Academic Emergency Medicine
None
American Journal of Emergency Medicine
None
Annals of Emergency Medicine
- aerosol dispersion length greatest for BiPAP (100 cm), followed by
- nasal cannula oxygenation with face coverings (86 cm)
- high-flow nasal cannulas with face coverings (67 cm)
- nonrebreather masks (63 cm)
- CPAP (47 cm)
Sexually Transmitted Infections Treatment Guidelines, 2021
BMJ
Fever therapy in febrile adults- systematic review with meta-analyses and trial sequential analyses
- Fever therapy does not seem to affect the risk of death and serious adverse events.
- Roughly 5% of Covid patients will lose their sense of taste or smell.
Circulation
None
EMCRIT
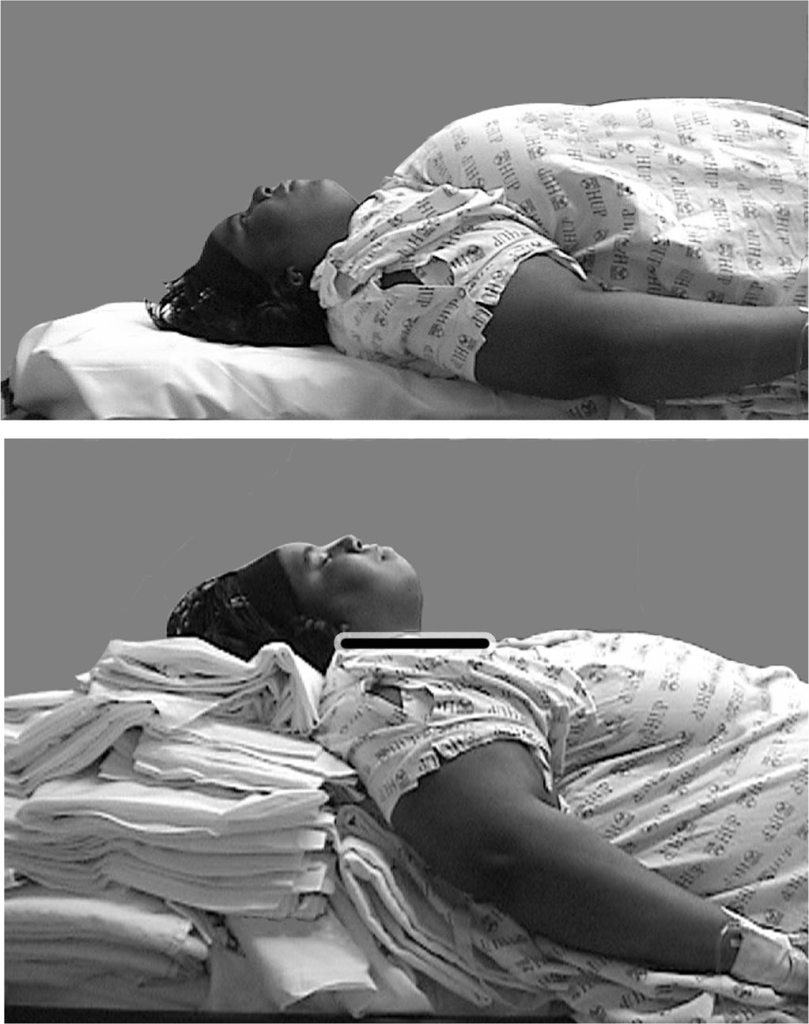
EMCrit 329 – Bariatric Critical Care and Resus Ready for the Super Obese Patient
- BP- can be falsely high because cuff is too small, can try calf but unknown if this is studied, Scott recommends an art line
- CPAP preox
- Positioning (see pics below): line up external auditory meatus with the sternal line not notch, meaning need to line up with the line from the sternal notch to diploid process.
- Avoid RSI in severely obese patients, DSI safer unless the patient is apneic.
