Annals of Emergency Medicine
- viral testing is costly and uncomfortable, and, for most patients, the gain in specificity rarely benefits subsequent testing or treatment decisions
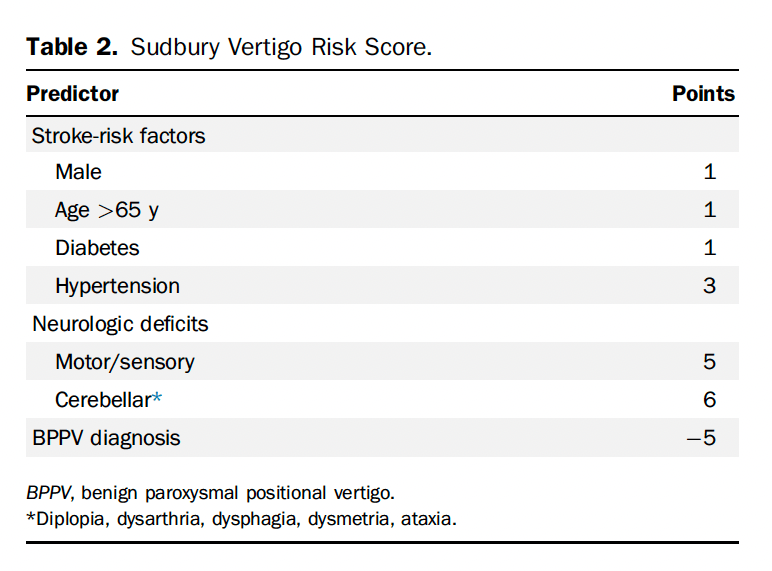
- Risk of a serious diagnosis was 0% if score is <5, 2.1% if the score is 5-8 and 41% if the score is >8.
- Not ready for prime time because it hasn’t been validated but seems promising.
Using the Osmolal Gap to Assess Toxic Alcohol Poisoning
- The osmolal gap should not be indiscriminately calculated in every patient with an anion gap metabolic acidosis. Acceptable test characteristics are predicated upon its application to a population with sufficient pretest probability of toxic alcohol exposure. For example, a history of possible toxin exposure, alcohol use disorder, prior suicide attempt, or at-risk occupation may inform clinician gestalt. Exclusion of alternative causes of anion gap acidosis such as alcoholic ketoacidosis also increases pretest probability. If the osmolal gap is elevated in a patient with sufficient pretest probability, treatment may be initiated; if not, and clinical suspicion remains high enough, the anion gap can be further trended to exclude toxic alcohol poisoning with normal osmolal gap.
The Osmolal Gap Has a Limited Role in the Evaluation of Possible Toxic Alcohol Poisoning
- The osmolal gap is an improper diagnostic aid for emergency physicians to use when evaluating an anion gap metabolic acidosis.
- Routine osmolal gap calculation in patients with anion gap metabolic acidosis with a goal to identify a small subset of patients with a toxic alcohol exposure would lead to the discovery of many elevated osmolal gap without an underlying toxicologic cause risking inappropriate resource allocation (eg, use of a costly antidote, interfacility transfer, hemodialysis), diagnostic confusion, and early diagnostic closure.
- A markedly increased osmolal gap, for example, more than 50 mOsm/L6 is more specific for a toxic alcohol ingestion; however, a progressive anion gap metabolic acidosis that does not improve despite treating other nontoxicologic causes will similarly identify the diagnosis.
- A superior diagnostic strategy to the osmolal gap involves meticulous history-taking, exclusion of alternative diagnoses, and frequent reassessment of patient response to resuscitation. Those patients with a worsening acidosis despite this strategy should be considered for treatments including alcohol dehydrogenase blockade and potentially hemodialysis while awaiting definitive laboratory testing.
- EDITOR’S NOTE: pro and con make good points, my personal approach will be to call poison control if I am suspicious based on history or severe unexplained gap acidosis or worsening acidosis despite standard resuscitation.
CJEM
Adding YEARS to optimize emergency department pulmonary embolism diagnostic workup
- researchers have shown that the YEARS criteria, a clinical decision rule, improves the efficiency of ruling out pulmonary embolism (without imaging) without compromising safety.
