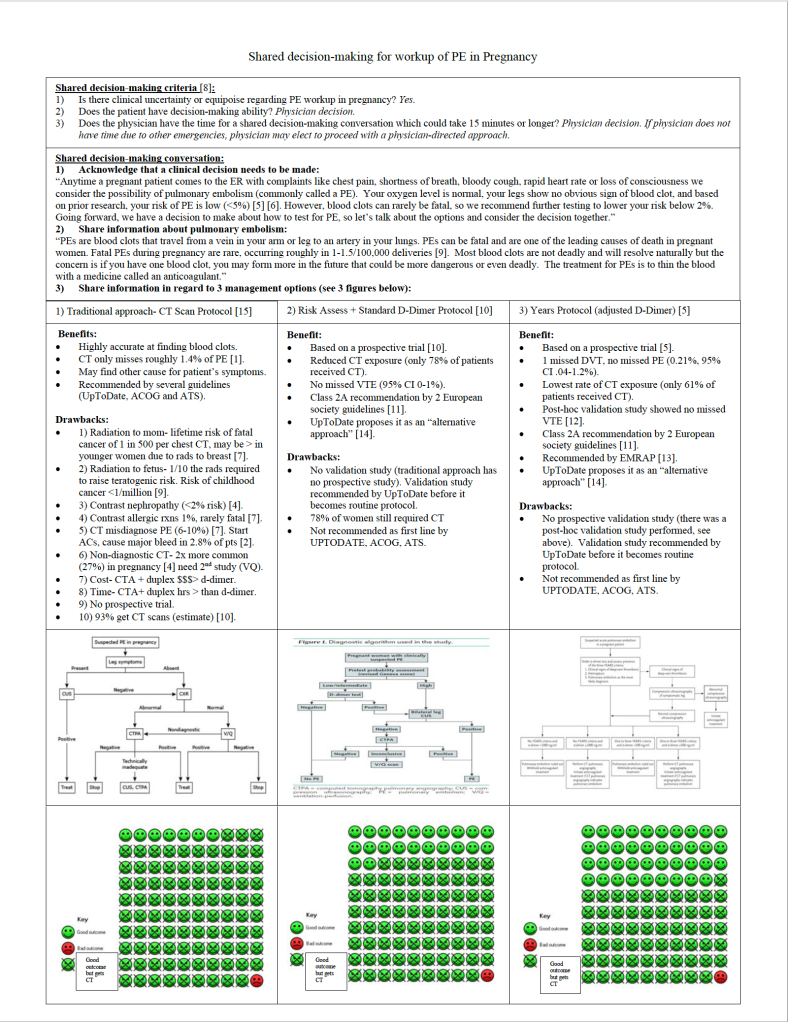
Despite physiologic reasons why pregnant women would be at increased risk for PE (hypercoagulable state, venous stasis ), they surprisingly have roughly the same rate of diagnosed PE (32/100k) as the general population of women under the age of 40 according to Olmsted County data published by Heit and referenced by Kline, as long as you remove isolated DVT and postpartum state. Early postpartum state, on the other hand, has roughly a 10 fold increased risk (421/100k). Normal physiologic changes of pregnancy such as dyspnea, leg swelling, increased resting heart rate can all mimic PE. For this reason, as well as the specter of missing potentially deadly PE that harms two patients simultaneously, physicians have been found to overtest for VTE, with a rate of positive VTE around 4% (Kline 2014 and van der Pol 2019), which is 1/3 the rate of positive workups in the general population. To make matters worse, the traditional workup, endorsed by American Thoracic Society and ACOG in 2011, did not use risk assessment or D-Dimer in pregnant patients due to lack of prospective trials and instead went directly to duplex and CT or VQ. As Kline breaks down in his 2015 review of the workup for PE, the risks to pregnant moms from CT not only include the 1 in 500 chance of a fatal cancer, but also the 26% chance of a non-diagnostic study study (higher cardiac output and higher plasma volume during pregnancy make the timing of the bolus less reliable), and the 6-10% chance of a false positive study in low risk populations which subjects the patient to 3-6 months of anticoagulation.
For many emergency clinicians, the NEJM publication of van der Pol’s Pregnancy-Adapted Years Algorithm for Diagnosis of Suspected Pulmonary Embolism in 2019 was all we needed to begin offering patients an alternative to mandatory CT for all low risk PE workup. Righini had already published a Pregnancy PE protocol that employed risk assessment with a normal D-Dimer but unfortunately this only reduced CT utilization in 22% of pregnant patients.
The challenge with using Years to guide management is that some leading expert guidelines (ACOG and ATS) which have not been updated since 2011 still recommend CT for all or, in the case of UpToDate, are calling for a second validation study before recommending the Years approach. Years was validated by the Righini group in a post-hoc fashion and showed a 0% miss rate but a prospective validation study is not yet published.
So what is a pregnant patient and a well-intentioned physician to do?
Shared decision-making!
Here is my attempt at a shared decision-making script to help patients decide what feels best for them.
Shared decision-making for workup of PE in Pregnancy