Defintion
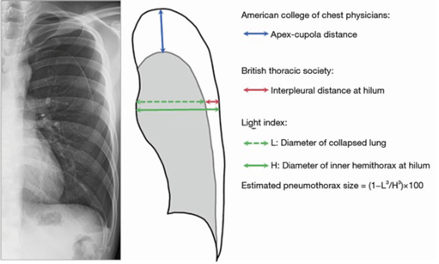
Large: differing definitions:
- ACCP: >3cm apex-cupola distance
- BTS: >2cm inter pleural distance at hilum
- Belgian guidelines: dehiscence over the entire length of the lateral chest wall
Causes
- Primary spontaneous- no underlying lung disease
- Classically tall, thin males
- Marfan syndrome
- Ehlers Danlos
- Homocytinuria
- Alpha-1 antitrypsin deficiency
- Secondary spontaneous- history of underlying lung disease
- Asthma, COPD, Blebs, Lung abscess, Pulmonary infarct, Malignancy
- Traumatic
- Penetrating
- Blunt (10% of blunt trauma patients found to have ptx, 68% occult)
- Iatrogenic
- Central Line, NG tube placement, Barotrauma (mechanical ventilation, scuba divers)
Management
Primary Spontaneous Pneumothorax – no known underlying lung disease
- Small
- Patients with small primary spontaneous pneumothorax who have stable vital sign and are mildly symptomatic can be observed in the ED with a repeat CXR at 4 hours
- If the pneumothorax appears stable, they can be safely discharged home with a repeat x-ray in 24-72 hours
- It is reasonable to provide supplemental oxygen while waiting for repeat CXR as there is retrospective data suggesting that it may hasten lung expansion
- Large
- Conservative approach
- Patients < 50yo
- Mildly symptomatic
- Stable vitals: Sat>90, Normal BP (not defined), HR<120/>60, RR<24, speaking in full sentences
- Shared decision making with patient
- If repeat CXR is stable at 4 hours, pt can be discharged home with repeat CXR in 24-72 hours.
- Interventional approach
- >/=50yo
- PTX increasing
- Unstable vitals, too symptomatic
- Patient preference
Secondary Spontaneous Pneumothorax– due to underlying lung disease
- Small
- UPTODATE says most patients with SSP require thoracostomy because they have underlying lung disease, more prone to prolonged air leak, failure of aspiration and tension pneumothorax.
- Conservative Approach
- Small PTX (<2cm from lung apex to parietal wall)
- Minimal or no symptoms
- Have a low threshold to admit
Traumatic Pneumothorax
- Small
- Conservative Approach
- UPTODATE describes the 35mm rule proposed by Eddine, J Trauma Acute Care Surg 2019
- </=35mm cutoff on CT using the radial dimension from parietal to visceral pleura of the largest air pocket is a safe threshold for conservative management
- only 9% of these patients ultimately required drainage
- If CT not otherwise indicated, UPTODATE does not recommend CT just to evaluate a small PTX.
