Academic Emergency Medicine
Peripheral Nerve Block for Hip Fracture
- The American Academy of Orthopedic Surgeons recommends regional analgesia for preoperative pain control in patients with hip fracture (strong evidence).11 Based on the available evidence, the review summarized here found that PNB reduced pain on movement, shortened time to first mobilization, and resulted in lower rates of delirium and chest infections. Thus, we have assigned a color recommendation of green (benefit > harm) for PNB for hip fracture. Further study is needed to evaluate PNB in periods and settings other than the perioperative period and the potential benefit of continuous infusion versus single injection. However, current data support that this would be a valuable intervention for hip fractures that could be utilized in the ED.
Neuraminidase inhibitors for treatment of influenza
- In summary, the existing data indicate that NAIs reduce the duration of symptoms by less than 1 day in patients with confirmed or suspected influenza. The use of NAIs to treat influenza does not prevent hospitalization and is associated with adverse events. Therefore, we have assigned a color recommendation of yellow (unclear if it provides benefit, more data needed) to this treatment.
American Journal of Emergency Medicine
None
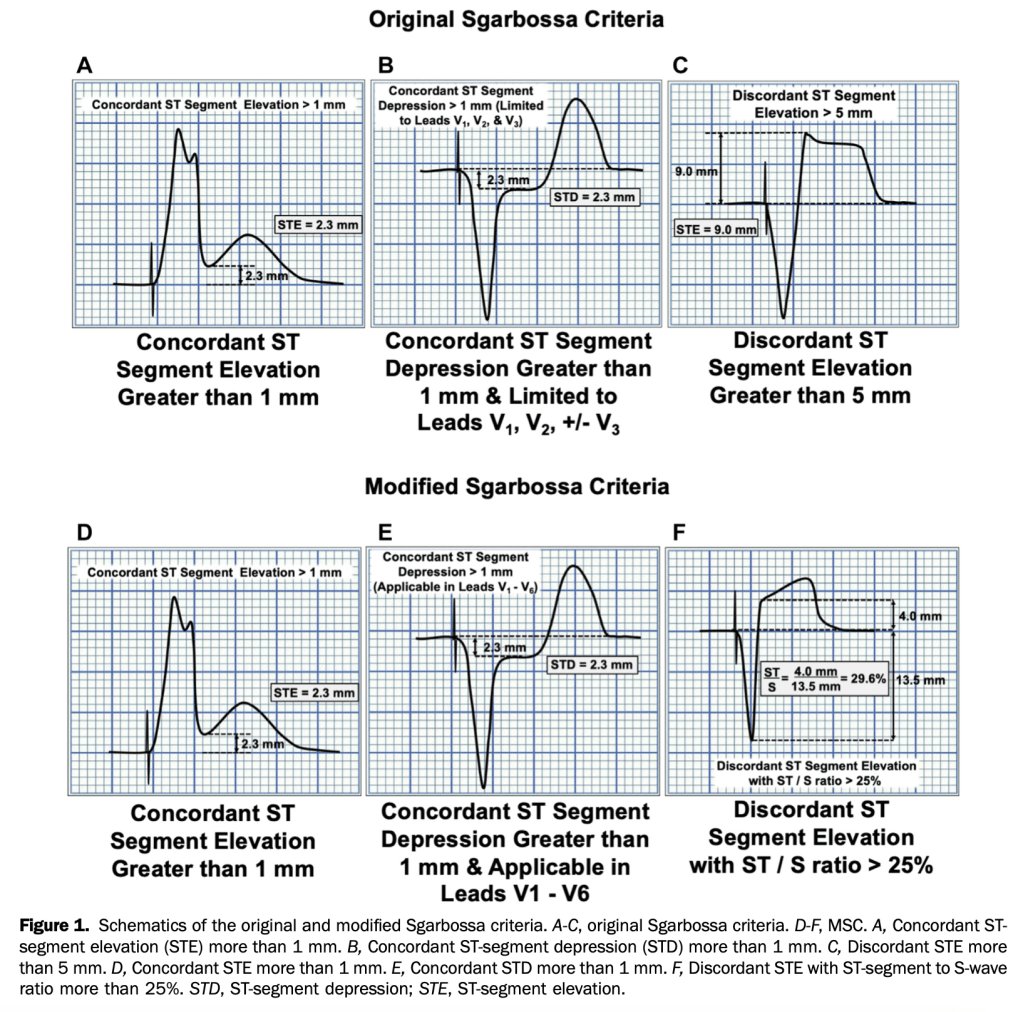
Annals of Emergency Medicine
- Modified Sgarbossa Criteria in LBBB- sensitivity was significantly higher than that of the original Sgarbossa criteria (91% versus 52% and 80% versus 49%, respectively; P<.001 for all) and high specificity was maintained (90% versus 98% and 99% versus 100%, respectively).
