Management of Acute Type B Aortic Dissection– NEJM Sept 2025
Definitions
Acute aortic syndrome: acute aortic dissection, intramural hematoma, and penetrating aortic ulcer are three distinct entities encompassed by the clinical diagnosis of an acute aortic syndrome.
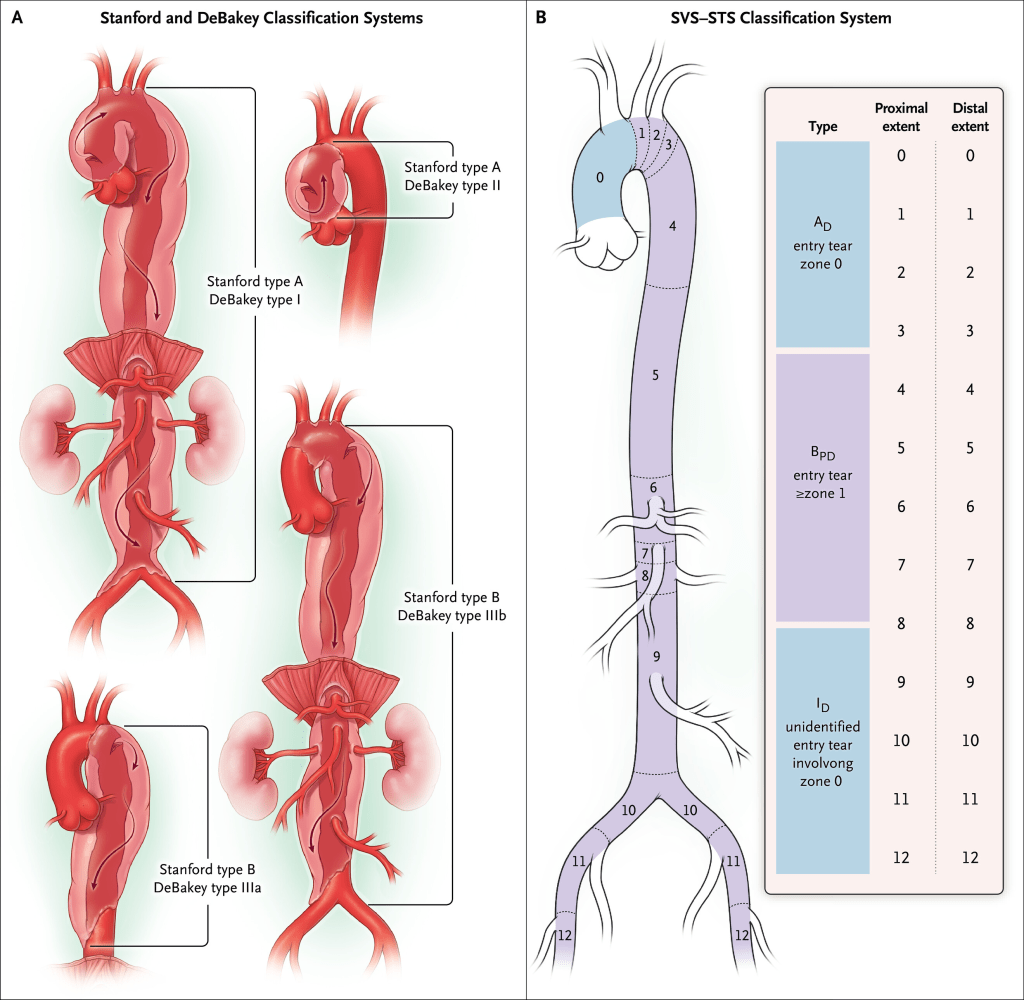
Stanford Type A Aortic Dissection: dissection involving the ascending aorta (defined as the aorta proximal to the inominate artery), regardless of where the original intimal tear occurs. The dissection involves an intimal tear, sometimes preceded by medial degeneration, causing separation of the intima from the media in an antegrade and retrograde manner. This creates two (or occasionally more) channels where the blood can flow outside the true lumen of the aorta, and complications arise if the blood flow into the aortic side branches becomes compromised.
Stanford Type B Dissection: a dissection that does not involve the ascending aorta.