- Discuss with CT Surgery their preference
- UPTODATE describes the 35mm rule proposed by Eddine, J Trauma Acute Care Surg 2019
- Thoracostomy Approach
- Unstable
- Large PTX
- Ventilator
- Conservative Approach
- Large
- Pigtail catheter, chest tube not necessary, per EMCRIT
Pigtail Catheter Insertion
Contraindications
- Unstable patient, go to chest tube
- Empyema, probably need a chest tube
- Located pleural effusion
- Coagulopathy not a contraindication per Weingart
Prep patient
Location
- Triangle of safety
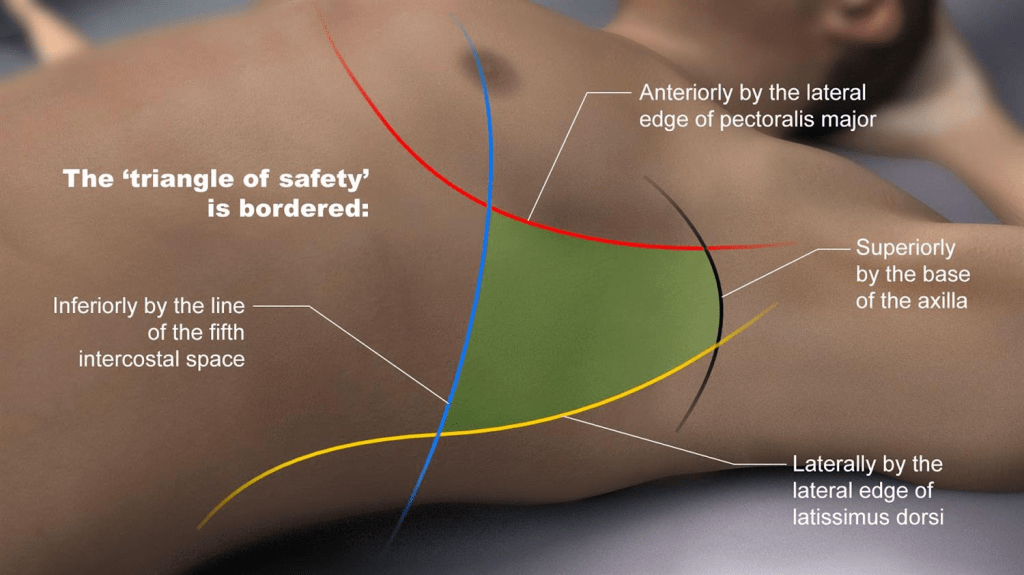
- 4th ICS safer than 5th ICS
- Bottom of the axilla
- Can use midpoint of upper arm
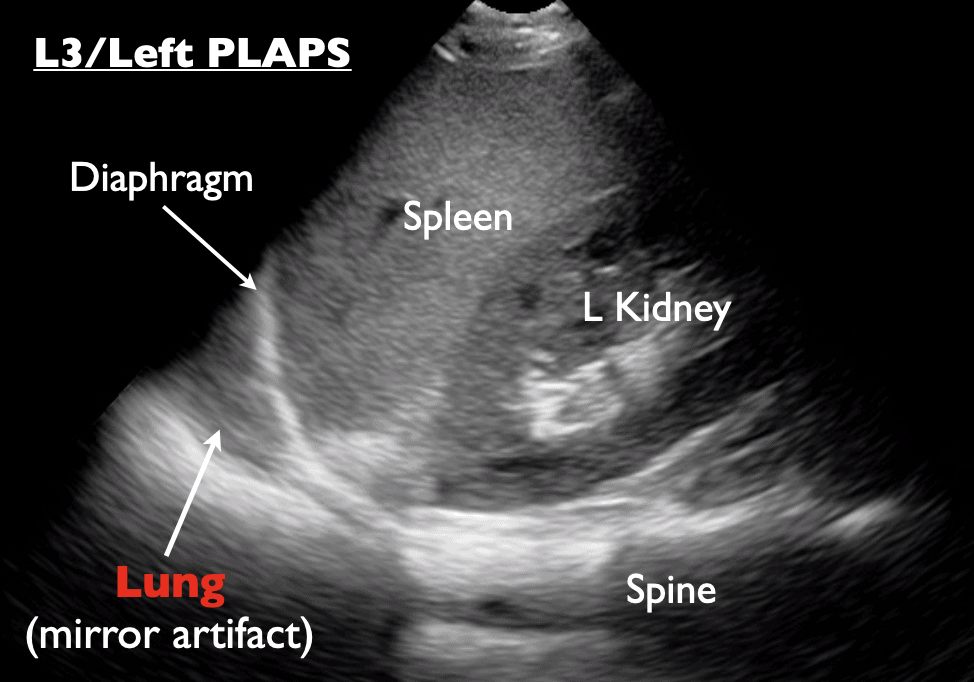
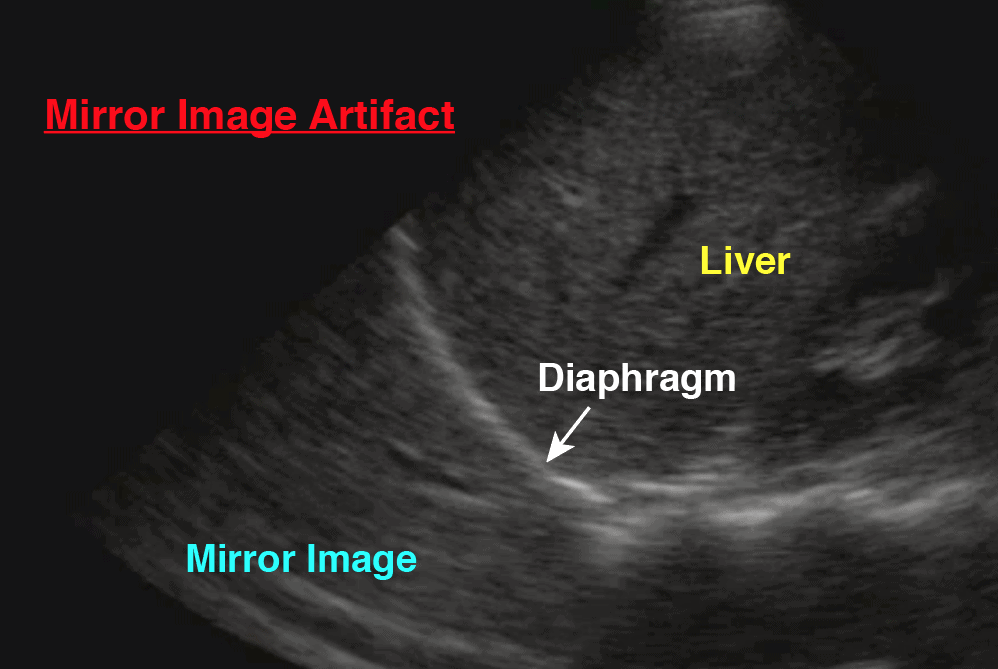
- Always use ultrasound to confirm you’re on the pneumothorax side and confirm you are above the diaphragm and no adhesions or vessels , mark with an X.
