Academic Emergency Medicine
None
Annals of Emergency Medicine
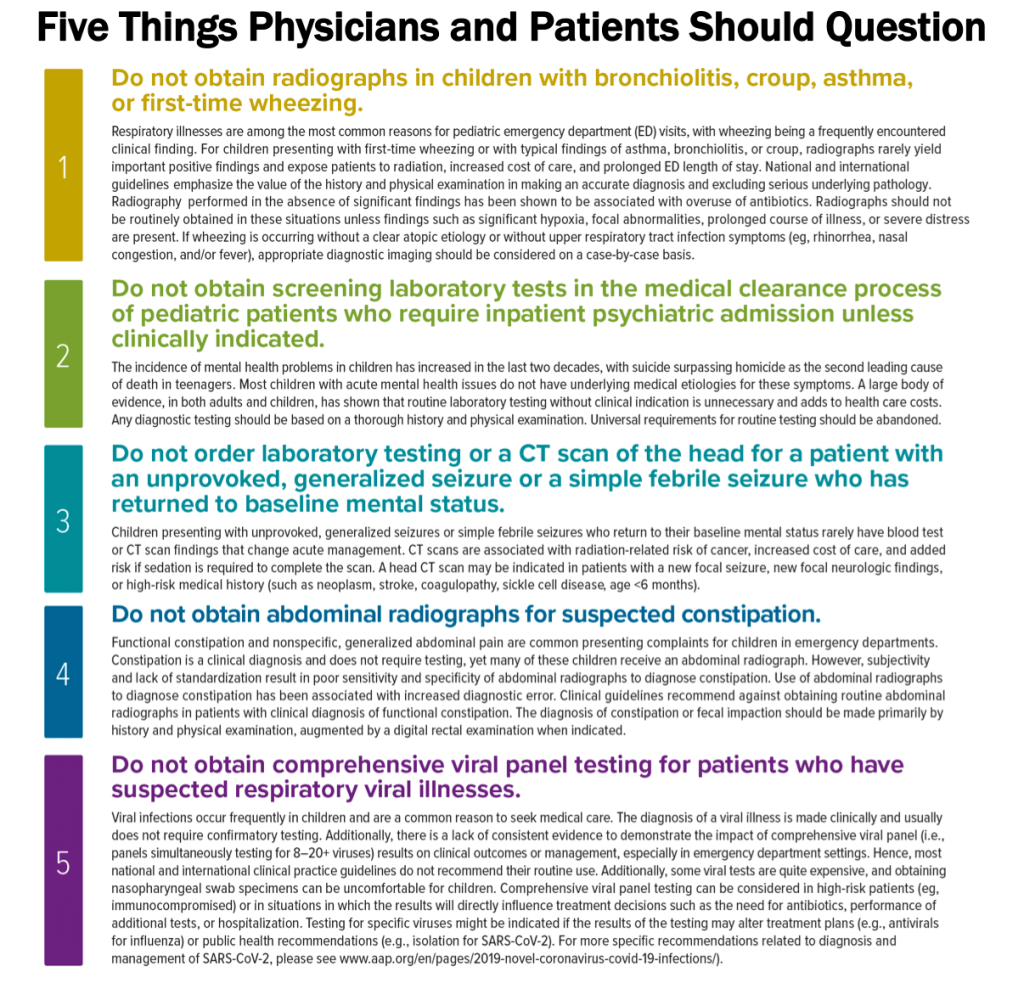
Adherence to “Choosing Wisely” Recommendations in Pediatric Emergency Medicine
EMCRIT
EMCrit 403 – What’s the Status of Status – Status Epilepticus 2025 with PulmCrit
Benzodiazepenes
Josh is giving 0.1 mg/kg of Lorazepam (up to 8 mg)
Scott varies by scenario:
Seizing < 5 minutes
Nothing or 2 mg of lorazepam
Status Epilepticus (seizing >5 minutes, but <10 min)
If you have IV access:
Midazolam 5 mg IV
wait 2-3 minutes
Repeat Midazolam 5 mg IV
No IV:
RAMPART dose of 10 mg IM up front
Status Epilepticus (Seizing with EMS prior to arrival, >10 minutes seizing)
Midazolam 10 mg IV or IM (if patient did not get this dose in the field already)
Ketamine
Scott gives Ketamine 1mg/kg with his second dose of midazolam, or immediately following the first 10 mg dose in extended seizures
Ket-Mid Study
PMID [40186980]
Debate with First10EM on this Study
Scheppke Study
PMID: 39642307
- F/u Retrospective Study with comparison group [DOI: 10.1016/j.annemergmed.2024.11.002]
- Additional support with ketamine as first-line infusion in peds [10.1007/s12028-025-02212-5]
Anti-Epileptics
We both start with Levetiracetam (Keppra) 60 mg/kg (max dose 4.5 g)
Give this whenever it is ready, but do not wait for it to work, if the patient is still seizing, move on to intubation and propofol
ESETT Trial looked at this dosing [10.1056/NEJMoa1905795]
2nd line anti-epileptic:
Lacosamide (Vimpat)
Major contraindications:
- Pre-existing heart block or conduction system disease.
