Academic Emergency Medicine
Annals of Emergency Medicine
Midazolam and Ketamine for Convulsive Status Epilepticus in the Out-of-Hospital Setting
ECG Patterns of Occlusion Myocardial Infarction: A Narrative Review
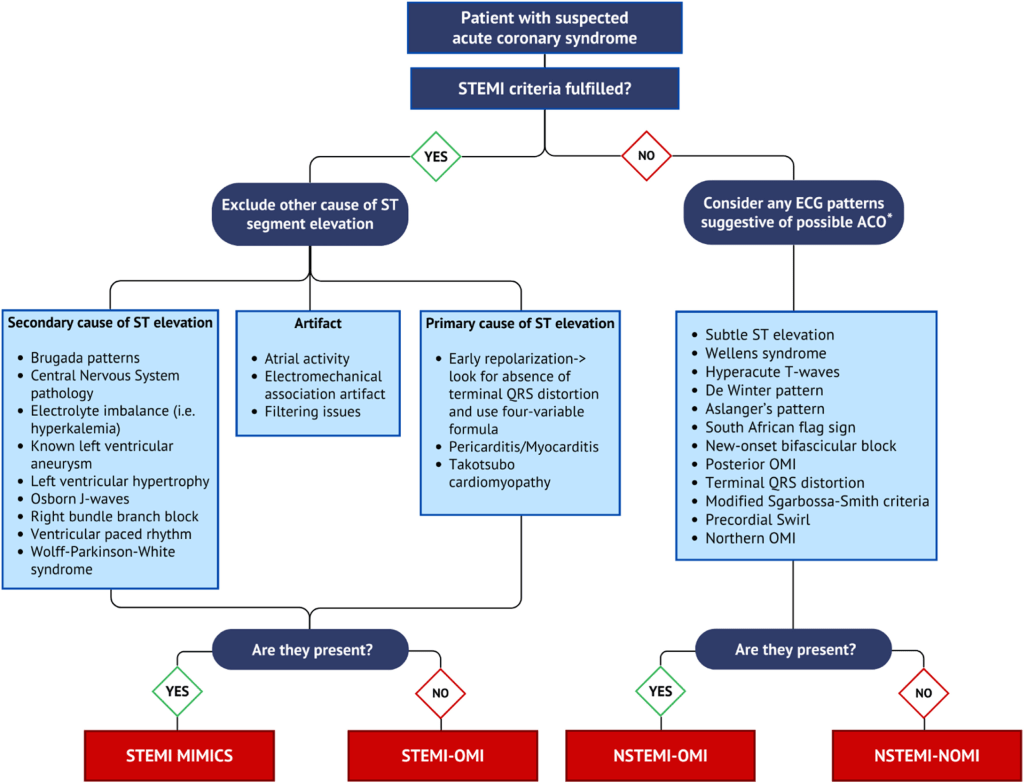
- Occlusion Myocardial Infarction (OMI) is the proposed new term for MIs that benefit from the Cath lab. Would replace STEMI/STEMI equivalent.
- Occlusion myocardial infarction represents an ongoing ischemia resulting in irreversible infarction caused by complete or near-complete occlusion of a culprit epicardial coronary artery, with inadequate collateral circulation, thus necessitating immediate reperfusion.
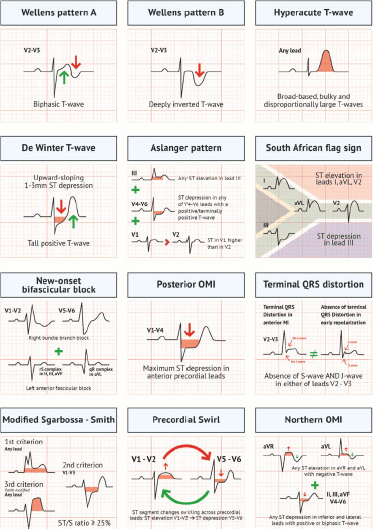
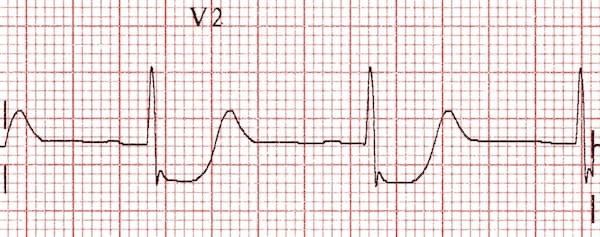
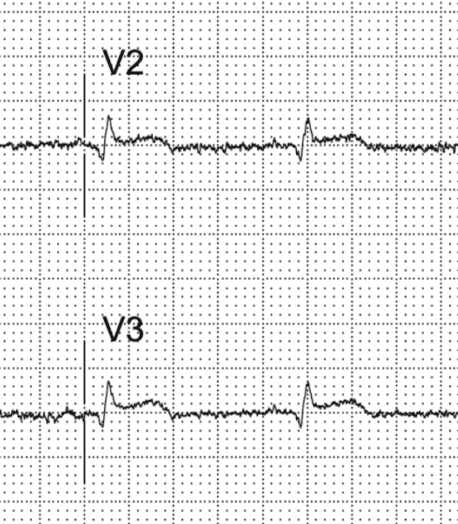
- Wellens Syndrome (V2-V3)
- Biphasic (pattern A) or deeply inverted (pattern B) T wave in leads V2-V3 and the absence of Q waves (Figure 1, Table 2) in a patient with recently resolved chest pain
- Critical and proximal stenosis of the left anterior descending coronary artery.