Sterilely Prep
- Prep the area around the X
Anesthetize
- 20cc of Lidocaine 1% with epi
- Large wheal at the skin surface
- Find the top of the rib, slowly insert as you aspirate, once you get air then withdraw slightly and once you feel resistance you can inject between innermost muscle layer and second layer, this is where the neuromuscular bundle lies, found as soon as needle withdraws out of pleural space and you feel resistance.
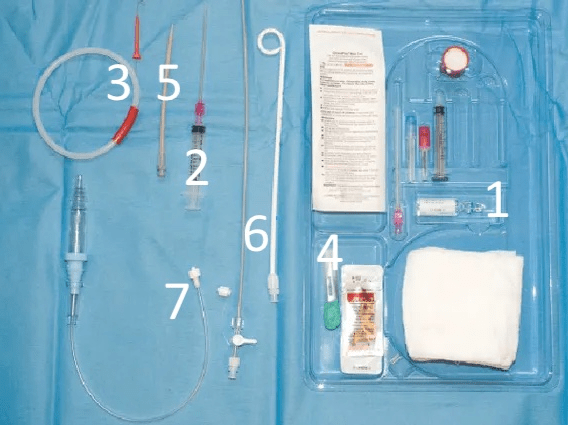
Different Pigtail Kits
- Seldinger Technique
- Thoracic Vent (e.g. Uresil Tru-Close)
- Trocar Technique (video instruction)
Seldinger Technique Supplies
- Suture kit with 3.0 ethilon suture
- Sterile gloves
- Sterile gown
- Pigtail kit
Procedure
- Thread long internal dilator into the pig catheter and then lock it into place.