- Intubation Meds
- Etomidate LBW LBW calculator
- Ketamine LBW
- Propofol TBW for drip
- Succinylcholine TBW
- Rocuronium- Some would say IBW, but Calvin Brown [UpToDate in the Biblio] and The EM Airway Course is recommending TBW–That is my rec as well
- DSI approach (per Scott): start with Ketamine 100mg and wait ten seconds, if patient not dissociated give more, this allows you to take a look, if intubation looks easy then redox and paralyze because DSI easier for looking then for passing a tube
- Post-intubation positioning- sitting up so pannus not preventing chest expansion
- Central line- neck or groin better, subclavian has no landmarks
PulmCrit – Myth-busting the conditional nephrotoxicity of piperacillin-tazobactam
- Piperacillin-tazobactam is not generally regarded as a nephrotoxin although it can rarely cause acute tubulointerstitial nephritis, an unusual allergic reaction seen with numerous antibiotics/other meds.
- Vancomycin is an actual nephrotoxin.
- Solution:
- Continue to use Piperacillin-tazobactam
- Avoid Vanco in non-MRSA situations (community acquired-urosepsis/intra-abdominal infections, non purulent cellulitis)
- Discontinue after 24-48 hours if negative MRSA nares PCR and negative blood culture)
- Dose Vanco carefully, monitor levels
- Consider Linezolid or Daptomycin over Vanco for patients at high risk of nephrotoxicity
Emergency Medicine Journal
None
EMRAP
Critical Care Mailbag: Critical Transfusions- Weingart
- Type is ABO group
- Screen evaluates if the patient has any of the common minor antibody groups (such as Rh, Kelly, Duffy).
- Crossmatch”: takes blood that matches the patient for both major and minor antibody groups and reserves it for the patient, essentially taking it out of the pool of available blood.
- Take Home #1: There is no need to routinely obtain Type + Cross on every patient who may need blood.
- If the patient screens “negative” for any minor antibody groups, crossmatch is unnecessary.
- If the patient needs immediate transfusion (eg, in the event of massive GI bleed or trauma with shock), you can transfuse without knowing the minor antibody groups.
- If the patient screens “positive” for minor antibody groups, crossmatch can be helpful in ensuring compatible blood is available.
- Take Home #2: Every hospital should have a system where the blood bank notifies the clinician when the patient screens positive for minor antibodies
- In this situation, taking a number of units out of circulation is important to ensure that when the patient with minor antibodies needs a transfusion, they have the right blood available.
MTP
- In most hospitals, massive transfusion protocol is the only way to rapidly get blood.
However, this approach is often more than is needed and can be wasteful as it utilizes a lot of resources and can shut the blood bank down to other patients. - Many bleeding patients will stabilize after 1-2 units making massive transfusion protocol unnecessary.
- An intermediate pack can be considered
These are immediate-release “universal donor” blood products. Scott recommends the pack consists of 2 units pRBCs and 2 units FFP.