EMCRIT
Small Bore for Hemothorax
<=14 F was as good as the big boys in this MA/SR
Lyons, Nicole B., Mohamed O. Abdelhamid, Brianna L. Collie, Walter A. Ramsey, Christopher F. O’Neil, Jessica M. Delamater, Michael D. Cobler-Lichter, et al. “Small versus Large-Bore Thoracostomy for Traumatic Hemothorax: A Systematic Review and Meta-Analysis.” The Journal of Trauma and Acute Care Surgery 97, no. 4 (October 1, 2024): 631–38. https://doi.org/10.1097/TA.0000000000004412.PLT Transfusion before CVC
Platelet Transfusion before Central Line
- Van Baarle, Floor L.F., Emma K. Van De Weerdt, Walter J.F.M. Van Der Velden, Roelof A. Ruiterkamp, Pieter R. Tuinman, Paula F. Ypma, Walter M. Van Den Bergh, et al. “Platelet Transfusion before CVC Placement in Patients with Thrombocytopenia.” New England Journal of Medicine 388, no. 21 (May 25, 2023): 1956–65. https://doi.org/10.1056/NEJMoa2214322.
HypoK doesn’t equal HypoMag
- Tuttle, Ashley, Scott Fitter, Henry Hua, and Kayvan Moussavi. “The Effects of Magnesium Coadminstration During Treatment of Hypokalemia in the Emergency Department.” The Journal of Emergency Medicine 63, no. 3 (September 2022): 399–413. https://doi.org/10.1016/j.jemermed.2022.06.007.
EMCrit 393 – CV-EMCrit – Inotrope Basics Part 1
EMCrit 394 – CV-EMCrit – Inotrope Basics Part 2 – Specific Scenarios
Specific Scenarios
Septic Shock
- Norepi
- Epi if need more inotropy- 0.01-0.08 mcg/kg/min (for a 70 kg pt, this is 1-5 mcg/min)
- Add Vasopressin if need more vasoconstriction .03-.04 units/min, add early bc an infusion without a loading dose may take 30 min to show effect
- If ionized calcium low, replace it, will give significant improvement in inotropy and blood pressure
Cardiogenic Shock without hypotension
- Milrinone low dose (Phosphodiesterase-3 (PDE-3) inhibitor that increases cAMP levels in cardiac myocytes by inhibiting cAMP breakdown by the PDE-3 enzyme leading to increased availability of Ca)
- Inotropy, lusitropy, but not as much chronotropy. Also comes with vasodilation (arterial, venous, and pulmonary arterial)
- Our Dose Recs
- 0.125 – 0.25 mcg/kg/min (max out at 0.37 mcg/kg/min)
- 45 minutes to really see clinical effects
- DO NOT GIVE THE BOLUS
- titrate every 45-60 minutes
- 2.5 hr clinical half life, but at least doubled with renal failure and in a pt on RRT can be 20 hours
- can consider in a patient who is strongly beta-blocked
Cardiogenic Shock with hypotension
- Norepi first grab (need to protect MAP for coronary perfusion)
- Epi if need more inotropy- 0.01-0.06 mcg/kg/min (for a 70 kg pt, this is 1-5 mcg/min)
- If ionized calcium low, replace it, will give significant improvement in inotropy and blood pressure
Right Heart Failure (or PE induced RHF)
- Start with the vasopressor to protect coronary perfusion but use vasopressin not levo
- Vaso .03-.04 units/min
- Epi 0.01-0.08 mcg/kg/min (for a 70 kg pt, this is 1-5 mcg/min)
- Norepi if you need more vaso squeeze
Atrial Fibrillation with RVR and Shock (EMCRIT Episode 20 Feb12, 2010)
- Sync Cardioversion 200j Biphasic AP pads- usually won’t work so proceed to 2. Best sedative meds 5-7 mg Etomidate and 10-15 mg Ketamine.
- Screen for WPW (wide complex tachy 250-300, shock early shock often, light them up!
- Amiodarone 150mg bolus followed by infusion 1mg/min OR
- Diltiazem 2.5mg/min until HR<100 or you max out at 50mg
- Magnesium 2g IV over 20 minutes may repeat x 1 in 1 hour
Bradycardic Shock
- Initiate Medical and Electrical treatment arms simultaneously
- Transcutaneous pacing
- Atropine and Epinephrine
- Atropine 1mg
- Epinephrine drip or push dose
- Calcium 3g IV over 5-10min
- Isoproterenol great for bradycardia but very expensive so pharmacy may not carry it
- Dobutamine helps increase HR but may cause hypotension
- IM Epi 0.5mg (not 0.3) Q5 min until you start the IV drip
- Clean Epi drip 5-20ug/min If No Clean Epi rapidly available then do dirty epi drip
- Dirty Epi drip Push 1mg in 1000cc NS and then run wide open (18g IV is 20-30ml/min or on the pump 1ug/10ml/min which for a 10ug/min infusion is 600ml per hour.