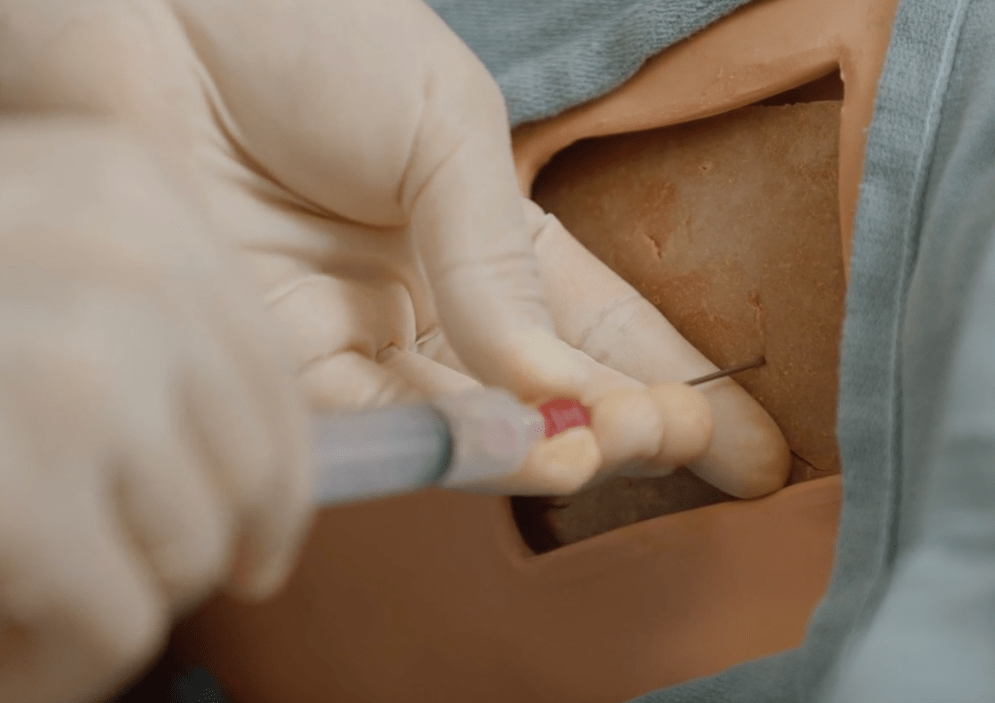
- Insert needle above rib until air is aspirated. Pay attention to how deep needle was when you aspirated air.
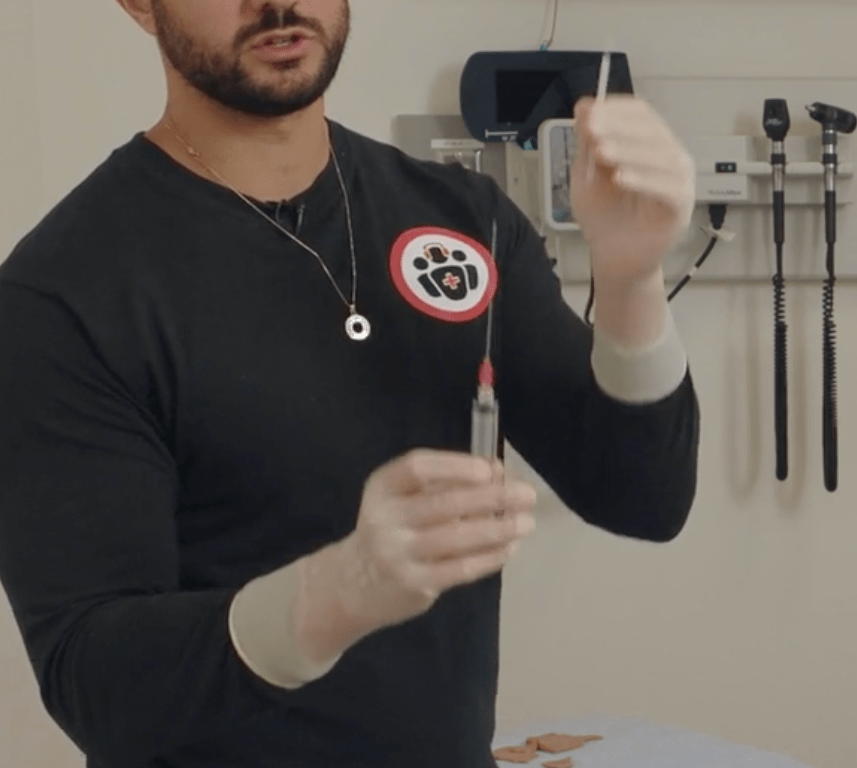
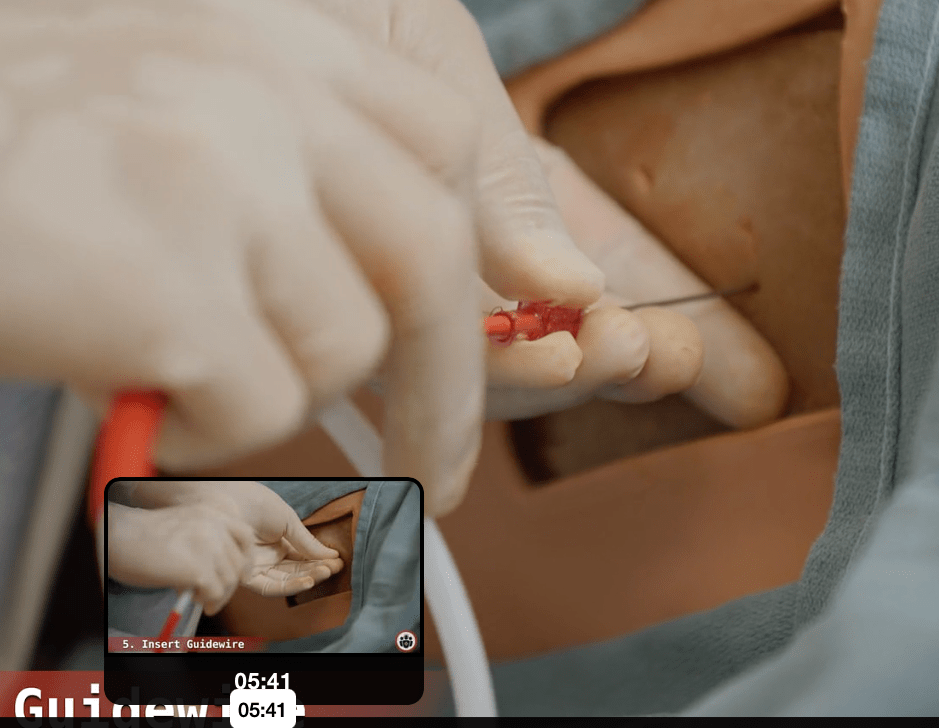
- Remove syringe and advance wire through the needle.
- Remove the needle.
- Make a nick at the wire and ensure the wire moves freely in the larger hole.
