Academic Emergency Medicine
- The 3 most common diagnoses (BV, Trich and Vaginal Candidiasis) have poor sensitivity by microscopy so consider empirically treating after shared decision making.
- sensitivities for microscopy to detect BV, TV, and Candida were 76.8%, 68.6%, and 56.9%
- For NAAT, sensitivities were 92.8%, 96.5%, and 90.2%, respectively.
- In light of these practical realities, empirical single- dose oral tinidazole treatment of both BV and TV (with single- dose fluconazole) would offer a patient- centered solution to optimize the chance for first- time cure, particularly for women challenged by medication adherence and follow-up capability
Validation of the Sudbury Vertigo Risk Score to risk stratify for
a serious cause of vertigo
- On MDCalc
Annals of Emergency Medicine
EMCRIT
EMCrit 405 – Paracentesis – the EMCrit (Easy) Way
- Adenosine 12mg right up from, like defibrillator we should give adenosine big
- Aortic Dissection Detection Risk Score (ADD-RS) of 0 or 1
- Highly sensitive D-dimer of less than 500 ng/mL FEU
- Emergency physicians can exclude acute nontraumatic AoD without obtaining advanced imaging (ie, CTA, MRI, or TEE).
EMCrit 407 – Massive Hemorrhage Protocol 2.0 with Petro
- Triggers Use ABC after 3 units.
- Transfuse Products 6 PRBC: 6 FFP: 1 Plateletpharesis Pack
- Once MHP arrives next units should be FFP to match the 3 units of PRBCs followed by 1 plateletpheresis pack for every 6 units of PRBCs and 6 units of FFP
- Calcium 1g with first unit of blood and then 1g per 4 units of PRBCs, maintain ionized calcium >1-1.2 mmol/L
- Targets
- Lab thresholds Hb >7, INR <1.8, Plt >50 (or >100 in ICH), Fibrinogen >1.5–2.
- TXA
- Tranexamic acid use Trauma: 2g early. Time CutOff – they still use 3 hrs, I really want it in within 1 hour to 90 minutes
- PPH: 1g then repeat.
- GI: avoid—can cause harm.
- Head Injury: Crash3 is ambiguous, Petro gives it, I do not
- Reanalysis of PATCH-Trauma proposes a 90 minute cut-off [10.1016/j.annemergmed.2025.06.609]
- Consensus Statement from ACEP and ACS-COT [40842057]. Give in pts getting blood, 2g slow IVP is fine
EASL Clinical Practice Guidelines for the management of patients with decompensated cirrhosis
- In patients with decompensated cirrhosis, the aetiological factor, should be removed, particularly alcohol consumption and hepatitis B or C virus infection as this strategy is associated with decreased risk of decompensation and increased survival (II-2,1).
- Neutrophil count and culture of ascitic fluid culture (bedside inoculation blood culture bottles with 10 ml fluid each) should be performed to exclude bacterial peritonitis. A neutrophil count above 250 cells/ll is required to diagnose SBP (II-2;1).
- Ascitic total protein concentration should be performed to identify patients at higher risk of developing SBP
- The SAAG (MDCALC!) should be calculated when the cause of ascites is not immediately evident, and/or when conditions other than cirrhosis are suspected (II-2;1).
- Cytology should be performed to differentiate malignancy-related from non-malignant ascites (II-2;1).
- Since the development of grade 2 or 3 ascites in patients with cirrhosis is associated with reduced survival, LT should be considered as a potential treatment option (II-2;1).
- ommendations
- A moderate restriction of sodium intake (80–120 mmol/day, corresponding to 4.6–6.9 g of salt) is recommended in patients with moderate, uncomplicated ascites (I;1). This is generally equivalent to a no added salt diet with avoidance of pre-prepared meals.
- If possible to slip scope through mouth do that, nasal intubation is a hassle in ICU
- Choose best nostril by testing listening at inhalation and exhalation by occluding each nostril, if no difference go on the right.
- Antisialagogue
- Oxmetazolline
- Lido 4%
- Lido cream 2% (Weingart says use the nasal airway but don’t follow how cream stays on the tube as you slide it in). Annals article says just have patient insufflate the cream in to the nostril.
- Insert 6.5 or 7.0 ETT (per Annals), beware of 6.0 ETT which get much shorter
- Insert tube before scope to confirm ETT will fit in nares, don’t want to find cords and then discover ETT doesn’t fit.
- Insert ETT to 12-13 cm per Annals
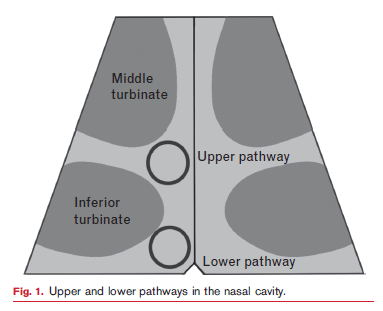
- Ride the Lower Passage to avoid the middle turbinate
Direct the Bevel-Up to select the lower pathway
Lift the tip of the nose
Aim as caudad as possible!
