Annals of Emergency Medicine
Managing Emergency Endotracheal Intubation Utilizing a Bougie
Selecting Tube Size for Traumatic Thoracostomy
- After insertion, clinicians should monitor for signs warranting immediate operative intervention including initial drainage of more than 1500 mL and persistent drainage (150 to 200mL/h for 2 to 4 hours)
EMCRIT
EMCrit 393 – CV-EMCrit – Inotrope Basics Part 1 and 2
What Heart Rate to Shoot For?
90-110 in most patients (may go higher if compensating for RHF or extremely low EF)
The Inotropes
Dobutamine, the ChronoInotrope
Hits B1, B2 and at higher doses, alpha
Not as much vasodilation as milrinone, but a lot of chronotropy and the possibility of arrhythmia induction
Dose: 1-5 mcg/kg/min (can go up to 10, but you start risking excessive chronotropy)
Milrinone, the InoDilator
Phosphodiesterase-3 (PDE-3) inhibitor that increases cAMP levels in cardiac myocytes by inhibiting cAMP breakdown by the PDE-3 enzyme leading to increased availability of Ca
Inotropy, lusitropy, but not as much chronotropy. Also comes with vasodilation (arterial, venous, and pulmonary arterial)
Our Dose Recs: 0.125 – 0.25 mcg/kg/min (max out at 0.37 mcg/kg/min)
45 minutes to see effect, avoid in ED because of long half life and Epi can do most of what Milrinone does.
Inotropic Epinephrine, Dual-faced: the pure Inotrope/Inopressor
0.01-0.08 mcg/kg/min (for a 70 kg pt, this is 1-5 mcg/min)
Hits B1, B2, and at higher doses, Alpha
Digoxin, Original-G
Trina uses this in AF with RVR in patients with reduced EF
30-45 min before you see clinical effects after a bolus
Delayed clearance with renal dysfunction
125-250 mcg bolus, may repeat x 1, two hours after 1st dose
after those 2 boluses, you really need levels
Calcium, “God’s” Inotrope
Correct low ionized calcium, will improve inotropy and hypotension if ionized calcium is low.
Dopamine, Fool’s Inotrope
Just don’t do it, just don’t…
Specific Scenarios
Septic Shock
- Norepi
- Epi if need more inotropy- 0.01-0.08 mcg/kg/min (for a 70 kg pt, this is 1-5 mcg/min)
- Add Vaso if need more vasoconstriction .03-.04 units/min, add early bc an infusion without a loading dose may take 30 min to show effect
- If ionized calcium low, replace it, will give significant improvement in inotropy and blood pressure
- Serious
Cardiogenic Shock without hypotension
- Milrinone low dose
Cardiogenic Shock with hypotension
- Norepi
- Epi if need more inotropy- 0.01-0.08 mcg/kg/min (for a 70 kg pt, this is 1-5 mcg/min)
- If ionized calcium low, replace it, will give significant improvement in inotropy and blood pressure
Right Heart Failure (or PE induced RHF)
- Start with the vasopressor to protect coronary perfusion but
- Vaso .03-.04 units/min
- Epi 0.01-0.08 mcg/kg/min (for a 70 kg pt, this is 1-5 mcg/min)
- Norepi if you need more squeeze
Atrial Fibrillation with RVR and Shock (EMCRIT Episode 20 Feb12, 2010)
- Sync Cardioversion 200j Biphasic AP pads- usually won’t work so proceed to 2. Best sedative meds 5-7 mg Etomidate and 10-15 mg Ketamine.
- Screen for WPW (wide complex tachy 250-300, shock early shock often, light them up!