- Advance short dilator over the wire, then twist, pull and pinch (twisting on the dilator as you pull back on the dilator which allows dilator to grab and tear fascia through the twist and pull but pinching on the wire from behind so wire doesn’t get pulled out.
- Remove short dilator
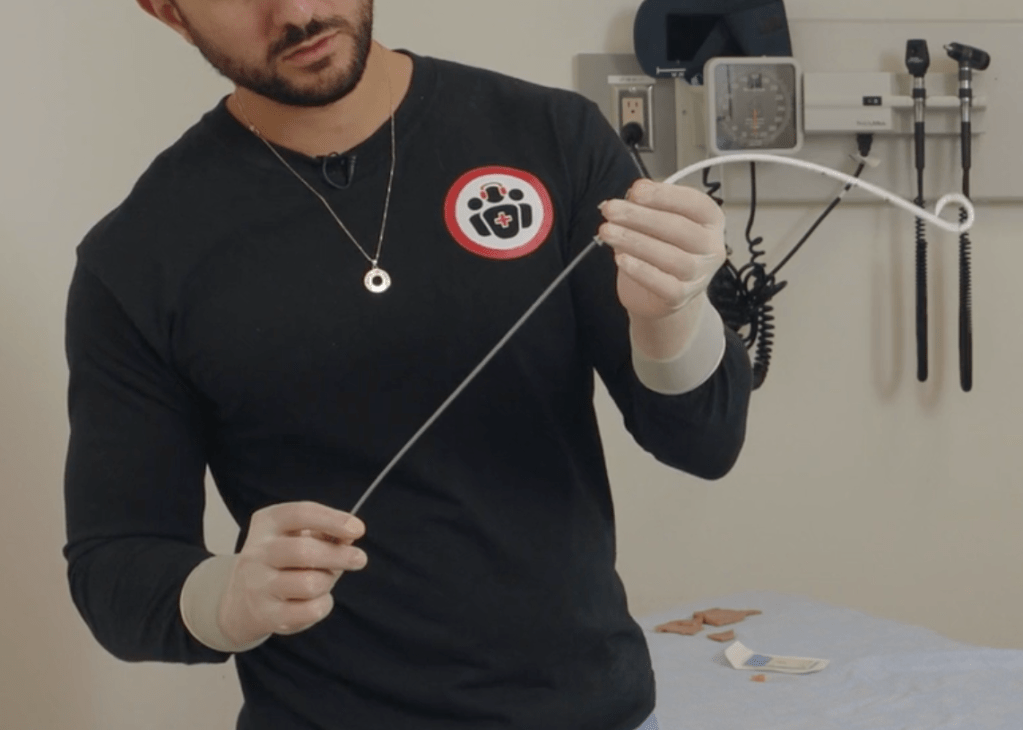
- Advance pigtail with internal dilator over the wire, stopping at the first or second line,