EMRAP
- CT scans performed in the U.S. in 2023 alone might eventually result in more than 100,000 new cancer diagnoses, representing 5% of all new cancer cases.
- In moderate severe COPD (pCO2>60 and pH 7.0-7.35, HVNI was noninferior to NiPPV in relieving dyspnea 4 h after therapy initiation. HVNI may be a reasonable treatment option for some patients experiencing moderate acute exacerbations of COPD in the ED. Vapotherm and HVNI equivalent per OpenEvidence.
- Neurocritical Care Mailbag: TBI Management
- Brain Injury Guidelines (BIG)
- Background
- BIG 1:
- Mild injuries with normal serial neurologic exams, no intoxication, and no major risk factors
- No anticoagulation/antiplatelet use
- Types of injuries:
- Small hemorrhages:
- Subdural hematoma (SDH) or epidural hematoma (EDH): ≤4 mm
- Single intraparenchymal hemorrhage (IPH): ≤4 mm
- Trace subarachnoid hemorrhage (SAH)
- No intraventricular hemorrhage (IVH)
- No skull fractures
- Small hemorrhages:
- Management: 6-hour ED observation, no repeat head CT, no neurosurgical consult
- Disposition:
- Safe for discharge if stable
- Possibly saves hospital admission (no patients required upgrades in the original study)
- BIG 2:
- Moderate injuries with mild risk factors (eg, intoxication, non-displaced fracture, slightly larger hemorrhages)
- No anticoagulation/antiplatelet use
- Types of injuries:
- SDH or EDH: 5 to 7 mm thick
- Single IPH: 5 to 7 mm or IPH in ≤2 locations
- Localized SAH
- No IVH
- Non-displaced skull fractures permitted, no depressed skull fractures
- No midline shift, mass effect, or herniation
- Disposition:
- Hospital admission, but no repeat CT or neurosurgical consult unless condition worsens
- Possibly saves transfer
- In the study, 9 out of 313 patients (2.9%) required upgrades:
- 7 for worsening head CT
- 2 for worsening exam
- None required neurosurgical intervention
- BIG 3:
- Severe injuries requiring close monitoring, repeat CT scans, and neurosurgical evaluation
- Patients on antiplatelets or anticoagulants were included in BIG 3 for original study
- Management: Admission to a higher level of care, full neurosurgical evaluation
- BIG 1:
- Validation of BIG:
- BIG was validated in a 2022 multicenter study of 2,300 patients, showing that no BIG 1 patients clinically worsened, and only 2 out of 295 BIG 2 patients experienced clinical deterioration.
- In this external validation study, BIG guidelines would have reduced
- CT scans by 29% overall
- 100% reduction for BIG 1 patients
- 98% reduction for BIG 2 patients
- Significant reduction in admissions and neurosurgical consults
- CT scans by 29% overall
- Limitations and considerations:
- Emergency physicians may be hesitant to discharge patients with visible bleeding on CT scans.
- Direct-acting oral anticoagulants(DOACs) are more common today but were not included in the original study.
- Neurosurgeons are already informally following these guidelines in many hospitals.
- Hospitals without in-house neurosurgery can avoid unnecessary patient transfers by using BIG for risk stratification.
- Encouraging collaboration among emergency medicine, neurosurgery, and critical care teams is essential to integrating BIG into hospital protocols.
- REFERENCES:
- The BIG (brain injury guidelines) project: defining the management of traumatic brain injury by acute care surgeons
- Joseph B, Friese RS, Sadoun M, et al. J Trauma Acute Care Surg. 2014;76(4):965-9. doi: 10.1097/TA.0000000000000161. PMID: 24662858.
- In this innovative trial, the authors did not observe improved clinical outcomes among patients with acute decompensated heart failure with significant pleural effusion who were treated with thoracentesis rather than standard medical management.
First10 EM
None
NEJM
A Gilded Age for Patients? The Broken Promises of Profit-Driven Medicine
Dismantling Public Health Infrastructure, Endangering American Lives
Progress Lost — The Unraveling of Medicaid and the Affordable Care Act
The Resurgence of Private Law in American Health Care
REBELEM
MDCalc Wars: Sorting Out Syncope – Which Rule Should You Trust?
- The San Francisco Syncope Rule is quick and easy to apply, but its inconsistent performance and poor external validation limit its reliability as a stand-alone tool. In contrast, the Canadian Syncope Risk Score is more comprehensive and has been more robustly validated, offering stronger risk stratification. However, it comes with added complexity and a degree of subjectivity, reminding us that no decision tool replaces sound clinical judgment.
ICARUS ED Trials Albumin for Undifferentiated Sepsis in the
Emergency Department
- Based on the best available current evidence, including this trial, albumin provides no meaningful clinical benefit in the resuscitation of septic patients.