- Wellens’ pattern represents acute reperfusion of occlusion myocardial infarction that went unrecorded by the ECG during the episode of pain.
- Cardiac biomarker levels almost always have some amount of elevation above the upper reference limit. During the active symptoms, the culprit vessel is functionally occluded (but neither ECG nor angiogram was recorded or recognized during that time), but then there is spontaneous or medication-induced partial thrombolysis with the restoration of some myocardial blood flow, causing resolution of active occlusion myocardial infarction findings and symptoms.
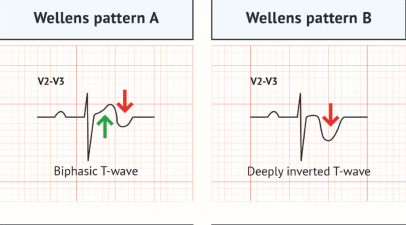
- Hyperacute T Waves
- Distinctive T-wave change seen in the early to middle stages of occlusion myocardial infarction, in which the T waves in the affected leads are both more symmetric and enlarged in terms of overall area under the curve relative to both their baseline size and to their QRS complex size.
- Hyperacute T waves are often the earliest specific ECG feature of occlusion myocardial infarction that can be recognized by trained and qualified ECG readers, exceeding the diagnostic accuracy of STEMI criteria in blinded studies.
- Mattu says suspect if T > QRS or if >10mm in men and >8 mm in women
- De Winter Pattern
- Tall, prominent, symmetrical T waves in the precordial leads
- Upsloping ST segment depression > 1mm at the J point in the precordial leads
- Absence of ST elevation in the precordial leads
- Reciprocal ST segment elevation (0.5mm – 1mm) in aVR

- Aslanger Pattern
- 1) Inferior STE isolated to lead III
- 2) Concomitant ST depression in any of V4-V6, with a positive/terminally positive T-wave
- 3) ST segment in V1 > V2
- South African Flag Sign (High Lateral STEMI)
- ST elevation primarily localised to leads I, aVL +/- V2
- Reciprocal ST depression and/or T wave inversion in inferior leads, most pronounced in lead III
- New-Onset Bifascicular Block
- obstruction of the proximal left anterior descending coronary artery may result in a right bundle branch block and/or left anterior fascicular block
- Posterior Occlusion Myocardial Infarction
- isolated ST-depression 0.5 mm and greater in V1-V3 leads may indicate left circumflex artery occlusion, best detected using posterior leads (ST-segment elevation ≥0.5 mm in V7-V9),
- Horizontal ST depression V1-3
- Tall, broad R waves (> 30ms)
- Upright T waves
- Dominant R wave (R/S ratio > 1) in V2
- Differentiating the ST-Segment Elevation of Normal Variant in V2-V4 From Subtle Occlusion Myocardial Infarction
- Use Subtle STEMI on MDCalc
- Must be at least 1mm STE in at least 1 lead from V2-4.
- Cannot show:
- >5mm STE
- Non-concave STE
- Inferior reciprocal changes
- Anterior ST depression
- Terminal QRS distortion in V2 or V3 (absence of S or J point notching)
- Use Subtle STEMI on MDCalc
- Terminal QRS Distortion
- Four-variable subtle anterior STEMI formula referenced above in MDCalc is a tool to differentiate normal variant elevation from LAD occlusion.