- Decadron 10mg IV (no steroid taper necessary)
EMRAP
Crit Bits: Pulse Checks
Haney Mallemat, MD, and Anand Swaminathan, MD
Discussion: Swami and Haney Mallemat discuss the utility of using manual palpation during pulse checks. Is manual palpation reliable? Should we be using ultrasound during resuscitation efforts? If so, how can we do this effectively? Listen as they answer these questions and provide tips on how to improve your skills for these high-stress cases.
Key Points:
The Data on Pulse Checks:
- Manual palpation for pulse is often inaccurate and misleading.
- You may feel a pulse when none exists or fail to feel one that is present.
- Checks delay chest compressions.
- Pulses felt may not actually mean that perfusion pressure is adequate to perfuse the brain or other vital organs.
- A pulse does not tell you if there is tamponade, right ventricle enlargement, or left ventricle dysfunction.
Alternatives to Manual Pulse Checks:
- A femoral arterial line provides systolic, diastolic, and mean arterial pressures.
- Arterial lines provide instant assessment for pulsatile flow during rhythm checks.
- Quantitative end-tidal CO2 estimates perfusion post-return of spontaneous circulation (ROSC) but may not be reliable if the code has been running for a long time.
- Advantages of ultrasound use:
- Bedside echo evaluates cardiac activity; if no activity is seen, then start compressions sooner.
- May find reversible cause.
- Linear probes can be used to visualize carotid and femoral arteries and look for pulsations. Studies have found this to be more accurate for finding pulse. Can add echo pulse wave Doppler to estimate systolic BP.
Ultrasound during cardiac arrest:
- Don’t screw around with the ultrasound during cardiac arrest. Get windows quickly.
- If the first rhythm check shows ventricular fibrillation or ventricular tachycardia (Vfib/Vtach), DO NOT place the probe on the chest. Provide shock!
- If rhythm check shows pulseless electrical activity (PEA) or asystole, then use the ultrasound probe to look for contractility or reversible causes.
- May see fine Vfib on the bedside echo. This would be an indication to shock.
- If bedside echo shows organized cardiac activity; then use end-tidal CO2 and pulse wave Doppler to look for systemic perfusion. Studies show that a peak systolic velocity >20 cm per second correlates to a systolic BP of 60 mmHg.
- Once you find that you have a nonshockable rhythm and reversible causes have been excluded, transition to only using the pulse wave Doppler to look for arterial pulsatility during pulse checks.
- Do not interpret videos during pulse checks. Save clips and interpret during active compressions.
PEARL: It’s time to stop using our fingers for manual palpation during pulse checks. We can improve our resuscitation efforts and skills by working on our ultrasound proficiency. Learning how to properly implement ultrasound use during a code can result in improved CPR, decreased pauses, and faster identification of reversible causes.
Neurocritical Care Mailbag: Central Retinal Artery Occlusion (CRAO)
Anand Swaminathan, MD, and Evie Marcolini, MD
Central Retinal Artery Occlusion (CRAO)
- Anatomy: Internal carotid artery ➡ ophthalmic artery ➡ central retinal artery (supplies inner retina)
- About one-third of people have a cilioretinal artery that supplies the fovea and they may still have preserved central vision.
- Sudden painless monocular vision loss (often only able to count fingers)
- May be preceded by amaurosis fugax
- Differential diagnosis for abrupt change in vision: CRAO, central retinal vein occlusion (CRVO), retinal detachment, vitreous hemorrhage, glaucoma
- Risk factors: carotid stenosis, atrial fibrillation, hypertension, hyperlipidemia, diabetes mellitus, atherosclerosis
- Most commonly secondary to embolic phenomena
- Exam: Afferent pupillary defect (APD), profound vision loss, retinal whitening, cherry red spot (choroidal preservation), boxcarring of retinal arteries; normal extraocular motion, normal pressures, normal anterior chamber
- Ultrasound can be used to rule out retinal detachment and vitreous hemorrhage but cannot make the diagnosis of CRAO.