- Underlying proarrhythmic conditions (ventricular tachycardia is reported in some cases).
- Severe hepatic dysfunction
Dose:
400 mg IV over 5 minutes (See IBCC for additional dosing info)
Med QuickRef
able 7. Medications for Status Epilepticus
First-Line Agents
| AGENT | ROUTE | DOSAGE |
|---|---|---|
| Lorazepam | IV | • 0.1 mg/kg; max 4 mg/dose (some say 8 mg) • May repeat once |
| Midazolam | IM/IV | • Weight 13–40 kg: 5 mg • Weight >40 kg: 0.2 mg/kg, max 10 mg • May repeat once |
| Diazepam | PR | 0.2–0.5 mg/kg, up to 20 mg, 1 time |
Second-Line Agents
| AGENT | ROUTE | DOSAGE |
|---|---|---|
| Levetiracetam | IV | 60 mg/kg; max 4.5 g |
| Valproate sodium | IV | 40 mg/kg; max 3 g |
| Fosphenytoin | IV | 20 mg PE/kg; max 1.5 g |
| Phenobarbital | IV | 15–20 mg/kg; max 2 g |
| Lacosamide | IV | 200–400 mg |
Third-Line Agents
| AGENT | ROUTE | DOSAGE |
|---|---|---|
| Midazolam | Infusion | Load with 0.2 mg/kg and infuse at 0.05–2 mg/kg/hr, with repeat bolus of 0.1–0.2 mg/kg if breakthrough seizure |
| Propofol | Infusion | Load with 1–2 mg/kg and infuse at 30–200 mcg/kg/min |
| Pentobarbital | Infusion | Load with 5–15 mg/kg and infuse at 0.5–5 mg/kg/hr |
| Thiopental | Infusion | Load with 2–7 mg/kg and infuse at 0.5–5 mg/kg/hr |
| Ketamine | Infusion | Load with 0.5–3 mg/kg and infuse at 0.1–5 mg/kg/hr |
Meds for Intubation
Scott uses propofol and succinylcholine
Josh uses Ketofol and rocuronium (but lower dose, 0.5-0.6 mg/kg
have a low threshold to intubate these patients!!
General Anesthetic after Intubation
We both use propofol. Scott would consider switching to high dose midazolam drip after 48 hrs if the pt is still seizing.
You need higher doses of propofol to stop seizures, 80-100 mcg/kg/min
These pts will all need norepi, bring it to the bedside immediately after intubation
EMRAP
Validating the Sudbury Vertigo Risk Score
- EDITOR’S COMMENTARY: This study provides the first validation of the recently derived Sudbury Vertigo Score. The score performed very well: scores <5 were associated with 0% risk of serious outcomes, and most patients were in this category. This validation was conducted in a historical cohort of patients at the same 3 sites from which the rule was derived, through retrospective methods leaving much to be desired. I do not think that this rule can be applied to the bedside yet, but it holds promise for helping differentiate this difficult-to-assess patient population.
EMA 2025 June Abstract 6: Risk of Delayed Intubation After Presumed Opioid Overdose in the ED
- EMA EDITOR’S COMMENTARY: This large prospective study included consecutive patients treated with naloxone for presumed opioid overdose at 10 major toxicology centers in the U.S. Only 1/1,591 patients (0.1%) required an intubation more than 4 hours after arrival, ostensibly because of ongoing toxic drug effects. Although the study has substantial limitations, the findings generally confirm that a 4-hour watch window is sufficient to identify almost all patients who will experience respiratory arrest.
- EM:RAP HD: Shoulder Reduction by Wrist-Clamping and Shoulder-Lifting
Sickle Cell Disease: Critical Illness
Anand Swaminathan, MD, and Jeff Glassberg MD
Pain control
- Patients with sickle cell disease frequently present with flare-ups of chronic pain and vaso-occlusive crises.
- We do not have a good test to determine whether patients are experiencing pain. Our duty is to treat their discomfort.
- We can look for trends of utilization that may suggest chronic pain.
- The first step is to treat their pain at this visit.
- Then we can look for ways to better connect these patients and more appropriately treat the chronic component of this condition.
- We can look for trends of utilization that may suggest chronic pain.
Transfusion goals:
- The treatment for sick or ill-appearing sickle cell patients with concern for any type of vaso-occlusive crisis or acute chest is to transfuse.