- Phenyephrine for MAP support without increasing HR
- Amiodarone 150mg bolus followed by infusion 1mg/min OR
- Diltiazem 2.5mg/min until HR<100 or you max out at 50mg
- Magnesium 2g IV over 20 minutes may repeat x 1 in 1 hour
Bradycardic Shock
- Initiate Medical and Electrical treatment arms simultaneously
- Transcutaneous pacing
- Atropine and Epinephrine
- Atropine 1mg
- Epinephrine drip or push dose
- Calcium 3g IV over 5-10min
- Isoproterenol great for bradycardia but very expensive so pharmacy may not carry it
- Dobutamine helps increase HR but may cause hypotension
Anaphylactic Shock
- IM Epi 0.5mg (not 0.3) Q5 min until you start the IV drip
- Clean Epi drip 5-20ug/min If No Clean Epi rapidly available then do dirty epi drip
- Dirty Epi drip Push 1mg in 1000cc NS and then run wide open which in a 18g IV is usually between 20-30ml/min or if you can set it on the pump it is 1ug/10ml/min which for a 10ug/min infusion is 600ml per hour.
- Decadron 10mg IV (no steroid taper necessary)
EMRAP
Urology Suite: Stone Cold Facts
Chris Reilly, MD, and Meghan Cooper, DO
Dr. Reilly and Dr. Cooper discuss the diagnosis and ED management of kidney stones.
Kidney Stones:
- Does size matter?
- Stones <5 mm have >90% chance of passing in 2-4 weeks.
- Stones 5-7mm have a 50%-60% chance of passing.
- Stones >7mm have a <30% chance of passing.
- Prior stone formers may be able to pass larger stones and have lesser symptoms.
- Hydronephrosis and obstruction may lead to pyelovenous backflow, increasing the chance of infection.
- Staghorn canaliculi act as a nidus for recurrent infections but do not necessarily increase the risk for sepsis.
- Nonsteroidal anti-inflammatory drugs (NSAIDs) are the preferred pain regimen and more effective than opiates.
- Imaging:
- In undifferentiated or sicker patients, computed tomography (CT) may be indicated.
- For well-appearing patients who appear to have uncomplicated kidney stones, it is reasonable to try expectant management for 2-3 weeks with strict return precautions.
- Renal ultrasound may rule out other pathology or show some features of kidney stones (eg, hydronephrosis, absence of ureteral jets)
- Lab testing has a limited role in diagnosis of kidney stones but may be helpful preoperatively or to assess underlying kidney function. Impaired kidney function is not an absolute indication for surgery unless there is a solitary kidney or bilateral obstruction.
- It is reasonable to consider outpatient management with antibiotics and strict return precautions for patients with a positive urinalysis and kidney stones if they are well-appearing and non-septic.
- Risky features for kidney stones that may warrant admission include pregnancy, immunosuppression, solitary kidney, renal dysfunction, or uncontrolled pain/nausea.
PEARL: Many patients with kidney stones can be managed as outpatients; the most important feature is clinical appearance as these patients can become quite septic.
Spinal Epidural Abscess
David Talan, MD
Dr. Dave Talan discusses the difficult and often missed diagnosis of spinal epidural abscess. This segment reviews the most common risk factors, imaging of choice, and antibiotic coverage for this elusive cause of back pain.
- Diagnosing spinal epidural abscess
- On average, it is diagnosed on the third ED visit.
- Only 10% of patients present with the classic triad of fever, back pain, and neurological deficits.
- Risk factors:
- Intravenous drug use
- Diabetes
- Transplant history
- Bacteremia
- Recent spinal procedure
- Spinal epidural abscesses affect the thoracic back more commonly than other causes of back pain; therefore, thoracic pain should raise your level of concern
- Erythrocyte sedimentation rate (ESR) is not specific and may not be sensitive in early infection.
- Order magnetic resonance imaging (MRI) with contrast of the whole spine given the frequency of skip lesions
- Prioritize transfer if MRI is unavailable at your institution.
- A CT myelogram relies on accuracy of locating the epidural abscess by history and exam.
- On average, it is diagnosed on the third ED visit.
- Treatment
- Draw blood cultures.
- Antibiotics:
- If septic, start empiric antibiotics that cover Staphylococcus and gram-negative bacteria, including Pseudomonas, with vancomycin and a broad-spectrum cephalosporin
- If the patient is being taken to the operating room immediately, you may defer antibiotics to allow neurosurgery to obtain an accurate intraoperative culture.
