Academic Emergency Medicine
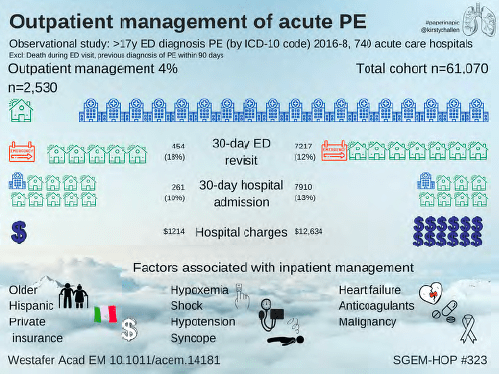
SGEM#323: Mama I’m comin’ home—For outpatient treatment of a pulmonary embolism
- @RozhenalMD : In my experience the limiting factor is often the fact that some insurance plans cover rivaroxaban and others cover apixaban, apparently none cover both. So it’s practically impossible to figure this out and send them home on a doac unless it’s 2 pm on a Tuesday. Hence, obs.
- Reply by author @LWestafer: We get around this with initial coupons. https://eliquis.com/eliquis/hcp/resources#panel- element-2… either 30d free or 10$ copay regardless of insurance- I tell patients they may get switched but this will get them started
Topiramate (Topamax) for migraine prophylaxis
- First line treatment per Uptodate
- Current dosing recommendations of topiramate for migraine prophylaxis approved by the FDA is to start at 25 mg a night for week 1, 25 mg twice a day for week 2, 25 mg in the morning and 50 mg in the evening on week 3, and finally 50 mg both morning and evening starting week 4.12 In patients with significant side effects, rapid discontinuation without tapering is favored.
- As of November 2020, a one-month supply of topiramate (50 mg twice daily) costs $9.00 to $11.81.
- Side effects: drowsy, dizzy, fatigue, also associated with long term and short cognitive dysfunction
American Journal of Emergency Medicine
Multisystem inflammatory syndrome in children with COVID-19 Review Article
High flow nasal cannula for adult acute hypoxemic respiratory failure in the ED setting
Annals of Emergency Medicine
- Of the 256 children, 58 (22.7%) had clinically important intussusception. POCUS identified 60 (23.4%) children with clinically important intussusception. The diagnostic accuracy of POCUS was 97.7% (95% confidence interval [CI] 94.9% to 99.0%), compared to 99.3% (95% CI 96.8% to 99.9%) for RADUS.
- According to this 1 hour YouTube lecture from AIUMultrasound, the study takes less than 2 minutes and requires minimal experience to perform.
United States Best Practice Guidelines for Primary Palliative Care in the Emergency Department
- If you would not be surprised if the patient was to die within the next year, consider a palliative care consult.
BMJ
None
Circulation
- In patients with acute chest pain and suspected ACS who are deemed low-risk (<1% 30-day risk of death or MACE), it is reasonable to discharge home without admission or urgent cardiac testing.
EMCRIT
- Introducer Sheath is in (If the patient NEEDS a pacemaker–an experienced person should put in the introducer)
- Position the Patient so you can see the monitor
- Put the damn sterile sheath on the wire
- Test the balloon (Special Syringe only allows 1.5 ml of air)
- Attach to wire extender to the box, the pacemaker pins and tighten!!!! (Write Negative=Distal on your Pacemaker Drawer)
- Have your partner set the box. Rate 2x intrinsic and V Output 20 mA
- attribution neededOrient the curve
- Advance to 15 cm
- Call for balloon up (Note be GENTLE with balloon inflation/and only passive deflation. Down until 1.3 cc)
