_____________________________________________________________________________________________
Preparation
_____________________________________________________________________________________________
- List of supplies
- High-risk deliveries:
- Maternal conditions: old or young moms, maternal diabetes or hypertension, maternal substance use disorder, previous history of stillbirth, fetal loss, early neonatal death
- Fetal conditions: prematurity, post maturity, congenital anomalies, intrauterine growth restriction, multiple gestations
- Antepartum complications: placenta previa or abruption, oligohydramnios or polyhydramnios
- Delivery complications: transverse lie or breech presentation, chorioamnionitis, foul smelling or meconium-stained amniotic fluid, antenatal asphyxia with abnormal fetal heart rate, maternal administration of a narcotic within 4 hours of birth, deliveries that require instrumentation (forceps)
_____________________________________________________________________________________________
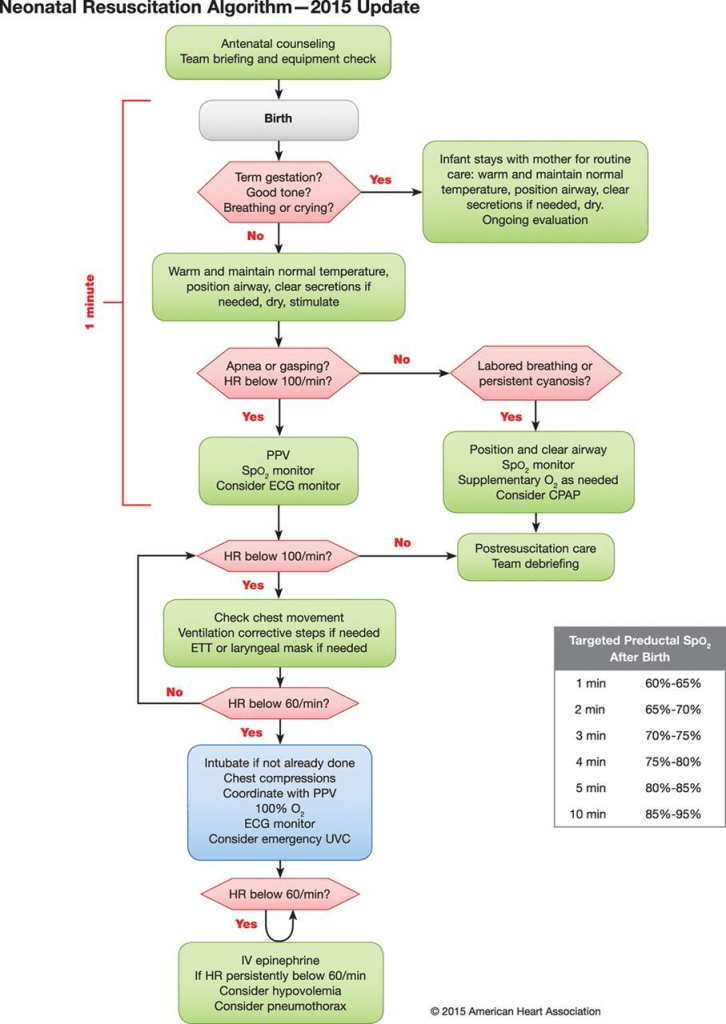
Newborn Resuscitation
_____________________________________________________________________________________________
_____________________________________________________________________________________________
Interventions
_____________________________________________________________________________________________
Temperature Control
- Skin to skin contact with mom if possible
- Drying and wrap in warm blanket or towel
Airway
- Positioning– for infants requiring further intervention, the infant is positioned flat on their back with head in a neutral position to slightly extended position (if needed a small rolled blanket or towel may be placed under the infant’s shoulder to slightly extend the neck to maintain an open airway.
- Suctioning– suctioning immediately after birth is reserved for babies with obvious obstruction due to secretions and as needed for those who require positive pressure ventilation to clear any mucous to prevent aspiration prior to delivery of assisted breaths. Mouth is suctioned first and then the nares to decrease the risk for aspiration.
- Meconium stained amniotic fluid– In the presence of meconium-stained amniotic fluid (MSAF), routine intrapartum nasopharyngeal suctioning and/or endotracheal suctioning post-delivery are not recommended. Care of these neonates is the same as for those without MSAF.
Monitoring
- Pulse Oximetry– when PPV used, supplemental oxygen used or cyanosis
- Heart Rate– ecg monitoring best, more accurate than pulse ox to monitor hr
Oxygenation
- Use room air
- PPV- for apnea, gasping or hr<100
- Give breaths at a rate 40-60 bpm: “breathe, two three, breathe, two, three”.
LMA
- May be better than BMV but studies are conflicting
Intubation
- Indications:
- BMV is ineffective or prolonged
- Chest compressions are being performed
Chest Compressions
- Indication: HR remains<60 bpm despite adequate ventilations for 30 seconds.
- Technique:
- Compressions 3 to 1 with breath after third compress: “one, two, three, breath”
- Imaginary line between nipples and xiphoid
- Apply pressure with two thumbs
- Compressions 3 to 1 with breath after third compress: “one, two, three, breath”
- Increase oxygen to 100% during cpr, wean down if rosc.
- Reassessment after 60 seconds of CPR and PPV: HR, color, respiratory effort
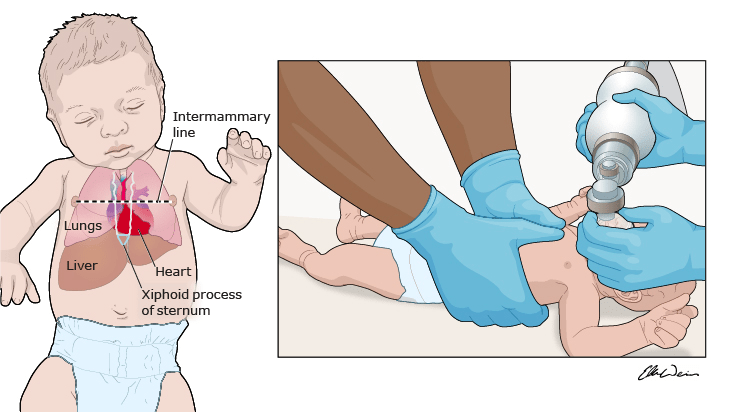
The thorax is encircled with the hands and cardiac compressions are performed with both thumbs. The compression site is approximately one finger’s breadth below the intermammary line. The area over the xiphoid process should be avoided to prevent injury to the liver, spleen, or stomach.
Epinephrine
- Indication: ongoing bradycardia (HR<60) despite adequate ventilation and chest compressions.
- Dose:
- Via IV: IV epinephrine .01-.03mg/kg (can use 5kg weight so give .05-.1 mg which is .5- 1ml of 1:10000)
- Via ETT: .05-.1mg/kg (can use 5kg weight so give 2.5-5ml via ETT)
Discontinuing Resuscitation
Resuscitation efforts may be discontinued after 20 minutes of effective resuscitation including intubation and the use of epinephrine if the neonate has demonstrated no signs of life (no heart beat or respiratory effort for>20 minutes).
_____________________________________________________________________________________________
References
_____________________________________________________________________________________________
Uptodate October 2023, Neonatal resuscitation in the delivery room, Author C Fernandes.