Epidemiology
- Mean age is 63yo
- Men predminantly affected
- Risk factors:
- uncontrolled hypertension
- connective tissue diseases
- genetic aortopathy
- smoking
- blunt trauma
- use of cocaine or meth
- Delayed diagnosis is not uncommon
- 2/3 of dissections are Type A
Treatment
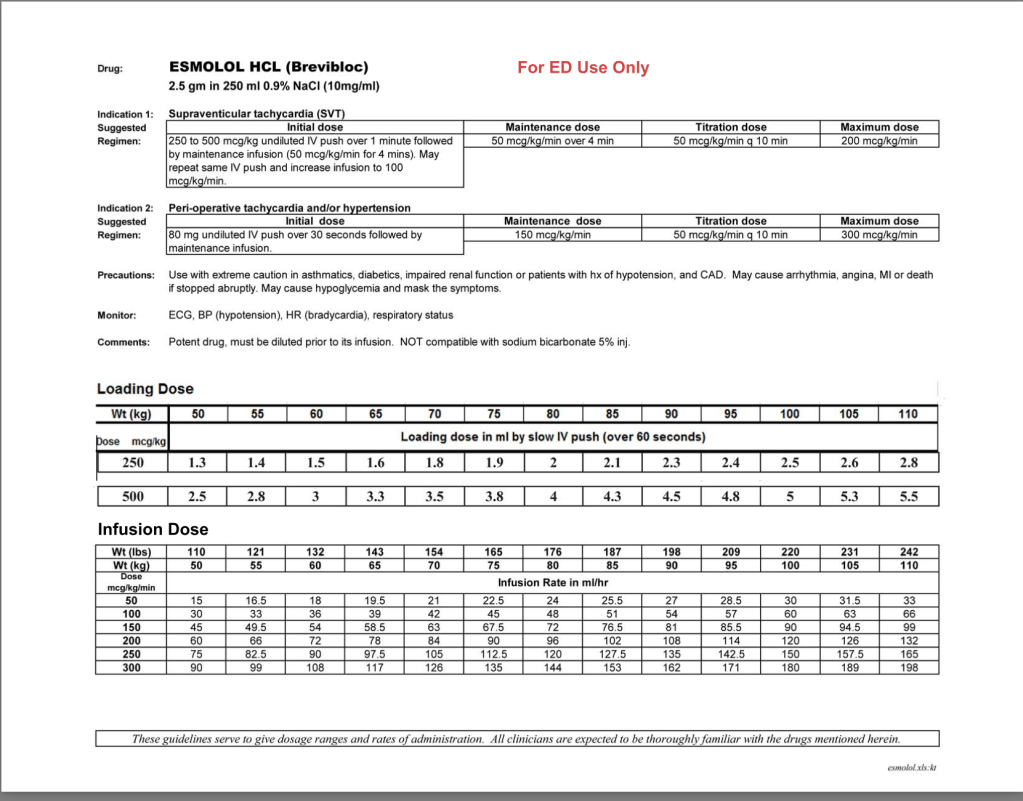
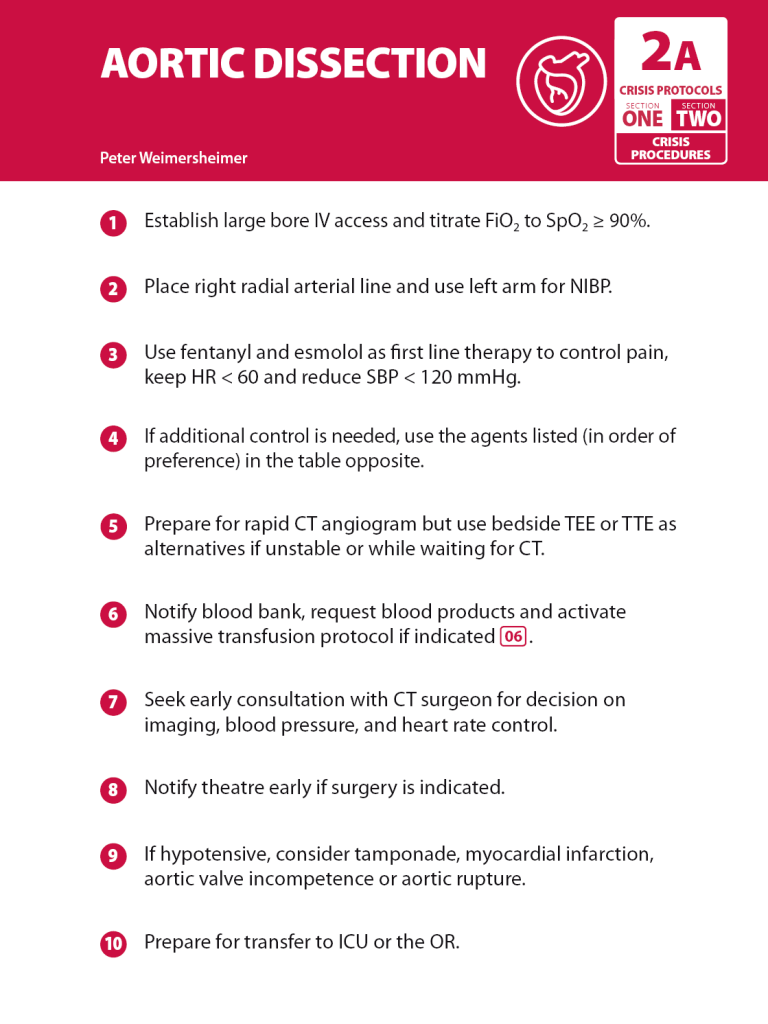
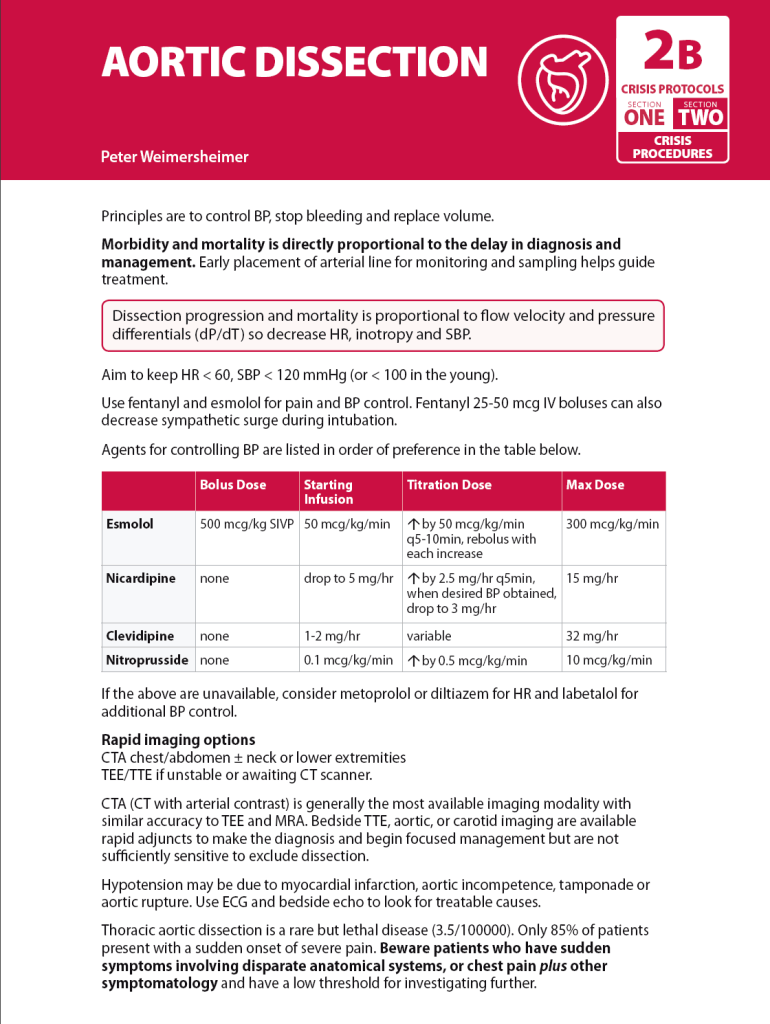
- Control pain- Weingart recommends Fentanyl bolus and drip
- B blockers- esmolol (drip sheet)
- Nicardipine drip
- Goal is HR<60, SBP<120