- This study showed MSC were more sensitive than the original Sgarbossa criteria; specificity was high for both rules. The MSC may contribute to clinical decisionmaking for patients with ventricular paced rhythm. [Ann Emerg Med. 2021;78:517-529.]
BMJ
- Etoricoxib 60 mg/day and diclofenac 150 mg/day seem to be the most effective oral NSAIDs for pain and function in patients with osteoarthritis. However, these treatments are probably not appropriate for patients with comorbidities or for long term use because of the slight increase in the risk of adverse events. Additionally, an increased risk of dropping out due to adverse events was found for diclofenac 150 mg/day. Topical diclofenac 70-81 mg/day seems to be effective and generally safer because of reduced systemic exposure and lower dose, and should be considered as first line pharmacological treatmentfor knee osteoarthritis. The clinical benefit of opioid treatment, regardless of preparation or dose, does not outweigh the harm it might cause in patients with osteoarthritis.
Acute urinary retention and risk of cancer: population based Danish cohort study
- CONCLUSIONS: Acute urinary retention might be a clinical marker for occult urogenital, colorectal, and neurological cancers. Occult cancer should possibly be considered in patients aged 50 years or older presenting with acute urinary retention and no obvious underlying cause.
- The absolute risk of prostate cancer after a first diagnosis of acute urinary retention was 5.1% (n=3198) at three months, 6.7% (n=4233) at one year, and 8.5% (n=5217) at five years. Within three months of follow-up, 218 excess cases of prostate cancer per 1000 person years were detected. An additional 21 excess cases per 1000 person years were detected during three to less than 12 months of follow-up, but beyond 12 months the excess risk was negligible.
Common intestinal stoma complaints
Circulation
None
EMCRIT
None
Emergency Medicine Journal
None
EMRAP
Pharmacology Rounds: Beers Criteria
- Avoid first antihistamines, second generation ok (loratadine)
- Nitrofurantoin (on the list bc not effective if cr cl<30, otherwise ok for short term)
- NSAIDS: incr cv and go complications, naproxen safest, safer than ibuprofen
- Antipsychotics: increased risk from prolonged use
Neutropenic Fever
- Fever: Temperature greater than 101ºF (38.3ºC) or sustained of 100.4ºF (38ºC) for at least an hour.
- Neutropenia: Absolute neutrophil count (ANC) < 1000 with an expected decrease to 500, or an ANC of < 500.
- The most common (and deadly) bacterial sources of infection are gram negative bac-teria. There is also a higher rate of resistant organisms and opportunistic infections.
- If there is no obvious source of infection, the work-up should include 2 blood cultures (1 from indwelling line, if present), liver function tests, bilirubin, chest x-ray (if upper or lower respiratory infectious symptoms), and respiratory viral panel.
- Administer empiric antibiotics as quickly as possible:
- Provide gram negative coverage with antipseudomonal activity: cefepime or a carbapenem if concern for ESBL.
- Piperacillin-tazobactam is another common choice.
- Vancomycin can be considered if an indwelling line is suspected to be the source of infection, or if they are hypotensive or toxic-appearing.
- Some patients may need fungal or viral coverage.
- Which patients can go home?
- Use MASCC calculator on MDCALC.
- This should only be done in consultation with oncology.
Watchman Procedure
- A cardiology procedure that eliminates the left atrial appendage, thus reducing the risk of clot formation in patients with atrial fibrillation (paroxysmal or chronic).
- Performed via percutaneous access through the femoral artery.
- Over approximately 45 days, the myocardium grows over the device that is placed in the appendage.
- Patients require anticoagulation for the first 45 days due to increased risk of thrombo-embolic disease, but do not require chronic anticoagulation.
- Watchman device versus systemic anticoagulation:
- Lower hemorrhagic stroke rate with the device. Lower cardiovascular mortality with the device. No difference in ischemic stroke rate.
- Overall complication rate: approximately 1-8% (most occurring immediately post-procedure). Cardiac perforation leading to tamponade.
JAMA
Comparison of New Pharmacologic Agents With Triptans for Treatment of Migraine
- For pain freedom or pain relief at 2 hours after the dose, lasmiditan, rimegepant, and ubrogepant were associated with higher ORs compared with placebo but lower ORs compared with most triptans. However, the lack of cardiovascular risks for these new classes of migraine-specific treatments may offer an alternative to triptans.