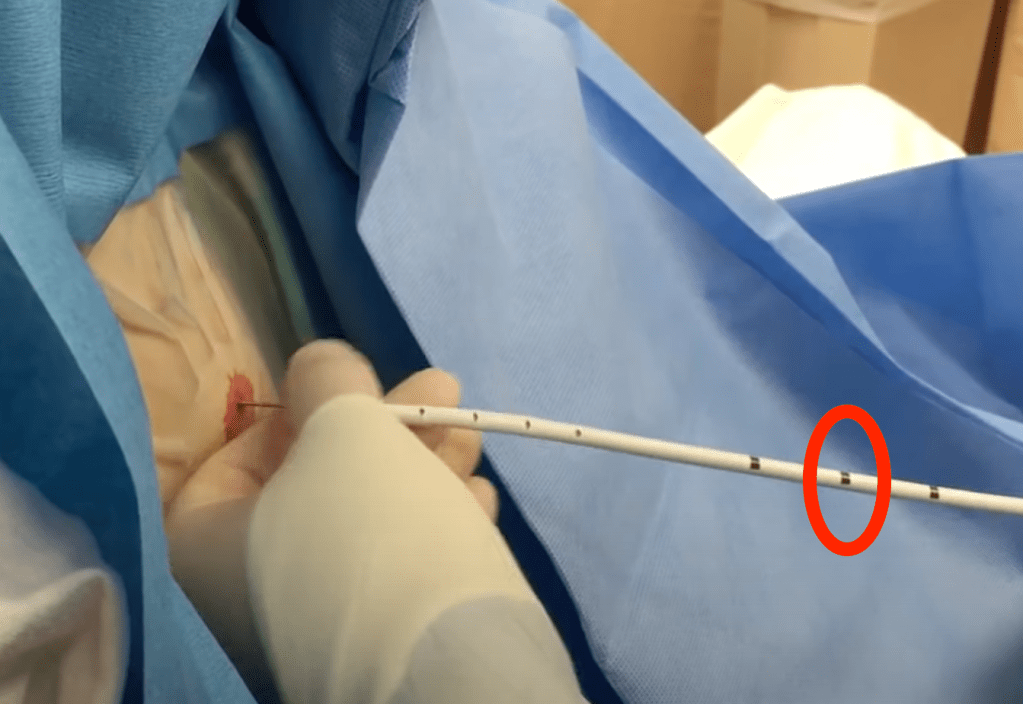
- Then advance the pigtail further while holding on the the internal dilator and wire so those do not advance. Weingart advances to third line on the pigtail.
- Remove wire and dilator.
- Confirm easy aspiration of air.
- Connect extension tubing to end of pigtail while capping the open port.