- The key to treatment is reducing the fraction of a patient’s own sickled blood to transfused blood.
- Do not transfuse to a hemoglobin (Hgb) >11 as this increases the risk of stroke.
- Patients with mild genotypes that have a higher baseline Hgb may need emergent exchange transfusion.
Vaso-occlusive crisis:
- Create a broad differential diagnosis.
- Labs: complete blood count ( CBC), reticulocyte count, comprehensive metabolic panel (CMP), lactate dehydrogenase (LDH), Hgb fractionation/plasmapheresis (will help the inpatient team). Assess these labs based on the patient’s baseline if available.
- Treatment:
- Oxygen is not beneficial if O2 saturation is >95%.
- Give a small amount of fluids; eg, 1 L of half-normal saline (1/2NS) or 5% dextrose in half-normal saline (D51/2NS) over several hours.
Acute chest syndrome:
- Clinically appears like pneumonia (chest pain, cough, hypoxia, infiltrate on CXR)
- Treat as you would pneumonia (antibiotics, pain control)
- If they are sick, the key treatment is blood transfusion even if the CXR is normal
Splenic Sequestration:
- While traditionally a pediatric condition, the early use of hydroxyurea can delay or prevent splenic auto-infarction in children, preserving immunocompetence.
- Patients who have not auto-infarcted their spleens are at risk for splenic sequestration as an adult.
- They present with abdominal pain or weakness and can go into hemorrhagic shock.
- These patients may show massive splenomegaly (>20 cm) on ultrasound.
- Treatment:
- Frequent CBC every 4 to 6 hours, frequent transfusion Hgb 1-2 > baseline, and neuro checks every 2 hours.
- When splenic sequestration reverses, it can lead to significant rise in Hgb, leading to massive strokes; treatment is emergent phlebotomy.
Delayed hemolytic transfusion reaction (DHTR):
- Patients generate antibodies to both transfused and native blood, leading to an amplified hemolysis of all of their blood.
- If a patient has received a recent transfusion and presents with an Hgb that is lower than their starting point, this raises concern for DHTR (or bleeding).
- Treatment includes transfusion and immunosuppression.
PEARL: The key components to treating sickle cell crisis is to treat the patient’s pain, keep them comfortable, and, if they appear ill from any type of vaso-occlusive crisis, to transfuse to decrease the ratio of sickled to transfused blood.
EMA 2025 June Abstract 13: Nebulized Tranexamic Acid for Post-Tonsillectomy Bleeding
- EMA EDITOR’S COMMENTARY: If you want to know everything there is to know about the evidence behind nebulized TXA for post-tonsillectomy hemorrhage, this is the article for you. The authors go over all 9 studies on the topic and provide easy-to-follow summaries of each. In sum, although nebulized TXA appears promising as a first-line intervention for PTH, higher-quality prospective studies with standardized protocols are needed before this modality can be universally recommended as standard practice in emergency departments.
EMA 2025 June Abstract 14: Biphasic Anaphylaxis: Incidence and Risk Factors
- EMA EDITOR’S COMMENTARY: In this single-center study, the authors estimate that biphasic anaphylaxis has an incidence of 16%, occurs an average of 21 hours after the initial reaction, and is generally mild. Emergency providers can use this information to provide anticipatory guidance and return precautions for patients being discharged after successful treatment for anaphylaxis.
Trauma and Transfusion: MTP and More
Jan Shoeneberger, MD, and Kenji Inaba, MD
On the 10-year anniversary of the landmark PROPPR trial, Dr. Kenji Inaba joins Dr. Jan Shoenberger to reflect on its lasting impact on massive transfusion protocols (MTPs). They explore practical challenges in trauma resuscitation, including limited access to O-negative blood, the growing interest in whole blood, and the ethical and logistical considerations clinicians face in real-time decision-making.
1. When to Activate the MTP
- Clinical triggers:
- Shock index >1 (HR/SBP)
- ABC score ≥2 (penetrating trauma, hypotension, positive FAST, tachycardia)
- Clinical gestalt: patient looks like they’re actively bleeding and unstable
- Immediate action:
- Send pink-top tube ASAP for type and cross
2. Standard Transfusion Ratio
- 1:1:1 ratio = 1 unit packed red blood cells (PRBC): 1 unit fresh frozen plasma (FFP): 1 apheresis platelet unit
(universal standard as of 2025)
3. Whole Blood
- Use when available, ideally low-titer O-positive
- Evidence of benefit exists, but data still limited
- TROOP trial is ongoing to evaluate whole blood + components vs components alone
4. O-Positive vs O-Negative Emergency Blood Use
- O-negative preferred for
- Women <55 years old
- Children <13 years old
- O-positive acceptable in life-threatening hemorrhage when O-negative is unavailable
- Alloimmunization risk is low (<7%)
- Administer RhoGAM if appropriate
5. Key Practical Reminders
- Activate MTP early in suspected hemorrhage
- Always aim for group-specific blood quickly (send pink top)
- Whole blood can be a first-line option if stocked
- If only O-positive blood is available, use it in crashing patients (prioritize survival)
PEARL: On this 10-year anniversary of the PROPPR trial, remember to activate MTP early. Always send a pink-top tube to expedite group-specific blood. Use whole blood as the first line if available. In a crashing patient, use O-positive if necessary—survival takes priority.