PEARL: Spinal epidural abscess is a difficult diagnosis that you will miss if you don’t know the risk factors. If suspicious, MRI with contrast is the diagnostic test of choice; CT myelogram is insufficient.
Pediatric ECGs
Whitney Johnson, MD, and Mimi Lu, MD
Dr. Whitney Johnson and Dr. Mimi Lu discuss pediatric ECGs and the approach to pediatric chest pain. This segment elucidates some pediatric ECG findings to be wary of and underlines important indications for ordering an ECG in children that you may not expect.
- When to get an ECG
- An ECG is often ordered reflexively by triage before seeing the patient.
- Have a low threshold; seeing more ECGs will help develop interpretation skills.
- Consider an ECG in patients with syncope, chest pain, dizziness, persistent unexplained tachycardia, recurrent febrile seizure, or epilepsy.
- Optimize the ECG by obtaining it after fever, pain, and anxiety are controlled.
- Interpreting Pediatric ECGs
- The vast majority of principles from adult ECGs can be applied to children 10 or older.
- When in doubt, use reference resources for normal values for age.
- Axis deviation
- Babies are born with a right axis that transitions to a normal axis at around 6 months of age.
- A right-deviated axis past 6 months may indicate right ventricular hypertrophy or congenital heart disease.
- P-waves should be upright
- Inverted P-waves may indicate an ectopic atrial tachycardia.
- T-wave inversions
- V1 should be upright for the first week of life before inverting.
- Failure to invert may indicate right ventricular hypertrophy.
- T-waves invert back to upright from 3-8 years of age and should not flip again.
- Compare to a previous ECG to determine level of concern.
- V1 should be upright for the first week of life before inverting.
- Narrow tachycardia is 1 of 3 things: supraventricular tachycardia (SVT), sinus tachycardia, or atrial flutter with 2:1 conduction.
- Arrhythmia
- Expand the rhythm strip or increase box lengths to uncover an arrhythmia.
- The most common arrhythmia is supraventricular atrioventricular reentrant tachycardia (AVRT).
- The vast majority of principles from adult ECGs can be applied to children 10 or older.
- Approach to Pediatric Chest Pain
- Age-appropriate questioning is key:
- Ask about decreased exercise intolerance, feeding intolerance, cyanosis with feeding, or failure to thrive.
- Consider myocarditis and ask about antecedent illness.
- Consider adding a troponin when the story does not make sense; eg, teens with chest pain in the middle of the night.
- Age-appropriate questioning is key:
PEARL: Have a low threshold to order an ECG in pediatric patients, especially in patients with syncope, chest pain, persistent unexplained tachycardia, or recurrent febrile seizure.
Critical Care Mailbag: All Things Vasopressin
Anand Swaminathan, MD, and Scott Weingart, MD
Dr. Swaminathan and Dr. Weingart discuss the mechanism, dosing, and administration of vasopressin in the ED. Their conversation covers which patients may benefit most from vasopressin and the potential future of vasopressin bolus to determine vasopressin responsiveness.
- Mechanism of Vasopressin
- Produced in the hypothalamus and secreted by the posterior pituitary in response to high sodium or low blood pressure
- Acts upon the 3 vasopressin receptors:
- V1 – Vasoconstriction
- V2 – Antidiuretic effect
- V3 – Adrenocorticotropic hormone release from the central nervous system
- Dosing of Vasopressin
- Single-agent dose is 0.01-0.06 units/minute.
- When combined with other agents, the maximum dose is 0.04 units/minute.
- Higher doses are associated with ischemic complications.
- Administration of Vasopressin
- Two common approaches for starting vasopressin drips:
- Add as a second-line pressor once the norepinephrine dose reaches an arbitrary threshold (0.2 μg/kg/minute or 10 μg/minute).
