Contents
- Definition
- Epidemiology
- ED Evaluation and Management
- Management of Hemorrhage
- Management of Infection
- Complications of Cervical Dilators
- Amniotic Fluid Embolism
- Uterine Perforation
- Self-managed Abortions
- Patients Requesting an Abortion Reversal
- Key Concepts
- References
_____________________________________________________________________________________________
Definition
_____________________________________________________________________________________________
Self-Managed Abortion
- Abortion attempted outside the formal healthcare system
Medical Abortion
- Early termination of pregnancy through medication
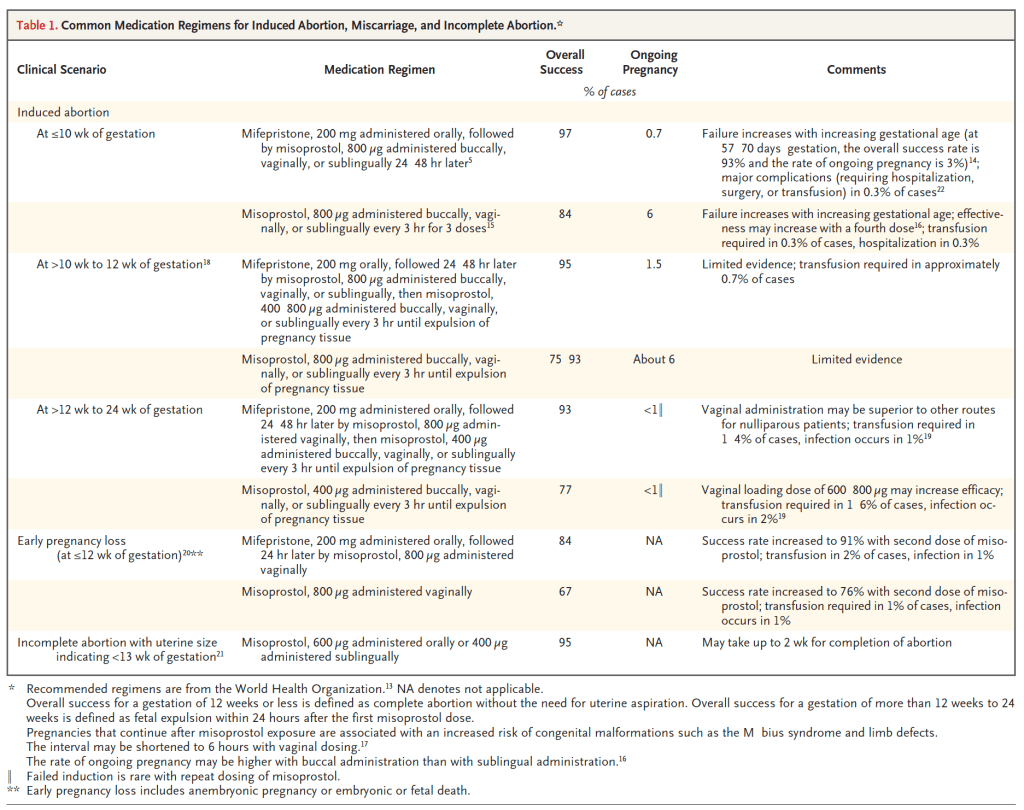
- Can be used until 70 days of gestation
- 2 drug regimen: Mifepristone 200mg PO (progesterone antagonist) followed by Misoprostol 800 ug bucally/sublingually/vaginally 24-48 hours later
- Mifepristone disrupts the pregnancy growth and misprostol causes uterine contractions to expel the pregnancy tissue with an efficacy rate of 96%
- Can be administered at home
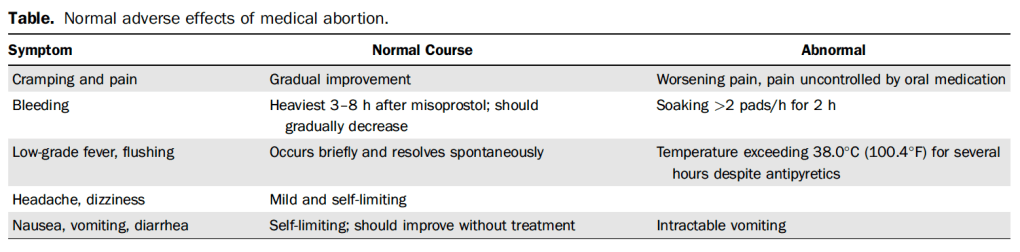
- Adverse effects
- cramping and vaginal bleeding
- brief low-grade fever and chills on the day Misoprostol is used
- headache, dizziness
- N/V/D
Surgical Abortion (First Trimester)
- First trimester surgical abortion is performed with vacuum aspiration (suction curettage but NOT sharp curettage).