- Advance somewhat rapidly until you see electrical capture (monitor shows big electrical spikes with lbbb morphology) then confirm mechanical capture by looking at rate of pulse ox or having someone check pulses or looking at ultrasound arterial pulse.
- Do the turn down dance
- Deflate Balloon/lock stopcock
- Secure by first clamping down on the wire then attaching down distal and clamping proximal portions of sheath and suture the introducer to the patient
- Hang box on IV pole
- Check Sensitivity Settings
- Get an Xray (RV placement will show the wire cross the midline)
- Place in VVI
Emergency Medicine Journal
None
EMRAP
Pediatric Pearls: Congenital Heart Disease Part 1
Cardiology Corner: Updates in SVT
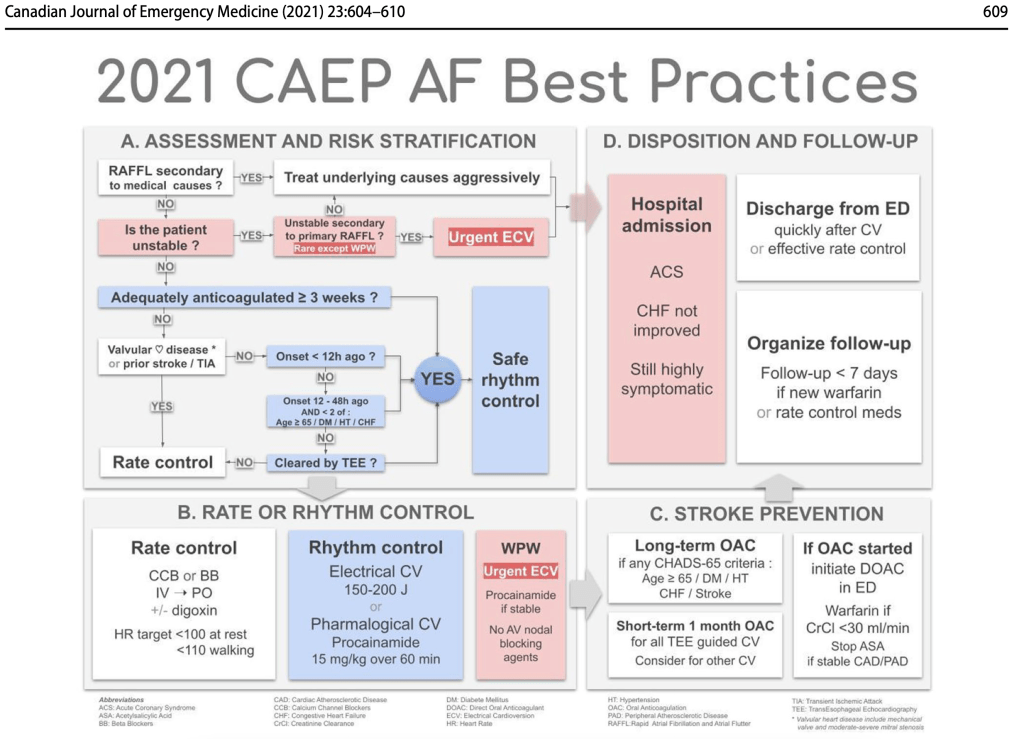
2021 CAEP (Ian Stiell) Atrial Fibrillation Algorithm
JAMA
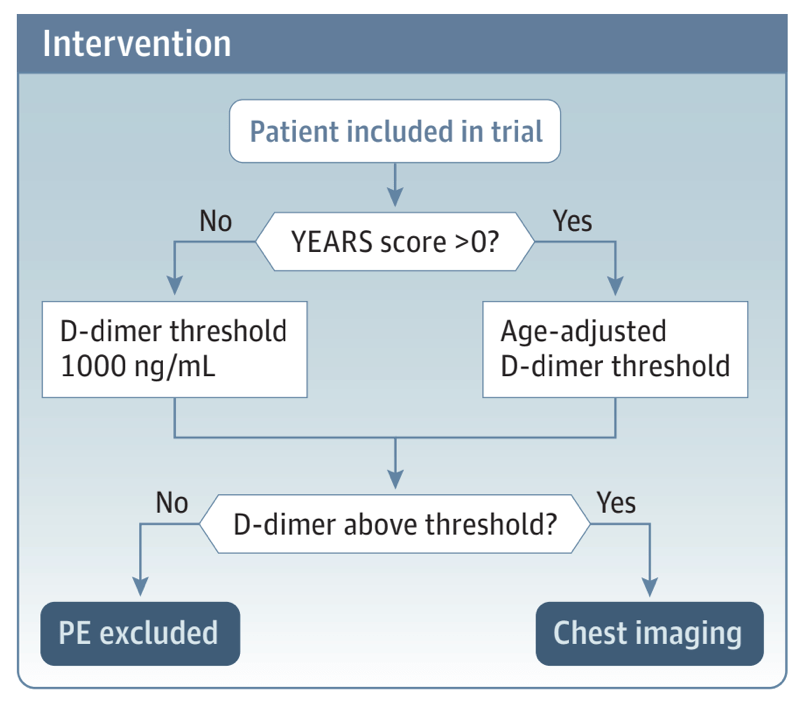
Diagnostic Strategies for Suspected Pulmonary Embolism- editorial
Journal of Emergency Medicine
None
Lancet
None
NEJM
A Randomized Trial of Intravenous Alteplase before Endovascular Treatment for Stroke
- tPA plus endovascular treatment no better than endovascular treatment alone
- In contrast to spontaneous bacterial peritonitis in patients with cirrhosis, which is diagnosed when the neutrophil count is 250 per μl or higher, peritoneal dialysis–related peritonitis is diagnosed with a white-cell count as low as 100 per μl if there are 50% or more neutrophils.
PEDIATRICS
Corticosteroids in the Treatment of Pediatric Retropharyngeal and Parapharyngeal Abscesses
- Retrospective study: Of the 2259 patients with RPAs and PPAs, 1677 (74.2%) were in the noncorticosteroid group and 582 (25.8%) were in the corticosteroid group. There were no significant differences in age, sex, or insurance status. There was a lower rate of drainage in the corticosteroid cohort (odds ratio: 0.28; confidence interval: 0.22–0.36). Patients in this group were more likely to have repeat computed tomography imaging performed, had lower hospital costs, and were less likely to have opioid medications administered. The corticosteroid cohort had a higher 7-day emergency department revisit rate, but there was no difference in length of stay (rate ratio 0.97; confidence interval: 0.92–1.02).
REBELEM
REBEL Core Cast 69.0 – Epiglottitis
- For patients with advanced inflammation, prophylactic intubation may be necessary. Involve consultants early for a possible awake intubation in the OR, and with preparations to convert to a surgical airway, if necessary.
REBEL Cast Ep104: VAM-IHCA – Vasopressin and Methylprednisolone for In-Hospital Cardiac Arrest
- Clinical Take Home Point: The combination of vasopressin and methylprednisolone compared to placebo during in-hospital cardiac arrest resulted in more ROSC but had no statistically significant difference in the more patient oriented outcomes of survival and survival with favorable neurologic status at 30 and 90d. In fact, survival at 30 days appeared to be worse in the VAM group. At this time, we cannot recommend the addition of vasopressin and methylprednisolone in the management of IHCA.

{kind=link}