- Start simultaneously with norepinephrine in patients who have liver failure, who are taking an angiotensin-converting enzyme inhibitor or angiotensin receptor blocker (ACE/ARB), or who you estimate to have been septic for ~24 hours at the time of their presentation.
- There is no evidence showing the safety of vasopressin in peripheral lines.
- There is new evidence suggesting that responsiveness to a bolus of vasopressin can determine which patients will benefit from a vasopressin drip.
- Two common approaches for starting vasopressin drips:
PEARL: Consider early vasopressin administration in patients who may have vasopressin deficiency from liver failure, ACE/ARB use, or prolonged sepsis.
Ectopic Pregnancy Management
Dara Kass, MD, and Anand Swaminathan, MD
Summary: In the landscape of uncertain decision-making regarding early pregnancy and medical care, the onus falls heavily on ED physicians to deliver more holistic and complete care for these patients. Dr. Kass and Dr. Swaminathan discuss the diagnosis and management of ectopic pregnancy in the ED in our current political and legal climates.
Uncertain Landscape of Early Pregnancy Management
- The reality is that shared decision-making as to whether a pregnant patient wants to continue a pregnancy is not available to every patient across the nation.
- Can the patient get close follow-up ObGyn care? How fast can an ObGyn come to discuss methotrexate as a treatment option (if available)?
- States with restrictions on medical care have fewer ObGyns available for consultation, which puts a higher burden on ED physicians.
- Management and care of early pregnancy used to be relatively predictable but now, with legislative changes, things have become more unpredictable.
- ED physicians have to be sharper with our care, more informed, and very clear on what we are going to do.
How does the value of beta human chorionic gonadotropin (beta-hCG) influence care?
- The interpretation of an ultrasound in the context of beta-hCG value allows us to put the clinical picture together: is this an early intrauterine pregnancy (IUP)? A pregnancy of unknown location? An ectopic pregnancy?
- The American College of Obstetricians and Gynecologists (ACOG) states that a beta-hCG level up to 3,500 mIU/mL with no IUP has zero likelihood of being a viable pregnancy.
- It may not be an ectopic pregnancy but could be a non-viable IUP.
- With beta-hCG in a window from 2,000 to 4,000 mIU/mL with a possible IUP, ED physicians in New York State can discuss treatment options with patients, depending on whether the pregnancy is desired or not, in addition to discussing risks of possible ectopic pregnancy.
- Now, around the country, we are seeing that at beta-hCG levels <4,000 mIU/mL, patient choice is being removed.
- ED physicians are now being put in a position where that decision is being pushed to later in the pregnancy, which increases our responsibility to ensure better follow-up, better communication, and better engagement with our consultants, given that risk of adverse outcomes is higher.
- Beta-hCG <2000 mIU/mLwith no IUP = expectant management (repeat hCG, repeat ultrasound).
- Beta-hCG >4000 mIU/mLwith no IUP = non-viable pregnancy regardless of location; patient needs treatment because if it is an ectopic pregnancy and it ruptures, the outcomes can be disastrous.
- Beta-hCG 2000-4000 mIU/mL (gray area) = remote possibility to have viable pregnancy, so we consult ObGyn to discuss various options with patients depending on what state and ED the patient is in.
- We all need to make uniform decisions as emergency medicine physicians so that it is not just physicians in restricted states who are thinking about a new way to make these decisions.
Transvaginal Ultrasound
- If a patient has an IUP on ultrasound and hasn’t received assisted reproductive therapy, an ectopic pregnancy is functionally ruled out.
- The risk of heterotopic pregnancy without assisted reproductive care is very low. (1:10,000)
- If the patient is receiving assisted reproductive care, the risk of heterotopic pregnancy increases.
- If a patient has an unruptured ectopic pregnancy, consult an ObGyn, who will review images and hCG levels and decide whether to offer the patient methotrexate or surgery.
- These patients need additional laboratory testing and need to be admitted after administration of methotrexate to repeat beta-hCG and ensure levels are decreasing.
- Failure of beta-hCG to decrease after methotrexate will result in a surgical procedure.