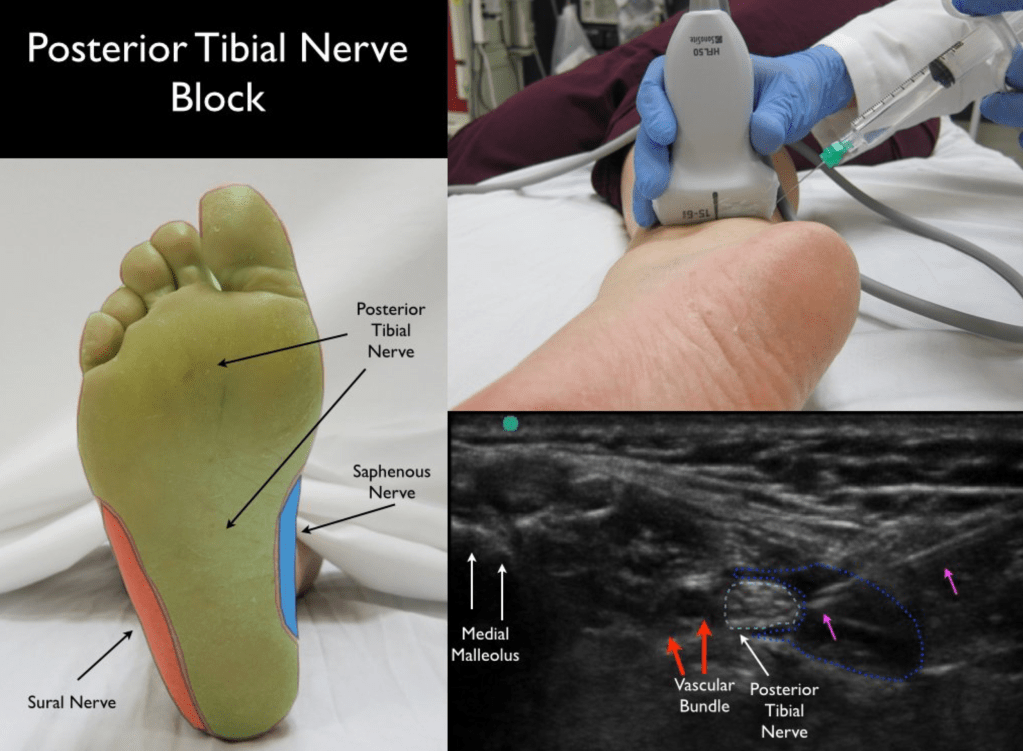
- Great video by Jacob Avila on how to perform this block for the sole of the foot.
- In addition to lacs and FBs, also good for calcaneus fractures.
- When to get MRI?
- Back pain plus fever
- Neuro deficits c/w cord compression
- New back pain plus risk factors (diabetes mellitus, HIV, cancer, renal disease, liver disease, dialysis or recurrent vascular access, alcoholism, IV drug use, immunocompromised, spinal instrumentation/surgery, older age)- order ESR and CRP, if either is high go to MRI, if both normal then workup can be concluded.
- What to MRI?
- Authors recommend MRI of the entire spine with contrast
Inflammatory Bowel Disease in the ED
- CT indicated if:
- Bowel obstruction
- Intra-abdominal sepsis
- Perianal sepsis
JAMA
- No benefit
Journal of Emergency Medicine
None
Lancet
None
NEJM
PEDIATRICS
None
REBELEM
Topical TXA in Atraumatic Anterior Epistaxis Yet Again
- Paper: Hosseinialhashemi M et al. Intranasal Topical Application of Tranexamic Acid in Atraumatic Anterior Epistaxis: A Double-Blind Randomized Clinical Trial. Ann Emerg Med 2022.
- Clinical Take Home Point: Based on this trial and the systematic review published in 2021 (Link is HERE), the fact that topical TXA is low cost, simple to use, and has no untoward effects it seems the best 1st line strategy in epistaxis is a TXA soaked pledget with direct pressure. It is unclear whether TXA has benefit in cases where compression with a topical vasoconstrictor fails.
REBEL Core Cast 85.0 – Superficial Venous Thrombosis
- Take Home Points
- SVT >5cm or ❤ cm from the SFJ (sapheno-femoral junction0 should be treated with anti-coagulation.
- The rate of concurrent DVT and PE in patients with SVT is 25% and 5%, respectively.
