Contents
_____________________________________________________________________________________________
Definition
_____________________________________________________________________________________________
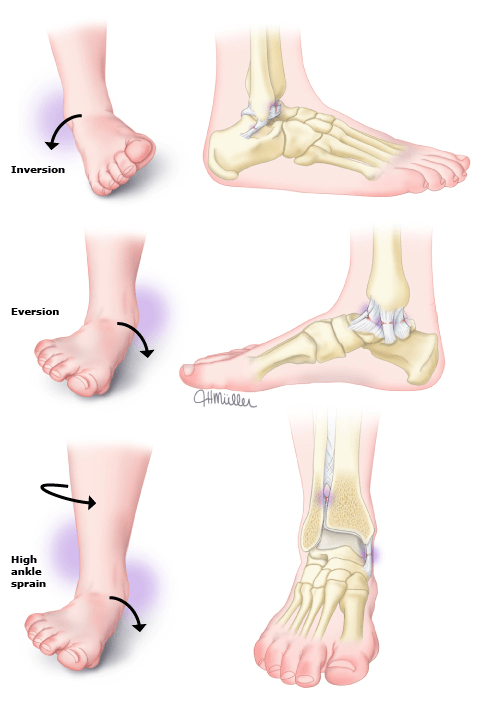
Lateral ankle sprain: most common, inversion injury causing damage to the lateral ligament complex (anterior talofibular, calcaneofibular and posterior talofibular ligaments.
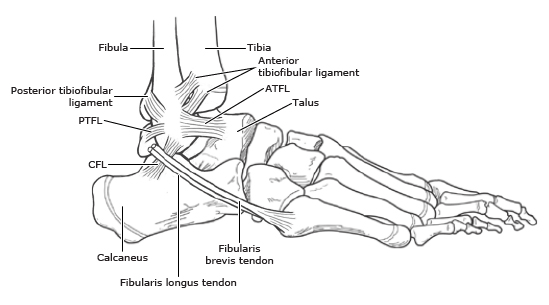
Medial ankle sprain: deltoid ligament, strongest ligament of the ankle, infrequently injured, more typically eversion injury causes a medial malleolus avulsion fracture.
Syndesmotic sprain (high ankle sprain)– dorsiflexion and external rotation or eversion may cause sprain of the syndesmotic structures (tibiofibular ligaments). These injuries contribute to ankle instability and are more to lead to result in recurrent ankle sprains.
Grade 1 sprain– results from mild stretching of a ligament with microscopic tears. Patients have mild swelling and tenderness. There is no joint instability on examination, and the patient is able to bear weight and ambulate with minimal pain. Due to their benign nature, these injuries are not frequently seen in the office.
Grade 2 sprain- incomplete tear of a ligament, moderate pain, swelling, tenderness, and ecchymosis. Weightbearing and ambulation are painful.
Grade 3 sprain- complete tear of a ligament, severe pain, swelling, tenderness, and ecchymosis. Patients may not be able to bear weight or ambulate.
_____________________________________________________________________________________________
Clinical Evaluation
_____________________________________________________________________________________________
History
- Mechanism is key to determining if the injury is medial or lateral or high ankle.
- Whether the patient could walk after the injury- stratify the risk of fracture and need for X-rays.
- History of prior ankle sprain.
Exam
- Inspect; swelling, ecchymosis?
- Palpate:
- Check for fracture of the proximal fibula (Maisonneuve)
- Check distal 6cm posteriorly of tibia and fibula for Ottawa rule
- Check 5 MT and achilles tendon (document Thompson test if tendon is tender)
Special Tests
- Squeeze Test-
- compression of the fibula and tibia at mid calf elicits pain in the anterior tibiofibular ligament anterior to the lateral malleolus and proximal to the ankle when patient has a high ankle sprain


With a syndesmosis sprain, pain occurs in the region of the ruptured anterior tibiofibular ligament (location indicated by the tip of the pen). Also shown are the locations of the anterior talofibular ligament (A) and the calcaneofibular ligament (B).