- Misoprostol (Cytotec) sometimes used to ripen the cervix.
- Routine prophylactic antibiotics is the standard of care but should not be continued after the day of the procedure.
Surgical Abortion (Second Trimester)
- Second-trimester surgical abortions make up a small portion of total abortions with only 8.8% of all abortions in 2015 being greater than 13 weeks gestation
- Procedure:
- Cervical dilation
- Osmotic dilator is placed in the cervix the day before and expands as it absorbs fluid from the cervix
- Misoprostol administered 90-180 minutes before the procedure, generally safe
- Amniotic fluid is aspirated
- Fetus is grasped and removed with forceps
- Suction aspiration to ensure complete uterine evacuation
- 85% of these procedures use moderate sedation
- Cervical dilation
_____________________________________________________________________________________________
Epidemiology
_____________________________________________________________________________________________
- 11.8 abortions per 1000 women aged 15-44 yrs
- 65% of abortions were obtained at or before 8 weeks of gestation
- 73% of abortions are surgical but the proportion of early medical abortions increased 114% from 2006 to 2015
- Average out of pocket cost for women seeking abortions is $500
- Since 1976, the Hyde Amendment has limited federal funds for abortions to cases of maternal life endangerment, rape or incest
- 16 states have policies to use state based Medicaid to expand abortion coverage beyond federal restrictions, either voluntarily or with a court order
_____________________________________________________________________________________________
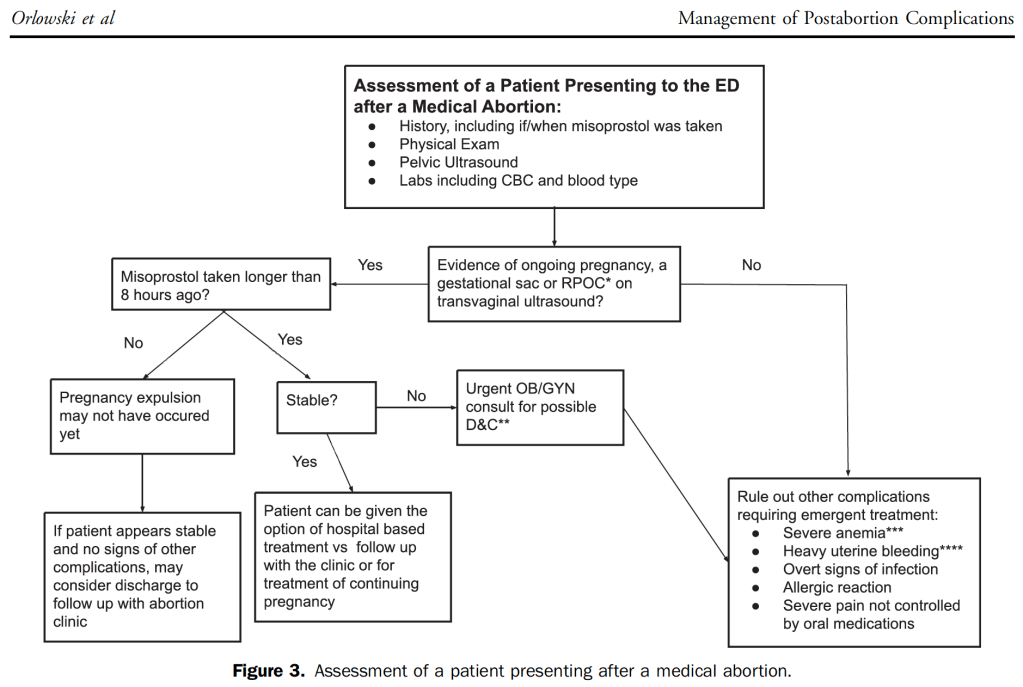
ED Evaluation and Management
_____________________________________________________________________________________________
History
- Gestational history
- Medical or surgical abortion?
- Medically supervised or self-managed abortion?
- Medications or cervical ripening agents (osmotic dilators)
- Contact the facility that performed the procedure to confirm details (if possible, many cases will present outside of clinic hours and may or may not have someone who can respond after hours)
- Medical history including any history of coagulation/bleeding disorders, diabetes, immunocompromised state?