- Terminal QRS distortion is another, more rapidly identifiable feature that can differentiate between the two. It is defined by the absence of an S wave and J wave in either of leads V2 or V3.when there is any precordial ST-segment elevation, if terminal QRS distortion is present, it is highly specific for left anterior descending coronary artery occlusion myocardial infarction
- Benign early repolarisation (BER) – no terminal QRS distortion

- LAD occlusion – terminal QRS distortion
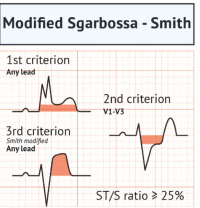
- Smith-Modified Sgarbossa Criteria for LBBB or ventricular paced rhythm
- Concordant ST-segment elevation 1 mm in any 1 lead or more
- Concordant ST-depression 1 mm in 1 lead of V1-V3
- Proportionally excessive discordant ST-segment elevation in any 1 lead and greater anywhere with 1 mm and greater ST-segment elevation, as defined by 25% and greater of the depth of the preceding S wave
- A cutoff of ST-Segment elevation to S-wave ratio of 20%, rather than 25%, was more sensitive and almost as specific
- Precordial Swirl
- The “precordial swirl” occlusion myocardial infarction pattern features marked ST-segment elevation and/or hyperacute T waves in V1-V2 and ST-depression and/or T-wave inversion in V5-V6, creating a distinctive clockwise vortex appearance of the ST-T waves through precordial leads.
- left anterior descending coronary artery occlusion myocardial infarction, typically proximal to the first septal perforator
- Northern Occlusion Myocardial Infarction
- any ST-segment elevation in aVR and aVL with negative T wave
- any ST-depression in inferior and lateral precordial leads with positive or biphasic T wave
Managing Acute Respiratory Failure With Facemask Noninvasive Ventilation
EMCRIT
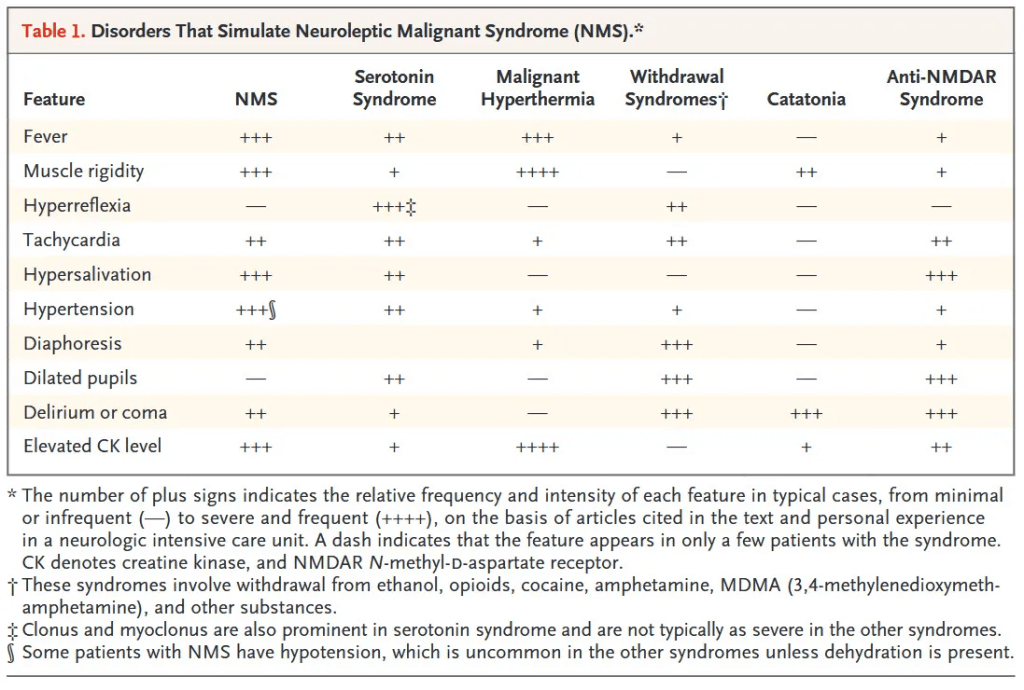
EMCrit 399 – Serotonin Syndrome (SS) and Neuroleptic Malignant Syndrome (NMS) – Primer Episode
EMCrit 398 – NeuroEMCrit – NeuroMuscular Emergencies
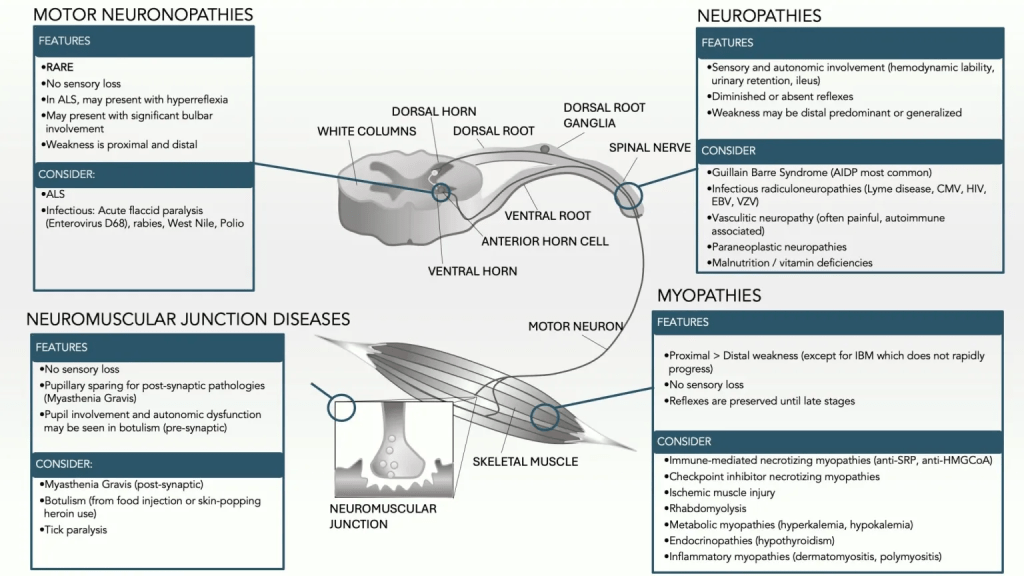
- Neuromuscular emergencies encompass four buckets of diseases (last 3 are important for ED):
- 1. Motor Neuropathies (ALS, Polio, West Nile) involve the lower/peripheral motor neuron (anterior horn cell) at it’s origin in the spinal cord right after it has received the neurotransmitter from the central upper motor neuron and before it has exited the spinal cord (see image below with circle at the origin of the anterior horn cell):