- Anterior drawer test-
- detects excessive anterior displacement of the talus on the tibia. If the anterior talofibular lateral ligament is torn by an inversion stress, the talus will sublux anteriorly and laterally out of the mortise. The test is performed with the patient’s foot in the neutral position (slightly plantarflexed and inverted). The lower leg is stabilized by the examiner with one hand, and with the opposite hand, the examiner grasps the heel while the patient’s foot rests on the anterior aspect of the examiner’s arm. An anterior force is gently but steadily applied to the heel while holding the distal anterior leg fixed

Deferred examination — Deferred examination may improve the diagnosis of ligamentous injuries and instability [4]. As an example, a study of 160 consecutive patients with inversion injuries found that performing a physical examination five days after the injury improved the accuracy of diagnosing ligament rupture [22]. The positive predictive value for ligament rupture of the triad of pain on palpation of the anterior talofibular ligament, lateral discoloration due to hematoma, and a positive anterior drawer sign was 95 percent.
_____________________________________________________________________________________________
Diagnostic Testing
_____________________________________________________________________________________________
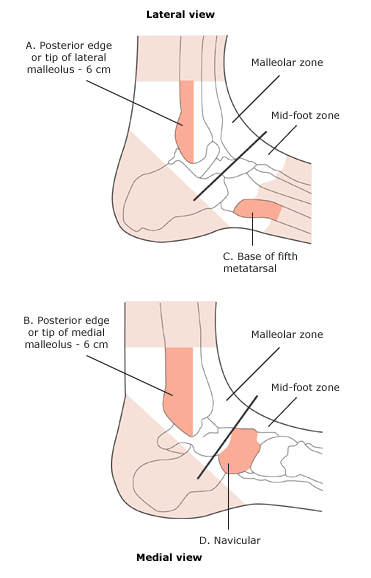
Ottawa Ankle Rules
- Plain radiographs of the ankle are only indicated for patients who have pain in the malleolar zone and
- Have bone tenderness at the posterior edge or tip of the lateral or medial malleolus
- or
- Are unable to bear weight both immediately after the injury and for four steps in the emergency department or doctor’s office
- Plain radiographs of the foot are only indicated for patients who have pain in the midfoot zone and
- Have bone tenderness at the base of the fifth metatarsal or at the navicular
- or
- Are unable to bear weight both immediately after the injury and for four steps in the emergency department or doctor’s office
- If the patient can transfer weight twice to each foot (four steps), he or she is considered able to bear weight even if he or she limps
_____________________________________________________________________________________________
Treatment
_____________________________________________________________________________________________
- Protection, rest, ice, compression, and elevation (PRICE) is a common-sense approach for the first two to three days, although formal study of its effectiveness is lacking.
- Protection is provided by applying an elastic bandage and, depending on the extent of injury, a splint, walking boot, or possibly a cast.
- Rest is achieved by limiting weightbearing; if needed, patients use crutches until they are able to walk with a normal gait.
- Ice or cold water immersion is recommended for 15 to 20 minutes every two to three hours while awake for the first 48 hours or until swelling is improved, whichever comes first.
- Compression with an elastic bandage to provide support and minimize swelling should be applied early.
- Elastic ankle sleeve makes the most sense to me because you can put a shoe over the sleeve.
- Elevate to further alleviate swelling. Ideally, the ankle should be kept above the level of the heart, but this may be difficult to achieve.
Immobilization
- Not needed for grade 1 and 2
- Favored for grade 3 severe sprain for a short period (10days) in a non-weightbearing cast.
_____________________________________________________________________________________________
Return to sports
______________________________________________________________________________________________
- Pain and swelling have substantially improved or resolved
- The athlete can complete in-office static balance and side hop test without instability.
- The athlete can perform sport-specific movements at full speed without instability, significant pain or subsequent (next-day) swelling.
_____________________________________________________________________________________________
Key Concepts
_____________________________________________________________________________________________
- Determine mechanism of injury: dorsiflexion and external rotation suggests a high ankle sprain which is more commonly associated with chronic instability and recurrent sprains.
- Exam less useful in the acute phase, may be able to identify a high ankle sprain the mid calf squeeze test.
- Grade of sprain interesting but not consistently predictive of how recovery time.
- Treatment:
- Protect against further injury by crutches and if severe a splint/cast.
- Rest- return to activity when swelling improving and no longer painful
- Ice 15-20 minutes every 2-3 hours while awake x 2 days
- Compression- compression ankle sleeve
- Elevate
______________________________________________________________________________________________
References
_____________________________________________________________________________________________
UPTODATE: Ankle Sprain in Adults. May 2023.