- If beta-hCG is decreasing on days 4 and 7 after methotrexate administration, the patient should have a weekly ObGyn appointment to repeat beta-hCG levels until they are zero.
- In some environments in the country, that “weekly follow-up” may actually be an ED visit for a beta-hCG level because patients don’t have anywhere else to go for follow-up.
- Access to this type of ObGyn medical care is changing around the country, and it is our job to deliver essential care to these patients if they cannot obtain it elsewhere.
Methotrexate Contraindications
- Renal insufficiency, immunodeficiency, active pulmonary disease, peptic ulcer disease, hypersensitivity to methotrexate, heterotopic pregnancy with viable IUP, and patients who are breastfeeding
- Pregnancy contraindications include beta-hCG >5,000 mIU/mL or presence of fetal cardiac activity
Complications of Delaying Care
- From the standpoint of long-term complications, offering a patient methotrexate as a treatment modality for an ectopic pregnancy is different from offering a patient surgery.
- Abdominal surgery means the patient will lose a fallopian tube and will be admitted to the hospital for a period of time, and it can affect fertility.
- If we don’t act early or we delay care for our own legal protections, we limit our patient’s treatment options and can cause long-term complications.
- The medico-legal climate is changing surrounding ectopic pregnancy care and, unfortunately, by discharging a patient who has an untreated ectopic pregnancy, you may run the risk of an Emergency Medicine Treatment and Labor Act (EMTALA) violation.
Administration of Rhogam
- The new ACOG recommendations still recommend administration of Rhogam in a patient with an ectopic pregnancy who is Rh negative, actively bleeding, and at less than 12 weeks’ gestation.
- A patient who is not bleeding and who is terminating a pregnancy for whatever reason (including ectopic pregnancy and elective terminations) does not require Rhogam.
PEARL: The medicine of ectopic pregnancy management has not changed; rather, changes in access to medical care, unevenness of care, and the current political and legal landscape surrounding pregnancy termination are challenging us as emergency medicine physicians. The onus is on us to be our patients’ advocates in the different environments in which we encounter and treat these patients across the country.
First10EM
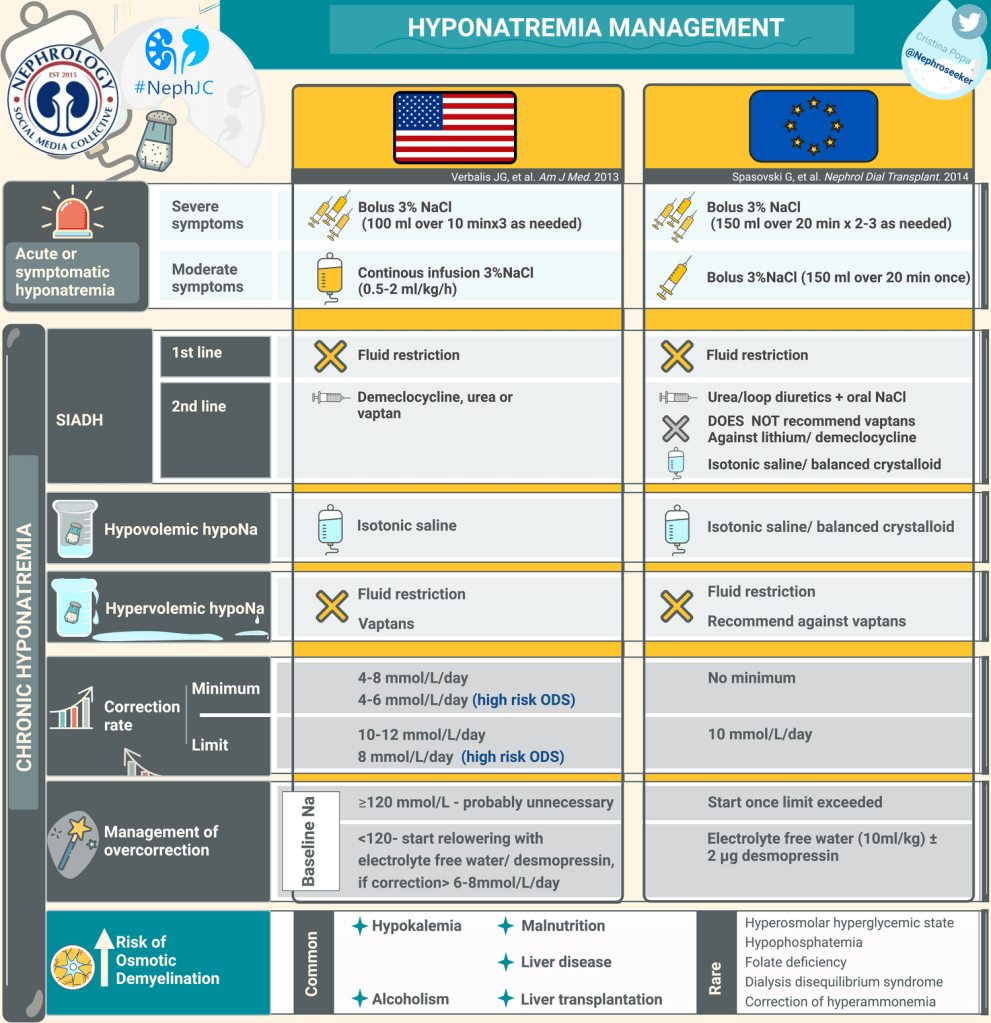
Hyponatremia: Are we all doing this wrong?