- Rare diseases with no ED treatment
- Features: no sensory loss because it has not exited the cord and joined the sensory nerves in the spinal nerve bundle, only motor function impaired
- Differential: ALS, Infectious: acute flaccid paralysis, rabies, West Nile, Polio
- 2. Neuropathies (Guillain Barre most common) involve the spinal nerve bundle which includes both the motor and sensory peripheral nerve as well as autonomic function,
- Sensory, Autonomic (hemodynamic lability, urinary retention, ileum) and Motor involvement and even cranial nerves (MFS variant of GBS)
- Diminished or absent reflexes
- Weakness may be distal initially, ascending weakness for GBS
- Guillain Barre (AIDP most common, Miller Fisher less common), Infectious radiculoneuropathies (CMV, HIV, Lyme disease)
- 3. Neuromuscular Junction Diseases (Myasthenia Gravis, Botulism, Tick Paralysis)
- No sensory loss
- Post-synaptic (Myasthenia- immune system mistakenly produces antibodies to the acetylcholine receptors on the muscular post-synaptic membrane)
- Pre-synaptic (Botulism, Ticks, Lambert-Eaton)
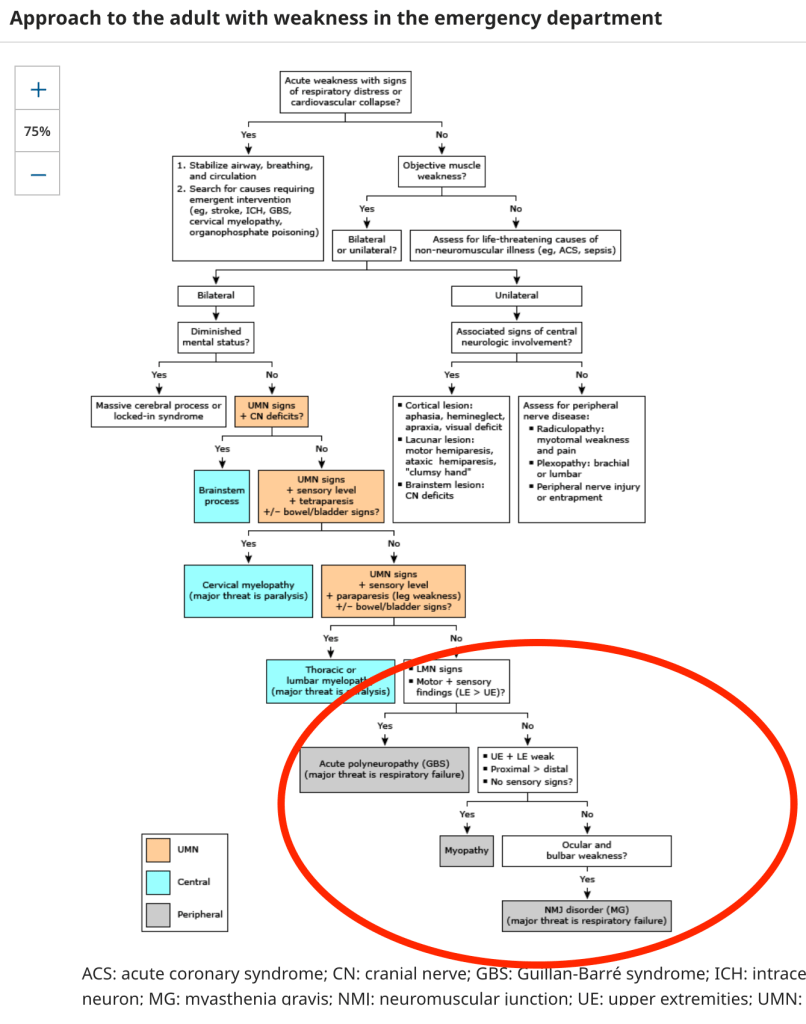
- 1. Motor Neuropathies (ALS, Polio, West Nile) involve the lower/peripheral motor neuron (anterior horn cell) at it’s origin in the spinal cord right after it has received the neurotransmitter from the central upper motor neuron and before it has exited the spinal cord (see image below with circle at the origin of the anterior horn cell):
- to the represent the last branch point in the UPTODATE weakness algorithm (see below) involving bilateral lower motor neuron findings
History

Physical Exam

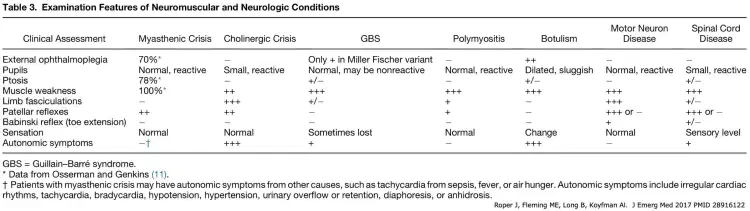
Myasthenia Gravis
Facial weakness, ptosis, extremity weakness. Pupils are spared. Symmetrical, fatigable.
New Presentation
Old man or young woman classically
Need to see a neurologist for full testing and screening
Fatigability Tests
Look up for 30 seconds, ptosis may emerge or get worse
Flap the chicken wing on one side 30 times and then test strength in both arms
EMRAP
Pediatric Smackdown: Minor Procedures and Sedation/Analgesia
Ilene Claudius, MD; Al Sacchetti, MD; and Jeff Seiden, MD
There is significant anxiety associated with a visit to the ED, especially when it comes to procedures such as lumbar punctures, catheterization, and IV placement.
Pharmacologic:
- Sucrose solution (Sweetease): used for pain control and anxiolysis in infants from birth to 6 months (best for infants 0-6 weeks).