Effect of Vasopressin and Methylprednisolone vs Placebo on Return of Spontaneous Circulation in Patients With In-Hospital Cardiac Arrest: A Randomized Clinical Trial. (article not open access).
Association of Tramadol vs Codeine Prescription Dispensation With Mortality and Other Adverse Clinical Outcomes (no open access)
- Compared with codeine, tramadol dispensation was significantly associated with a higher risk of all-cause mortality (incidence, 13.00 vs 5.61 per 1000 person-years; HR, 2.31 [95% CI, 2.08-2.56]; ARD, 7.37 [95% CI, 6.09-8.78] per 1000 person-years), cardiovascular events (incidence, 10.03 vs 8.67 per 1000 person-years; HR, 1.15 [95% CI, 1.05-1.27]; ARD, 1.36 [95% CI, 0.45-2.36] per 1000 person-years), and fractures (incidence, 12.26 vs 8.13 per 1000 person-years; HR, 1.50 [95% CI, 1.37-1.65]; ARD, 4.10 [95% CI, 3.02-5.29] per 1000 person-years). No significant difference was observed for the risk of falls, delirium, constipation, opioid abuse/dependence, or sleep disorders.
J Am Geriatr Soc.
Effect of age on treatment outcomes in benign paroxysmal positional vertigo: A systematic review (no open access)
- Although more CRPs (Canalith Repositioning Procedures- Epley’s maneuvers) are needed, the rate of complete recovery in older adults is similar to that observed in younger adults.
Journal of Emergency Medicine
None
Lancet
- No benefit, increased mortality.
NEJM
Immediate versus Postponed Intervention for Infected Necrotizing Pancreatitis
- No difference if you wait until walled off.
Clinical Features of Vaccine-Induced Immune Thrombocytopenia and Thrombosis
PEDIATRICS
Recommendations for Prevention and Control of Influenza in Children, 2021–2022
REBELEM
REBEL Core Cast 66.0 – Congenital Cardiac Issues
- Once you figure out the neonate that presented to your ED is sick, run through a differential of why then can be sick so you don’t anchor. I like to use TIMOT (Trauma, Infection, Metabolic, Organs, Tox) but use whatever works for you.
- Use your detailed history looking for risk factors to help you narrow the differential down. Do a good hands-on physical exam. Work them up more than you would a standard baby and do things like you would to an adult such as a bedside US. These will all lead you to the diagnosis of a congenital cardiac disease
- You have two options now: they either have a cyanotic lesion that requires prostaglandins and a dose of 0.05-0.2 mg/kg/min and will need to be intubated. Or they are in full blown heart failure and require lasix at 1 mg/kg and pressors, typically a combination of dobutamine and norepinephrine.
- Don’t be a hero but don’t have imposter syndrome. You can manage these kids, but do so with support from your PICU, cardiac surgeon or transferring institution. What you are doing in the ED is temporizing to keep them alive to definitive therapy which is usually a combination of ECMO and/or surgery. Get them out of your department ASAP.
REBEL Cast Ep101: The TOMAHAWK Trial – Angiography after OHCA without STEMI
- Clinical Take Home Point: In hemodynamic and electrically stable patients with OHCA and no STEMI after ROSC, an immediate-angiography strategy does not appear to improve 30-day mortality. It appears that an approach of intensive care first followed by delayed angiography if clinically indicated is preferred.
The DisCoVeRy Trial: Remdesivir in COVID-19 – An Expensive Version of Tamiflu?
- Clinical Take Home Point: Although earlier trials showed a signal of benefit for remdesivir improving time to recovery, no trials have shown an improvement in mortality, a more important clinical outcome. Additionally, this is now the third trial showing no clinical benefit of remdesivir. The current evidence does not support the use of remdesivir in hospitalized patients with symptoms for more than 7 days and requiring oxygen support. This story sounds much like another antiviral medication used for another viral illness (i.e. Tamiflu for influenza), except this medication is much more expensive ($3k – 5k for a 5 day course).
Rebellion 21: Clap Back – Gonorrhea and Chlamydia Updates via Jenny Beck-Esmay, MD
- Testing:
- Male: 1st catch urine sample (Not a clean catch urine – midstream) as good as urethral swab
- Female:Vaginal swab as sensitive as cervical swab (Can be collected by the patient themselves)
- Urine: Needs to be 1st catch urine (Not a clean catch urine – midstream); Not as sensitive as vaginal or cervical swab