- The diagnosis of CRAO relies on a fundoscopic exam and benefits from a dilated exam.
- Labs: Order CBC, coagulation panel, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), and pregnancy test.
- If concerned for CRAO, treat it like a stroke, get last known well time (LKWT), and order CT angiography of head and neck. Reach out to ophthalmology and or vascular neurology and transfer if needed.
Treatment:
- There is no great randomized evidence. Retrospective data show a 50% recovery with the use of thrombolytics for CRAO within 4.5 hours from onset.
- There is an increase in recovery in patients treated with thrombolysis.
- Five patients had bleeding events but none in patients that received alteplase.
- Screen for arteritic CRAO: the obstruction is caused by calcium/cholesterol and does not respond to lytics.
- This is more likely in elderly patients, those with claudication symptoms or scalp/neck pain, or those with elevated ESR/CRP.
- Treatments without supporting evidence include ocular massage, anterior chamber paracentesis, and hemodilution.
- Hyperbaric therapy will improve oxygenation of the retinal tissues, increasing passive choroidal tissue oxygenation from 50% to >90%.
PEARL: CRAO presents as an abrupt profound change in vision and should be treated similarly to a stroke of the eye.
SummaryConversation (2)CME Credits (2)
Rabies
Sean Nordt, MD, and Sheema Shah, MD
Dr. Nordt and Dr. Shah discuss the transmission, symptoms, treatment, and prevention of rabies.
Background
- Rabies is a zoonotic neurotropic virus that is uniformly fatal.
- The incubation period for the virus is 4-12 weeks.
- Timely vaccination and immunoglobulin administration prevent transmission.
Epidemiology
- United States: Fewer than 10 deaths annually
- Globally: Approximately 59,000 deaths, primarily in children
- Most common vectors in the US:
- East coast: Raccoons
- Midwest and West coast: Skunks
- Southwest: Gray foxes
- Nationwide: Bats (unique because indirect exposure may require prophylaxis)
- Domestic animals like dogs, cats, and ferrets rarely carry rabies in the US but this varies globally.
Transmission
- Transmitted through bites, scratches, or mucosal contact.
- Pearl: Bats can transmit rabies through mucosal contact alone, so being in the same room as a bat without a bite may constitute a potential exposure.
- Risk factors:
- Location of bite: Proximity to brain increases risk.
- Animal behavior: Unprovoked bites carry higher risk.
Symptoms
- Initial symptoms: Flu-like illness, possible paresthesias at bite site
- Progressing symptoms: Personality changes, swallowing difficulty, hydrophobia, encephalitis
- Rabies is nearly always fatal once the patient is symptomatic.
Prevention and post-exposure prophylaxis:
- Incubation period of 4-12 weeks allows time for intervention.
- Immediate steps after exposure:
- Thorough wound cleaning with copious water and antiseptic such as chlorhexidine or betadine.
- Administer human rabies immunoglobulin (HRIG) at wound site. Administer any leftover volume at a distant site.
- Begin vaccination at day 0, followed by days 3, 7, and 14.
- Additional considerations:
- Previously vaccinated individuals do not receive HRIG and follow a modified vaccine booster schedule.
- Remember TDaP (tetanus, diphtheria, and acellular pertussis) and antibiotic prophylaxis if indicated as well.
- Be proactive with prophylaxis in uncertain cases due to the high stakes of untreated rabies.
Public Health Considerations:
- Review your local public health department’s guidelines.
- A link to the San Diego Health Services Rabies PEP algorithm is included below for reference.
- Report animal bites to your public health department.
- If possible, the animal should be observed for behavioral changes to help determine the need for further interventions and treatment.
- Understand your local rabies vectors and risk factors to guide decisions on prophylaxis.
- Maintain awareness of international exposures to ensure timely intervention upon return.
PEARL: Understand the risk factors for rabies transmission based on your local public health guidelines and initiate prompt post-exposure prophylaxis when indicated.
Pediatric Pearls: Blood Cultures
Ilene Claudius, MD; Loren Miller, MD; and Felice Adler-Shohet, MD
Discussion: Listen as our experts discuss the clinical implications of positive blood cultures, urine cultures, and strep PCR (polymerase chain reaction test) vs throat cultures. How should we interpret these and what steps need to be taken when informed of a positive culture in a patient who has been discharged?