- Administer to the buccal mucosa or place on a pacifier.
- Intranasal fentanyl: 1-2 μg/kg (best used for children >2 months)
- Monitor with a pulse oximeter; duration of action is <20 minutes.
- At low doses, it will provide analgesia and possibly mild sedation.
- Ketamine (children >3 months)
- Administer 1 mg/kg intranasal for mild sedation.
- Administration of 1.5 mg/kg IV results in deep sedation (and requires closer monitoring).
- Midazolam (can be given intranasally): pure periprocedural anxiolysis, typically for children >6 months.
- Pharmacologic agents for sedation or analgesia introduce potential risks, including medication side effects, dosing errors, additional cost, and additional resource utilization.
Nonpharmacologic:
- Distraction techniques, toys, and child life specialists are proven techniques to help facilitate procedures in the ED without side effects.
- Parents/caregivers should be in the room to help keep the child comfortable and calm during procedures.
- They can help with distraction, comfort, and positioning.
PEARL: There are many pharmacologic and nonpharmacologic methods to help facilitate procedures in the pediatric ED. The correct combination of these tools may be case specific to help facilitate invasive procedures.
Opioid Update
Jessie Werner, MD, and Darren McCollum, MD
Fentanyl
- Fentanyl is everywhere and is in everything!
- There is a huge supply and it is very cheap.
- It is terrifying for many reasons:
- Potent
- Cheap to make
- Made in a few different ways and precursors are inexpensive
- Widely available
- Difficult to track and regulate by drug enforcement
- Fentanyl precursors made from readily available chemicals
- Easier to track where heroin was coming from (opium farms in Afghanistan and Australia)
- Unable to regulate amount of fentanyl in the products being sold
- Leads to more overdoses (300 μg vs 5 μg in fake norco pills)
- People don’t know how much they are actually taking
Narcan/naloxone
- We are starting to see a trend in administering higher doses of naloxone (Narcan) to treat overdoses:
- 10 mg or 20 mg doses of naloxone
- Monitor patients for at least 4 hours post-naloxone administration.
- The pharmacokinetics of street vs. hospital fentanyl is completely different
- Naloxone-induced noncardiogenic pulmonary edema (NCPE) is a rare but serious side effect following naloxone administration.
