Contents
- Definition
- Epidemiology
- Pathogenesis
- Clinical Presentation
- Physical Exam
- Labs
- Indications for Imaging
- Differential Diagnosis
- Diagnosis
- Treatment
- Disposition
- Key Concepts
- References
_____________________________________________________________________________________________
Definition
_____________________________________________________________________________________________
- Diarrhea is defined as three or more unformed liquid stools per day (stool that takes the form of the container in which it is placed).
- Dysentery: inflammation of the intestine, particularly the colon, causing diarrhea with blood and mucus, generally associated with fever, abdominal pain and rectal tenesmus (the sensation of incomplete defecation).
- Acute (<7 days)
- Prolonged (7 to 13 days)
- Persistent (14 to 29 days)
- Chronic (>30 days).
_____________________________________________________________________________________________
Epidemiology
_____________________________________________________________________________________________
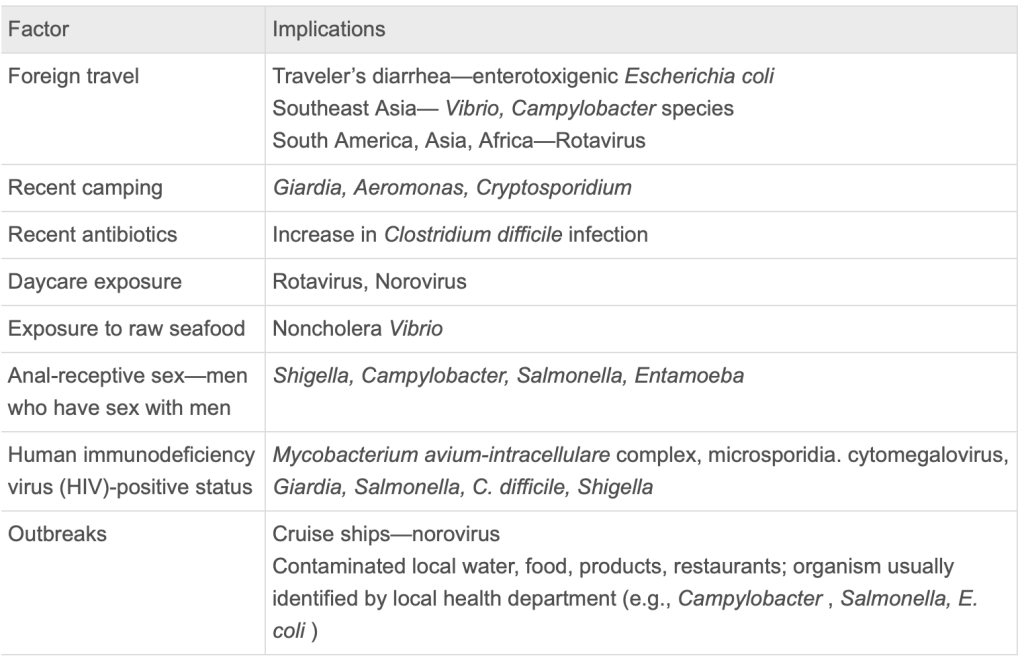
- Gastroenteritis frequency is increasing due to increased international travel, mass production of foods and the increased consumption of raw produce such as spinach and fresh fruits.
- Diarrheal deaths in developed countries are usually in elderly and c diff and norovirus are most frequently implicated.
- Acute and prolonged gastroenteritis (</=13days) usually viral or bacterial causes.
- Persistent and chronic gastroenteritis (>13 days) is often caused by protozoans, parasites, or noninfectious conditions.
_____________________________________________________________________________________________
Pathogenesis
_____________________________________________________________________________________________
- 4 mechanisms:
- ingestion of preformed toxins
- adherence of infectious pathogens to intestinal cell walls
- invasion of mucosal cell walls
- production of enterotoxins and cytotoxins
- Each mechanism leads to increased fluid secretion or decreased fluid absorption in the GI tract.
_____________________________________________________________________________________________
Clinical Presentation
_____________________________________________________________________________________________
- GI sxs after short incubation (1-6 hours) suggest preformed Staph or Bacillus toxins.
- Diarrhea more than 2 wks suggests Giardia/parasites or IBD
- Norovirus causes sudden onset of severe vomiting and only moderate diarrhea
- Large volume diarrhea suggests small bowel involvement such as viral gastroenteritis or Vibrio cholerae.
- Colonic involvement causes smaller volume but bloody.
- Campylobacter or shigella cause dysentery.
- Yersinia mimics appy.
- Scombroid: spoiled dark meat (tuna, mahi mahi) causes bacterial growth which break down the flesh of the fish releasing large amounts of histamine. Allergic sxs and diarrhea minutes to hours after eating the fish.
- Foul smelling stools and bloating and flatulence and cramping and diarrhea > 2 weeks suggests Giardia, often a h/o camping.
- Most patients with invasive AGE recover within 1 week although diarrhea can last for an extended period.
Shiga-Toxin Producing E Coli
- Produces Shigella-like toxins
- Major cause of hemorrhagic colitis, HUS or TTP.
- Inadequately cooked beef has caused many large outbreaks.
