clinical improvement with α₂-agonist therapy supports the diagnosis.
Management
- Primary management focuses on supportive care and α₂-agonist therapy to suppress sympathetic overactivity and stabilize withdrawal (eg, clonidine for mild to moderate, dexmedetomidine for severe).
- Supportive care includes intravenous fluids, antiemetics, treatment of agitation with antipsychotics when needed.
- Intensive care monitoring may be required for severe hypertension, persistent vomiting, altered mental status, or failure of oral therapy.
Disposition
- Patients who stabilize may be discharged with a short outpatient taper of α₂-agonist therapy (eg, clonidine).
- Outpatient management should only be considered in clinically stable patients without severe hypertension, delirium, persistent vomiting, chest pain or syncope, or significant laboratory abnormalities.
NEJM
- Botulism case
Bleeding Risk with Apixaban vs. Rivaroxaban in Acute Venous Thromboembolism
- Among patients with acute venous thromboembolism, the risk of clinically relevant bleeding was significantly lower with apixaban than with rivaroxaban during the 3-month treatment period.
REBELEM
- No difference
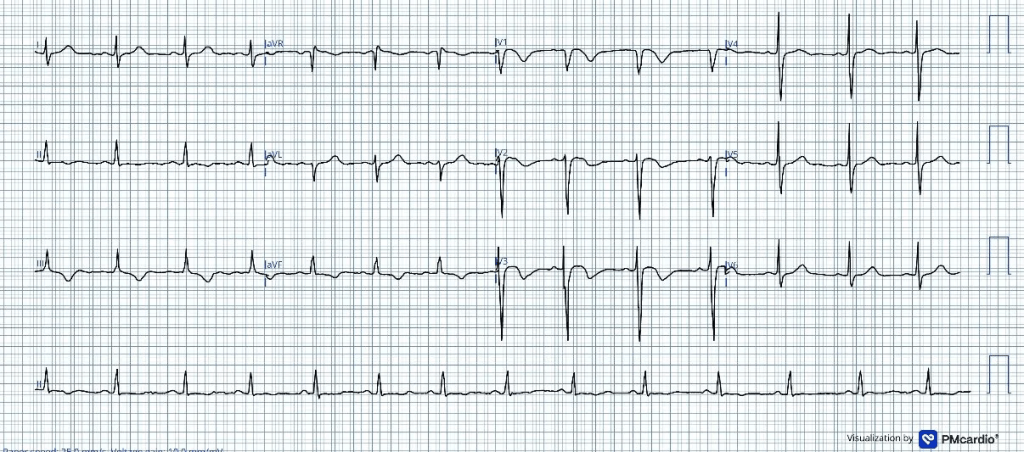
The Queen of Hearts Returns: AI vs Physicians in STEMI-Equivalent and STEMI-Mimic ECGs
- ♥️ Queen of Hearts AI outperformed both emergency physicians and cardiologists when interpreting challenging STEMI-equivalent and STEMI-mimic ECGs.
- ⚡ These are some of the hardest ECGs to interpret, where missed OMIs can delay reperfusion and false positives can trigger unnecessary cath lab activation.
- 🫀 Physicians missed 41% of true OMIs, while the Queen of Hearts AI missed only 11%, suggesting meaningful improvement in detection.
- 🎯 The AI also reduced overcalling of non-OMI ECGs, which could help decrease unnecessary catheterization laboratory activations.
MDCalc Wars: HAT vs SEDAN — Hemorrhage Risk After Stroke Thrombolysis
- 🧠 HAT and SEDAN help estimate symptomatic intracranial hemorrhage risk after stroke thrombolysis and can support real-time bedside counseling.
- ⚡ HAT is faster and simpler, making it useful when you need a quick estimate with basic clinical and CT data.
- 🖥️ SEDAN adds more imaging detail, which may provide a more refined risk estimate when CT findings are well characterized.
- ⚠️ These scores are adjuncts, not gatekeepers and should not be used alone to deny thrombolytics to otherwise appropriate patients.
- 🗣️ Best use case: inform shared decision-making, set expectations with families, and guide post-treatment monitoring.





{kind=link}