- Related to catecholamine release after naloxone is administered
- Related to dose of naloxone given
- More likely in patients who were breathing and suddenly regained ventilation (alveoli “pop” open quickly leading to pulmonary edema)
- 2020 Annals of Emergency Medicine Review
- This review examined whether the administration of higher doses of naloxone was associated with increased pulmonary complications.
- Patients who received >4.4 mg of naloxone were 62% more likely to have pulmonary complications.
- Despite this relationship, the study did not find a clinically significant relationship between elevated naloxone doses and pulmonary edema specifically.
- This review examined whether the administration of higher doses of naloxone was associated with increased pulmonary complications.
Components mixed with fentanyl
- Xylazine (Tranq) or medetomidine
- Breaking News Special with Dr. Swadron and Dr. Nordt
- EMA Abstract
- Alpha-2 agonists
- Presents like heavier opioid intoxication
- Miosis, bradypnea, hypotension, bradycardia
- Sometimes contaminates the fentanyl supply
- These agents make the hit “harder” but also more difficult to reverse because xylazine is not going to respond as you traditionally see with naloxone dose
- Many patients are admitted to the ICU on vasopressors until they metabolize
- Many synthetic opioids are not going to show up on a urine toxicology screen.
Buprenorphine
- Use buprenorphine in patients as treatment for active withdrawal.
- An X-waiver is no longer needed.
- Dr. Reuben Strayer Segment
- For the most part, buprenorphine is very safe.
- If your ED does not have buprenorphine, you can consider using clonidine in a patient with active withdrawal.
- Mortality for young patients who present after an opioid overdose is high; consider using buprenorphine!
PEARL: Unregulated fentanyl doses and synthetic opioids are commonly found in street fentanyl today. These drugs produce an intoxication or overdose that is difficult to treat with common naloxone doses or with naloxone alone. Consider higher doses of naloxone and/or supportive care for mixed ingestion cases.
Critical Care Mailbag: RSI
Anand Swaminathan, MD, and Scott Weingart, MD
Drs. Swaminathan and Weingart take a deep dive into critical topics such as rapid sequence intubation, laryngoscope blade size, and reoxygenation in between failed intubation attempts.
Rapid Sequence Intubation
- Definition: RSI is the near simultaneous administration of induction agent and paralytic that rapidly achieves ideal intubating conditions.
- Today, RSI entails resuscitation of the patient prior to intubation, positioning of the patient, and other key factors.
- Timing principle of medication administration:
- Etomidate achieves apnea at the 45-second mark, succinylcholine achieves apnea at the 45-second mark, and rocuronium achieves apnea at the 60-second mark.
- So, there’s an extra 15 seconds of unwanted apnea if you use the etomidate/rocuronium combination and push medications back to back.
- In the anesthesia literature, a few randomized controlled trials state that you should push rocuronium first, wait 15 seconds, and then push the induction agent (reverse order).
- This approach is based on theoretical ideas of timing but may not necessarily be a “win,” even though it makes sense on paper.
- Etomidate achieves apnea at the 45-second mark, succinylcholine achieves apnea at the 45-second mark, and rocuronium achieves apnea at the 60-second mark.
- Consider using ketamine for intubation; there is no additional period of apnea because it does not induce apnea.
- Ketamine does not have to be “slammed in” because it doesn’t stop the patient’s breathing.
- Administer a slow push of ketamine (3-4 seconds).
- This is ideal for patients who are hypotensive.
- Ketamine may not be available at all institutions.
- Consider pushing medications yourself to make sure the timing is right.
- Consider using a stopwatch or clock with seconds for ideal timing and medication onset.
- Catoire et al. performed a secondary analysis of the association between pushing the paralytic first and first-pass intubation success.
- Failure in emergency medicine airway management:
- Pushing the paralytic and then not waiting the right amount of time:
- Etomidate = wait 45 seconds after medication push
- Rocuronium = wait 60 seconds after medication push
- Pushing the paralytic and then not waiting the right amount of time:
Size of Laryngoscope Blade (Macintosh)
- Length of blade does not really matter for Miller or Hyperangulated blades because you are not using a lifting force.
- For Macintosh-style blades, blade size is very important because it works first by compression of structures like the tongue and the bottom of your mouth and then by jaw suspension.
- Requires task-specific muscle development for lifting force
- Physics of Macintosh Laryngoscope
- The Macintosh blade is the lever arm.
- The further away the weight at the end of the lever arm is from the axis of force (the handle of the laryngoscope), the more weight you’re actually lifting, and the more force you have to apply to get that same amount of lift.
- Mac 3 (if it reaches) will allow you to have much easier lifting force to get the exposure you need for that individual patient.
- Mac 4 adds the amount of force you need for that same amount of lift.