Ayus JC, Moritz ML, Fuentes NA, Mejia JR, Alfonso JM, Shin S, Fralick M, Ciapponi A. Correction Rates and Clinical Outcomes in Hospitalized Adults With Severe Hyponatremia: A Systematic Review and Meta-Analysis. JAMA Intern Med. 2024 Nov 18:e245981. doi: 10.1001/jamainternmed.2024.5981. PMID: 39556338
Bottom line: This meta-analysis of observational data shows an association between slower sodium correction in severe hyponatremia and increased mortality. These results are not definitive, but considering the rarity of demyelination, and the magnitude of the mortality results, this should probably influence clinical practice until we get the proper RCTs.
Nice graphic from the nephrology journal club as a nice overview of hyponatremia management:
NEJM
Medicaid on the Chopping Block
Heart Failure with Preserved Ejection Fraction
Striking a Balance — Advancing Physician
Identification and Treatment of Alcohol Use Disorder
REBELEM
Clinical Conundrum: Should Acute Asthma Exacerbations Be Discharged From the ED With Combination Beta Agonist/Corticosteroid Inhalers?
- Written by Steve Orellana DO,REBEL Core, REBEL EM
- Bottom Line: Current research suggests we should replace prescriptions for a SABA inhaler (i.e. albuterol) with a LABA-ICS combination inhaler as it can be used both for maintenance therapy and as a rescue inhaler. Furthermore, Budesonide + Formoterol is a safe patient-centered option that is at least as effective, if not better, than SABA alone. This change does not alter the recommendation of treating with a systemic steroid (ie dexamethasone, prednisone etc). The practice of discharging a patient with SABA inhalers alone should be ended.
- Prescription: Budesonide/formoterol 80/4.5 μg/puff, 1-2 puffs once to twice daily for maintenance, and then 1-2 puffs every 2-4 hours as needed for asthma symptoms, with instructions to go to the ED if more than that is required.
D-Dimer in High-Risk PE: A Gamble Worth Taking?
Author Conclusion: “In this study, ruling out pulmonary embolism in high-risk patients based on D-dimer below the age-adjusted threshold was safe, with no missed pulmonary embolism. However, the sample size was not large enough to draw a definitive conclusion on the safety of this strategy.”
Clinical Take Home Point: It may be reasonable to consider forgoing CTPA imaging in high-risk PE patients if they have a negative D-dimer, but more research that is prospective with larger cohorts is needed to determine the safety of this approach