_____________________________________________________________________________________________
Physical Exam
_____________________________________________________________________________________________
- Digital rectal exam can be performed to assess for gross blood, mucus, rectal lesions in the setting of blood or mucus in the stool or complaints of rectal pain.
_____________________________________________________________________________________________
Labs
_____________________________________________________________________________________________
- Routine labs not needed in many cases
- Indications for labs:
- High fever
- Severe abdominal pain
- Bloody stool
- Persistent diarrhea (>/=14d)
- Elders with abdominal pain (>/=65yo)
- Immunocompromised
_______________________________________________________________________________
Indications for Imaging
- Per Uptodate, imaging not typically indicated with acute diarrhea unless patients have significant peritoneal signs or ileum (abdominal distension?) where there is a concern for toxic megacolon, perforation, obstruction, abscess or fulminant colitis.
- Rosen recommends CT for patients with C Diff colitis who are older, appear septic, have a high WBC or have a tender distended abdomen.
_____________________________________________________________________________________________
Differential Diagnosis
_____________________________________________________________________________________________
- Appy
- Chole
- Pancreatitis
- SBO
_____________________________________________________________________________________________
Diagnosis
_____________________________________________________________________________________________
- Stool cultures for Salmonella, Shigella, Campylobacter, Yersinia, Shiga-toxin producing E coli (STEC) and C Diff may be considered for patients with
- Severe illness
- Fever of >/=38.5 (101)
- Dysentery
- Immunocompromised
- Recent hospitalization
- Recent antibiotic use
_____________________________________________________________________________________________
Treatment
_____________________________________________________________________________________________
- Ondansetron .15mg/kg up to 8mg PO or IV (side effects HA and diarrhea)
- Oral rehydration unless severe dehydration
- Pedialyte
- Diluted fruit juice
- Chicken broth
- Gatorade
- Food, if possible, promotes mucosal recovery and improves fluid absorption.
- Imodium (loperamide) for adults, not kids
- 4mg with first dose, then 2mg per loose stool up to 16mg/day.
- Avoid in dysentery unless also starting abx
- Antibiotics not indicated for the majority of AGE
- Empirical Antibiotics indicated for:
- Toxic
- Febrile
- Dysentery/Bloody Stools
- Uptodate acknowledges the concern for treating bloody stools with abx given the possibility of STEC as the causative pathogen but they feel abx may still be warranted because:
- Most cases of bloody diarrhea are not STEC
- Risk of HUS and TTP has been predominantly reported in kids
- Thus the benefit of abx in severe bloody diarrhea may outweigh the risk of complications from treating STEC
- Do not give abx if the risk of STEC is higher such as in an afebrile patient or known STEC outbreak.
- Uptodate acknowledges the concern for treating bloody stools with abx given the possibility of STEC as the causative pathogen but they feel abx may still be warranted because:
- Severe traveler’s Diarrhea
- Suspected C Diff
- Immunocompromised
- Prosthetic grafts
- Azithromycin 500mg QD x 3d or
- Second line: Cipro 500mg PO BID x 3-5d (higher resistance)
_____________________________________________________________________________________________
Disposition
_____________________________________________________________________________________________
- Most patients can be managed as outpatients
- Hospitalization:
- Toxic
- Severe or persistent symptoms
- Inability to tolerate POs
- Significant electrolyte abnormalities
- Severe dehydration
- Special consideration to patients at the extremes of age or immunocompromised
_______________________________________________________________________________
Key Concepts
______________________________________________________________________________
- AGE is usually self-limited and most patients require no testing.
- Patients with fever, bloody stools, sepsis, severe dehydration, suspicion for C Diff or immunocompromised state should generally get CBC, electrolytes, and stool cultures.
- Oral rehydration with pedialyte or diluted juices or broth or gatorade is recommended over IVF unless dehydration is severe.
- Ondansetron .15mg/kg up to 8mg PO or IV is safe and effective.
- Normal feeding is recommended, promotes mucosal recovery.
- Campylobacter and Salmonella are the top two causes of culture-proven bacterial enteritis in developed countries.
- Norovirus is the most common cause of AGE in kids and adults.
- 80% of traveler’s diarrhea is bacterial, ETEC (enterotoxigenic EColi) is the most common etiology.
- Antibiotics prolong shedding of Salmonella and can worsen STEC so not recommended in most AGE.
- Uptodate recommends abx reasonable in adults with bloody diarrhea with fever since STEC complications are primarily reported in kids and STEC less likely with fever (especially >/=101).
- Classic food poisoning is usually 1-6 hours post ingestions due to preformed toxins from Staph, Bacillus and Clostridium Perfringens, no live organisms, self-limited.
- C Diff risk factors include recent antibiotics (1-4 weeks), recent hospitalization, long term care facility, solid organ transplant, the use of antacids.
- CT for patients with suspected c diff who are older, septic, high wbc or tender distended abdomen.
_______________________________________________________________________________
References
_____________________________________________________________________________________________
Rosen’s Emergency Medicine: Concepts and Clinical Practice. Tenth Edition. 2023. Chapter 80- Gastroenteritis. Authors: Thomas Nguyen and Saadia Akhtar.
UPTODATE: Approach to the adult with acute diarrhea in resource-rich settings. Empiric Antibiotic Therapy, Indications. Authors: LaRocque and Harris.