- Mac 3 works for almost all adults, but consider sizing up to Mac 4 if the patient’s jaw looks big (and lay the Mac 3 against them to size appropriately).
Reoxygenation In Between Failed Intubation Attempts
- Use a bag valve mask (BVM) or supraglottic airway.
- Consider attaching end-tidal waveform onto BVM to know whether or not the patient is difficult to bag.
- Consider putting in an oral or nasal airway.
- Reposition the patient.
- Use a good C-E grip, with two hands and “thumbs to feet” grip, on BVM (with separate person bagging) to give breath, and if no end-tidal, then use your supraglottic airway.
- Supraglottic airway is helpful in patients with a lot of facial hair or when you have a limited ED team and all hands need to be on deck (good seal, BVM bagging, etc).
PEARL:
- Consider onset of action of RSI medication and timing between administration. Weingart likes Ketamine because no apnea (as long as you push slowly over 4 seconds) unlike Etomidate. If you use etomidate then give Roc first because onset is 60 seconds, Etomidate 45 seconds so avoids prolonged apnea. Use a stopwatch to ensure you attempt intubation at 60 seconds after Roc is pushed. Reuben Strayer likes Ketamine over Etomidate for all intubations except patients who you don’t want HR and BP rise (SAH, Aortic Dissection, Sympathomimetic toxicity).
- Mac 3 blade best for adults except patient with very large jaw (then do Mac 4). Mac 3 also works for kids except preemie according to Weingart!!
- For reoxygenation between failed intubation attempts, you don’t always have to use a supraglottic airway device as long as you can get a good seal on with your BVM (two hands on the mask and another person providing the bagging).
Cervical Spine Clearance
Anand Swaminathan, MD, and Andrew Petrosoniak, MD
Summary:
- Nexus and Canadian C-spine rules are sensitive but they are not perfect. It is important to consider the pretest probability of injury when considering the need for imaging.
- Know the inclusion/exclusion criteria for decision rules (eg, patients with altered mental status were not included in original studies). You must apply them correctly when deciding not to obtain imaging.
- The mean age of patients included in the Canadian C-spine rule study was 37 years. Patients >65 years should be imaged if there is concern for injury, regardless of rules.
- Geriatric patients require special consideration given the conflicting data in the literature. The absence of neck pain does not exclude a c-spine injury in this special population.
- When in doubt, obtain a CT c-spine on elderly patients following ground-level falls or on patients in high-risk populations. If obtaining a head CT, strongly consider adding a CT c-spine.
- Special populations at high risk of c-spine injury include geriatric patients, frail patients, those with a history of rheumatoid arthritis or Down syndrome (atlantoaxial instability), prior c-spine injury or surgery, or bamboo spine (diffuse idiopathic skeletal hyperostosis [DISH]) or osteophytes on CT.
- Plain X-rays are non-diagnostic for c-spine injuries in adults. If you are seeking c-spine clearance, obtain a CT.
- A normal neurological exam (paresthesia and weakness), absence of midline tenderness, and normal range of motion are required to clear the c-spine. If unable to clear on the initial exam and the CT is negative, the patient must be re-examined and cleared after a repeat normal exam.
- If there is persistent midline tenderness after a negative CT c-spine, obtain magnetic resonance imaging or consult spine specialists at your institution. If spine specialists are unavailable, then discharge patients with a soft collar and have them follow up in 1 week in the ED or outpatient for re-examination.
PEARLS: Clinical decision rules are not perfect. Consider imaging high-risk populations and frail patients following ground-level falls. C-spine injuries can be missed even with a negative CT. Always re-examine your patients after a negative CT c-spine and clear the c-spine ONLY after a normal re-examination.
Case of the Week: Management of Cirrhotic Ascites and Paracentesis
Anand Swaminathan, MD, and Jan Shoenberger, MD
Jan and Swami discuss the case of the week involving a patient with cirrhosis. This segment touches on important points to consider when evaluating and managing cirrhotic patients and common paracentesis complications.
Case: A patient with known cirrhosis presents with abdominal distention, shortness of breath, and abdominal discomfort. Vitals are stable (heart rate is normal, respiratory rate is slightly elevated due to abdominal distention, and oxygen saturation [SpO2] is 98%). The exam is notable for ascites without abdominal tenderness. He is requesting a paracentesis.
Initial Evaluation:
- Distinguish whether this is the usual presentation for cirrhosis. Keep a broad differential and rule out pneumonia, pulmonary embolism (PE), and other etiologies of dyspnea.
- When was the last paracentesis? Is there a change in urine output? These patients are at risk of hepatorenal syndrome.
- Evaluate for diuretic resistant/refractory ascites by asking about medication compliance.