Key Points:
- Order blood cultures only when necessary; false positives are common and they can lead to unnecessary repeat visits, admissions, and overuse of antibiotics.
- Current recommendations do not support ordering a set of blood cultures in febrile patients aged 3-36 months if they are
- Well appearing
- Up to date with vaccinations
- Without significant comorbidities
- If you are called about a positive blood culture, it is important to distinguish between pathogens and contaminants:
- Pathogens include Staphylococcus aureus, group A Streptococcus, group B Streptococcus, Streptococcus pneumoniae, Listeria, Clostridium species, Candida, Cryptococcus, Escherichia coli, Klebsiella, Proteus, Pseudomonas, Haemophilus influenzae, Gonorrhea, and Neisseria meningitidis.
- Contaminants include coagulase-negative Staphylococcus, Staphylococcus hominis, Staphylococcus epidermidis, Carnobacterium, diphtheroids, and Bacillus species.
- Take caution with patients with intravascular/recent endovascular devices. Bacteria that are considered contaminants can actually be clinically significant and lead to serious morbidity and mortality.
- If patients are immunocompetent with a fever plus viral symptoms, and blood cultures are positive with commoncontaminant bacteria, then it is more likely a viral syndrome. Give return precautions but it is likely that fever is not secondary to contaminant.
- Positive blood cultures require consideration of patient symptoms and history before deciding to treat or instructing patients to return for re-evaluation/treatment.
- If a blood culture is positive for Staph aureus, the patient must come back for re-evaluation and further workup. Staph aureuscan lead to serious complications such as osteomyelitis and psoas muscle abscesses, and can be difficult to treat.
- Do not order urine cultures unless clinically indicated. Clinical symptoms should be consistent with diagnosis and workup. Older patients are usually colonized and have asymptomatic bacteriuria.
- Patients aged 3 months to 1 year should have a urine culture ordered if they have a positive urinalysis.
- PCR tests for strep throat are more sensitive than throat cultures; treatment for strep throat is indicated if the PCR test is positive.
- Avoid unnecessary throat cultures in patients with viral syndromes.
PEARL: Remember to follow best practices for blood culture collection and interpretation. Don’t order blood cultures in fully vaccinated febrile children >3 months who are well appearing. Know your contaminants and pathogens in positive cultures. Oral antibiotics may be sufficient for most infections in noncritically ill patients. Older patients are colonized and have asymptomatic bacteriuria, so don’t work up urinary tract infections in these patients unless you have a high clinical suspicion or the patient is symptomatic.
Critical Care Mailbag: February Hodgepodge
Anand Swaminathan, MD, and Scott Weingart, MD
ED referrals:
- There are ethical implications of advising patients to visit the ED to bypass long appointment wait times.
- Scott recommends using the line “I wish that things were otherwise,” meaning “I wish things were otherwise, but I am unable to expedite your appointment from the emergency department.”
- There is potential for systemic abuse if patients learn they can do this.
- Helping individual patients may encourage misuse of ED resources.
Non-invasive BP measurement:
- Non-invasive cuffs are generally accurate, although arterial lines are preferred for critically ill patients.
- The systolic, diastolic, and mean arterial pressures are accurate in noncritically ill patients. All of the values are taken from the oscillatory wave pattern that the BP cuff measures.
- In the prior segment, Haney was focused on critically ill patients.
- Non-invasive BP cuffs can be misleading in patients with low perfusion states or in severely bradycardic patients with pulse rates <40.
Ketamine use in ethanol withdrawal:
- NMDA activity is upregulated in chronic ethanol (EtOH) abusers and has a role in EtOH withdrawal. Ketamine blocks excess NMDA activity.
- Despite mechanistic rationale, more robust clinical evidence is needed because this is not standard care.
- Phenobarbital and benzodiazepines are standard of care at this time. Studies using ketamine against standard care are lacking.
- Current data are in intensive care unit (ICU) patients who are on ketamine infusions, which is not applicable to the ED or to the EtOH withdrawal patient we typically encounter in our setting.
Hypoglycemia in cardiac arrest:
- Should hypoglycemia be treated as a reversible cause of cardiac arrest?
- In 2010, hypoglycemia was removed as a reversible cause of cardiac arrest by the American Heart Association (AHA).