EMA 2025 June Abstract 15: Vapocoolant Spray vs Lidocaine-Prilocaine for IV Cannulation Pain
- EMA EDITOR’S COMMENTARY: This relatively straightforward randomized trial indicated no difference in pain reduction during IV placement between the use of a vapocoolant spray and lidocaine-prilocaine cream among adult ED patients. If these treatments really have equal performance, vapocoolant spray is actually the clear winner from a practical perspective, because its immediate onset of action affects procedural time, efficiency, and flow, and the study indicated its higher patient acceptability for future use. The real question is how much added value these treatments provide over using nothing at all; this aspect was not addressed in this study but would influence the ability to recommend routine use.
EMCrit 404 – Facial Trauma
July 19, 2025 by Scott Weingart, MD FCCM
Look Me in the Face and Tell Me That I Needed to Be Transferred: Defining the Criteria for Transferring Patients with Isolated Facial Injuries [10.1097/TA.0000000000004651]
Bellal Joseph, MD FACS
Dr. Bellal Joseph is the Martin Gluck Endowed Professor of Surgery, Professor of Neurosurgery, Chief of General Surgery and Chief Division of Trauma, Critical Care, Burns & Emergency Surgery, at the University of Arizona. He is also the Vice Chair of Research for the Department of Surgery.
Imaging
Who are you getting specific Face CTs on?
- Anyone with external signs of trauma or with facial tenderness
- Scott also gets it on any super sick patient
Who are you getting temporal cuts on?
- Anyone with a temporal bone fracture
Transfer of Facial Trauma (Facial Injury Guidelines)
Upper Facial Bone Fxs
Frontal Sinus Fractures
- All should get transferred
- Look for cerebrospinal fluid (CSF) rhinorrhea
- All are going to get either observation or operation
Middle Facial Bone Fxs
Radiology Tip: if there is no opacification of the maxillary sinuses, then the only fracture you will miss is a nasal bone fracture
Orbital Fractures
Transfer if decreased visual acuity, diplopia, restricted ocular motility, retrobulbar hemorrhage, or comminuted fracture
Zygomatic Arch, Nasal Bone, Maxillary Sinus Fractures
May need drainage of septal hematoma
Easier to reduce nasal fractures when swelling goes down
Alveolar fracture doesn’t preclude discharge
Zygomaticomaxillary Complex Fractures
Here the complex refers to the components of the fracture pattern, not the complexity
aka quadripod fracture or quadramalar fracture
Transfer if diplopia or decreased visual acuity (On the show, we agreed, decreased ocular motility as well)

Transfer Naso-Orbito-Ethmoid Fractures (NOE) these fxs connote a high mechanism injury
Le Fort Fractures

Type I – Do not transfer
Type II/III – transfer
Lower Facial Bone Fxs
Maxillary Alveolar and Hard Palate Fractures
Do not transfer
Speak with consultants for malocclusion–depends on ability to get the pt in for follow-up
Mandibular Fractures

Transfer bilateral mandibular fractures or condylar fractures
Soft Tissue Injuries
Transfer if >2cm of flap defect or missing tissue, neurologic signs/symptoms, eyelid or globe laceration
Neuro signs and symptoms include loss of sensation, paresthesia, and facial muscle weakness
Additional Tips
Remember to Check the Hearing
Some of these fractures and penetrating injuries can affect the auditory apparatus
Midface Hemorrhage
First10 EM
None
NEJM
Self-Neglect in Older People — A Clinical, Social, and Ethical Dilemma
- Consider consulting APS for patients with self-neglect that don’t qualify for admission.
Tirzepatide as Compared with Semaglutide for the Treatment of Obesity
- Tirzepatide (Zepbound) more effective than Semglutide (Ozempic/Wegovy)
Intravenous Tenecteplase before Thrombectomy in Stroke
- Patients with CVA<4.5hrs did better with lytics before thrombectomy than thrombectomy without lyrics.
REBELEM
MDCalc Wars: Stop Before the CT! — Are You Using PERC or Wells Correctly

{kind=link}