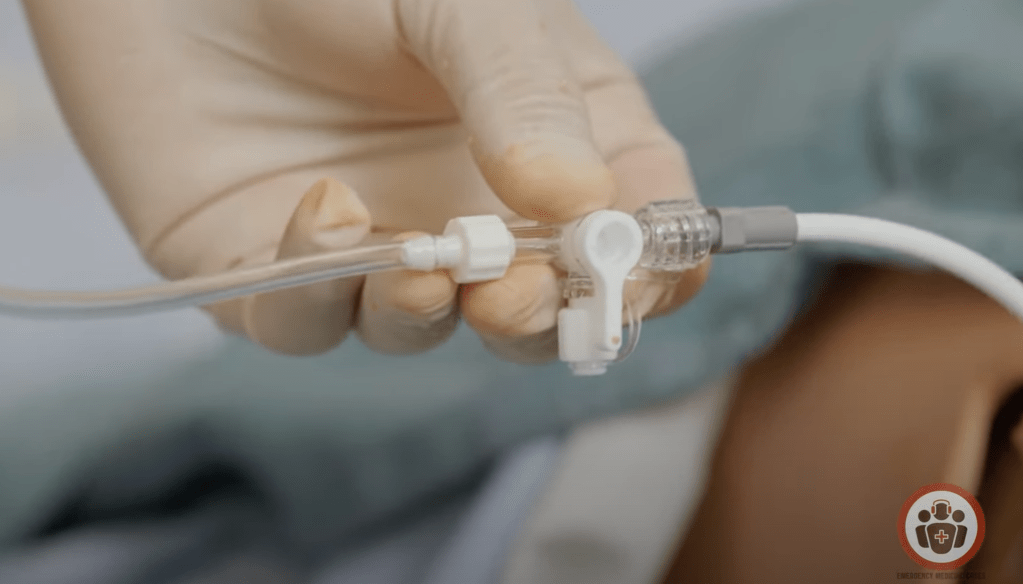
- Make sure the stopcock direction is off to the side port, as pictured above, so that it is open to the tubing going to the pleur-evac.
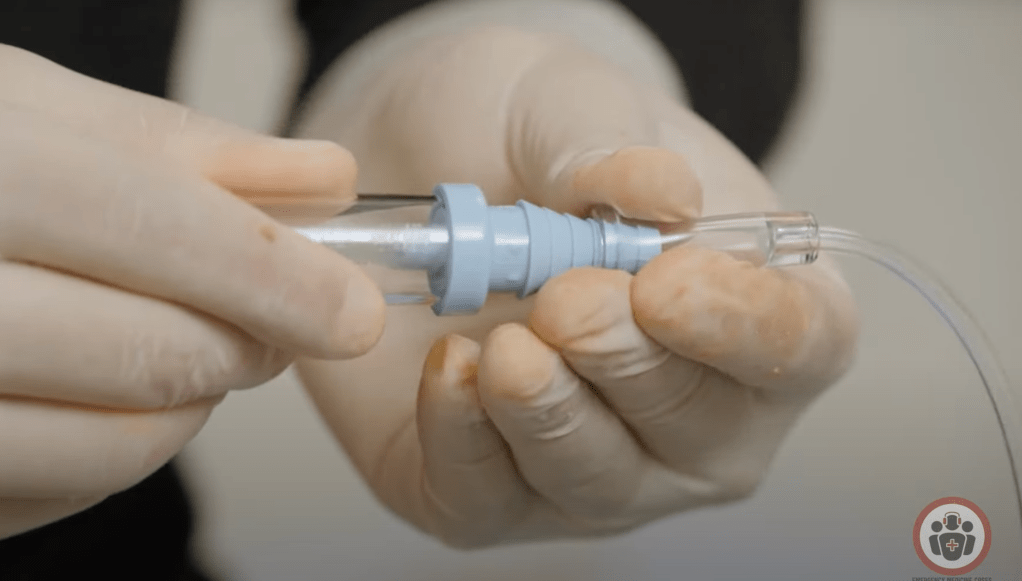
- Connect the Blue side of the Heimlich valve to the pigtail catheter to ensure air flow is out of the thorax (there is writing on the valve that directs you if you forget).
- The heimlich valve can then be be connected to the pleur-evac and left to water seal or suction with 20cm.
- Suture the pigtail in place: Take a bite of tissue and throw three knots, leaving two long tails, then wrap those tails snugly around the catheter and throw three more knots.