Workup Considerations:
- Therapeutic paracentesis is indicated to relieve discomfort and dyspnea. Embrace the opportunity to prioritize patient comfort and establish rapport.
- Always use an ultrasound as it improves accuracy and decreases complication risk. Use local anesthesia and know your landmarks.
- Labs are not absolutely necessary before a paracentesis, especially if there are recent labs (within 1-2 weeks) to refer to. Consider labs in patients with symptoms of weakness or atypical presentation as these patients are at risk of hyponatremia, renal dysfunction, gastrointestinal (GI) bleeding, and occult infections.
- Always send ascitic fluid for cell count. Do not rely on absence of abdominal tenderness to rule out spontaneous bacterial peritonitis (SBP). SBP can be tricky.
Large-Volume Paracentesis
- Albumin is recommended if removing >5 L of ascitic fluid or if BP drops.
- Observation for hypotension can be completed while the patient awaits cell count and lab results.
Paracentesis Complications:
- If a patient becomes hypotensive, use albumin instead of normal saline or lactated Ringers. Normal saline and colloids are not as effective due to decreased oncotic forces and increased fluid shifting.
- If there is a bloody tap that clears, then this is likely secondary to procedural trauma. It is safe to continue with the procedure. If the blood does not clear during the paracentesis, stop the procedure, obtain serial hemoglobins, and consider a computed tomography (CT) angiogram of the abdomen to evaluate for etiology of blood (eg, bleeding hepatocellular carcinoma or vascular injury).
- Persistent leakage of ascites at the site of paracentesis can be fixed with a suture or Dermabond.
Disposition:
- Discharge the patient after a negative SBP workup and completion of observation time without complications.
- Ensure outpatient gastroenterology follow-up.
- Consider palliative care consult as these patients are high risk with a high mortality rate.
PEARL: A paracentesis is an opportunity to prioritize patient comfort. Paracentesis can be completed without pre-procedure labs. Always remember to send a cell count because SBP can be easy to miss.
Cardiology Corner: Asymptomatic HTN
Anand Swaminathan, MD, and Amal Mattu, MD
Summary:
- Hypertensive emergency: severely elevated BP and evidence of new end-organ damage
- Severely elevated BP = systolic BP >180 mm Hg, diastolic BP >110 mm Hg
- End-organ damage:
- Brain: ischemic stroke, intracranial bleeding, encephalopathy
- Cardiac: acute coronary syndrome (ACS), cardiogenic pulmonary edema
- Renal: acute renal failure, acute elevation in creatinine
- Vascular: aortic dissection, retinopathy, microangiopathic hemolytic anemia
Evaluation:
- Acute neurologic problems can be largely ruled out in patients without a headache/vision changes or neurologic symptoms.
- Patients without chest pain/discomfort, orthopnea, or shortness of breath may not need an ECG or further workup.
- Consider a creatinine or urine dip as kidney function cannot be easily assessed on history and physical.
- Without a baseline, it may be difficult to interpret whether it represents an acute change in renal function, but the value may indicate the urgency of the workup or follow-up that the patient needs.
Management :
- There is no proven benefit to treating elevated BP without evidence of end-organ damage.
- There are risks associated with using IV medications to acutely decrease BP, and such medications should be avoided if not necessary.
- If the patient is on medications but missed their dose, they can resume their home medications or increase their dose.
- Asymptomatic patients with elevated BP do not routinely need to be admitted.
- There is no strict cutoff for management of markedly elevated BPs (eg, systolic BP >220 mm Hg). It is patient- or system-specific whether they need admission for monitored slow correction of their BP vs close outpatient management.
- If you decide to start a new antihypertensive, you can look up the 2017 hypertension clinical practice guidelines for the most appropriate initial medication.
Pearl: A thorough history and physical is the most important step for assessment of asymptomatic hypertension; for many of these cases, all they need is close outpatient follow-up.
REFERENCES:
The management of elevated blood pressure in the acute care setting: a scientific statement from the American Heart Association
Bress AP, Anderson TS, Flack JM, et al. Hypertension. 2024;81(8):e94-e106. doi: 10.1161/HYP.0000000000000238. PMID: 38804130
2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines
Whelton PK, Carey RM, Aronow WS, et al. Hypertension. 2018;71(6):1269-1324. doi:10.1161/HYP.0000000000000066. PMID: 29133354 [published corrections appear in Hypertension. 2018;71(6):e136-e139 (doi: 10.1161/HYP.0000000000000075) and Hypertension. 2018;72(3):e33. (doi: 10.1161/HYP.0000000000000080)]
First10 EM
None
NEJM
Alteplase for Posterior Circulation Ischemic Stroke at 4.5 to 24 Hours
REBELEM
None