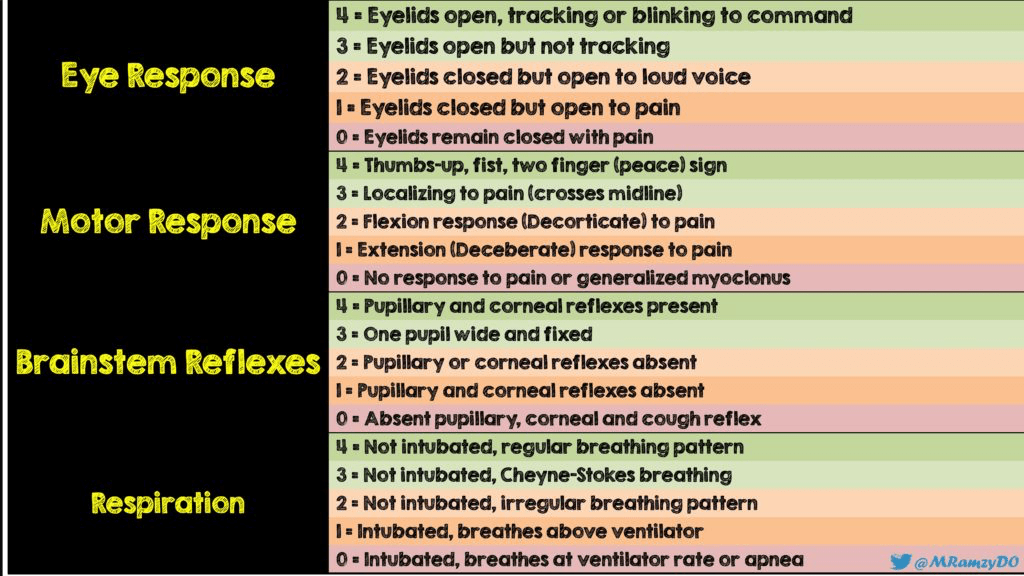
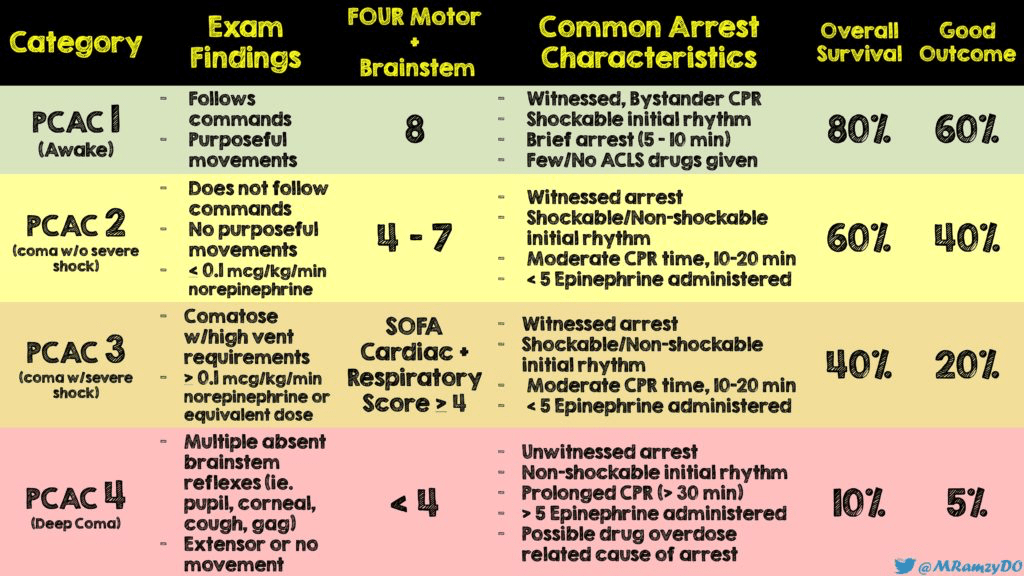
External Validation of Pittsburgh Cardiac Arrest Category (PCAC) Illness Severity Score
Resuscitation
Pulseless electrical activity in in-hospital cardiac arrest – A crossroad for decisions
- PEA is a crossroad in which the subsequent course is determined. The four distinct presentations of PEA behave differently on important characteristics. A transition to PEA during resuscitation should encourage the resuscitation team to continue resuscitative efforts.