- It should be noted that hypoglycemia can cause arrhythmias that cannot be improved with antidysrhythmics without first addressing the hypoglycemia.
- Hypoglycemia is likely present before arrest and likely contributes. It is unknown whether hypoglycemia can cause cardiac arrest, but keep it on your differential as a potential reversible cause.
What is the utility of midodrine in septic shock?
- The MIDAS trial in 2020 showed no benefit of using midodrine to wean ICU patients off norepinephrine.
- It has a potential role in cirrhosis with hepatorenal syndrome.
- There is no indication for midodrine use in the ED.
DKA: Columnar insulin protocol
- Columnar insulin protocol is a titration of insulin drip based on the glucose level instead of anion gap (AGAP) and ketone clearance.
- It has been found to delay resolution of diabetic ketoacidosis (DKA) by focusing on glucose rather than anion gap.
- Columnar protocols may be more effective in hyperosmolar hyperglycemic state (HHS) to allow for continued progression but not steep declines in glucose.
- Keep an eye out for the implementation of artificial intelligence in DKA management in the coming years.
PEARL: Swami and Scott discuss a variety of topics in this month’s mailbag. At this time, the jury is out on ketamine use for alcohol withdrawal. There is no indication for midodrine use as a vasopressor in the ED. The columnar insulin protocol delays DKA resolution, and may be more effective when used in HHS. And finally, remember to refer patients appropriately to their outpatient specialist to prevent abuse of our medical system.
Radioactive Materials
Nick Studer, MD, and Anand Swaminathan, MD
Dr. Studer and Dr. Swaminathan discuss the basics of radiation exposure and how to begin treatment and care for affected patients in the emergency setting.
- Radioactive material emits 3 types of radiation: alpha, beta, and gamma radiation.
- Alpha and beta particles are large particles that can damage or burn tissue if in direct contact but cannot penetrate clothing.
- Gamma radiation is high-energy electromagnetic radiation that can penetrate clothing and cause tissue damage.
- Exposure to a radioactive source can be in the form of direct contact, inhalation, or ingestion. The source will continue to emit radiation until removed with decontamination.
- Radiation exposure is very rare; exposures typically occur from industrial work accidents, terrorist attacks, or war.
- First responders will typically be able to tell you that there was radiation exposure at the site.
- “Exposure” means an individual was near radioactive material and, as they move away from the source, they are no longer exposed and are not a risk to others.
- “Contamination” means an individual has radioactive material (eg, dust, particles) on them or that they inhaled or ingested material. This material will continue to emit radiation to the patient as well as others they come in contact with. These patients require prompt decontamination.
- To date, no US physician has been harmed by radiation contamination or exposure.
- Personal protective equipment (PPE): Use droplet precautions including gowns/jumpsuits and N95 masks, controlled air purifying respirators (CAPRs), or powered air purifying respirators (PAPRs) to minimize contamination. Unfortunately, radiation suits do not exist.
- Acute radiation syndrome:
- First symptoms include headache, nausea, and vomiting, followed by a latent period.
- Higher doses of radiation lead to faster symptom onset. The time to nausea/vomiting can be used to predict the dose of exposure.
- A CBC with differential should be collected early; the lymphocyte count can be used to predict the dose of exposure and can be trended.
- Initial treatment is supportive care and rehydration.
- REAC/TS: 865-576-1005 has a nurse, physicist, and physician on call 24/7 to help assist with care and locating resources to aid in the treatment of patients with radiation exposure.
- Review your hospital’s disaster preparedness protocols and familiarize yourself with their plans for decontamination in an emergency setting.
PEARL: The most important first step in treating patients exposed to radiation is decontamination; the REAC/TS hotline is available 24/7 for assistance.
First10EM
Diltiazem for atrial fibrillation: does calcium pretreatment help?
- This is a well done, blinded RCT that demonstrates that prophylaxis with calcium in atrial fibrillation patients being treated with diltiazem might result in statistically higher blood pressures, but doesn’t seem to have much of a clinically important impact.
NEJM
REBELEM
Clinical Conundrum: Do I Have to Replace the Nail After an Avulsion?
- Bottom Line: Despite the classic teaching, the best available evidence doesn’t show a cosmetic difference between replacing the nail and not replacing the nail in pediatric patients. You would be well supported by the data if you chose to skip nail replacement.