Exam
- Perform a pelvic exam including speculum and bimanual exam (especially in cases of postabortion hemorrhage or possible infectious complications)
Labs
- Quant HCG (use for trending to rule out ectopic)
- CBC
- Type and Rh (Rhogam should be offered if Rh negative)
- CMP (recommended by NEJM article2, to look for toxic effects from self-managed abortions from ingestions)
- If hemorrhage:
- Coags
- If infection suspected:
- Blood Cultures
- Genital Cultures (bacterial aerobic cervical swab)
- Lactic Acid
- Coags, Fibrinogen and D-dimer (if DIC possible)
Pelvic Ultrasound
- Identify ongoing pregnancy
- Duration and site of pregnancy
- Adnexal mass
- Free fluid
- Echogenic material in the uterus or a thickened stripe commonly seen after a medical or surgical abortion and should not immediately trigger further intervention
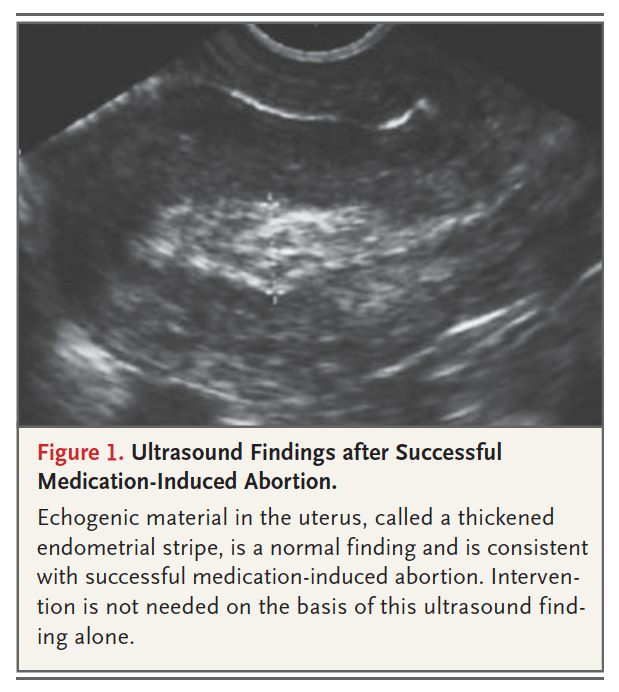
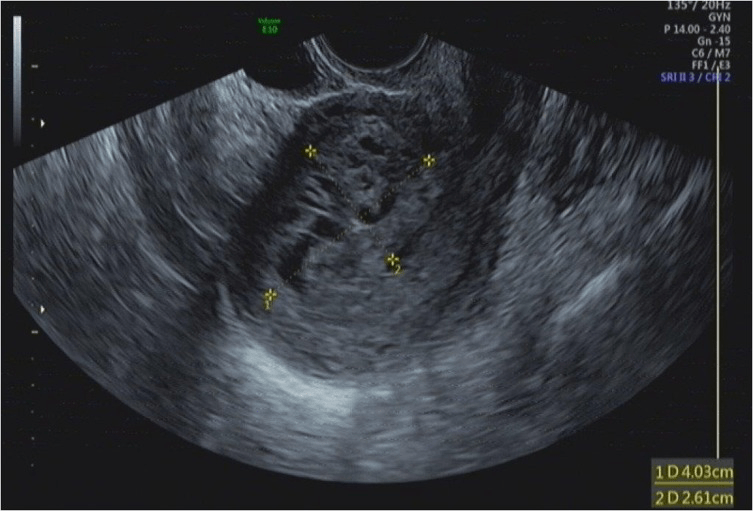
https://www.ejog.org/article/S0301-2115(18)30093-9/fulltext
Management
- Rhogam should be offered when the duration of gestation is unclear and patient is Rh negative (Rhogam may not be needed with a pregnancy < 56 days of gestation2)
- Hemorrhage management
- Infection management
Disposition
Discharge with abortion clinic follow-up can be considered for:
- Reassuring pelvic US (no gestational sac, no free fluid, no retained POC, no adnexal mass)
- Normal lab testing
- Benign exam
- Stable vitals
Emergency OB consult is necessary for:
- Evidence of retained products of conception > 8 hours after misoprostol
- Unstable vitals
- Severe pain not controlled by oral medicines
- Heavy bleeding (more than 2 pads/hour for 2 hours) or “significant” decrease in blood volume (not specified1).
- Severe anemia (not specified)
- Overt signs of infection
- Allergic reaction
- Concerning ultrasound (adnexal mass, free fluid)
Any postabortion patient who is discharged should be warned that they can become pregnant as soon as 10 days after an abortion, so early access to contraception is crucial.
- Immediate postabortion insertion of IUDs on contraceptive implants is an evidence-based effective practice.
- Patients who present to the ED postabortion may already have an IUD or implant in place.
_____________________________________________________________________________________________
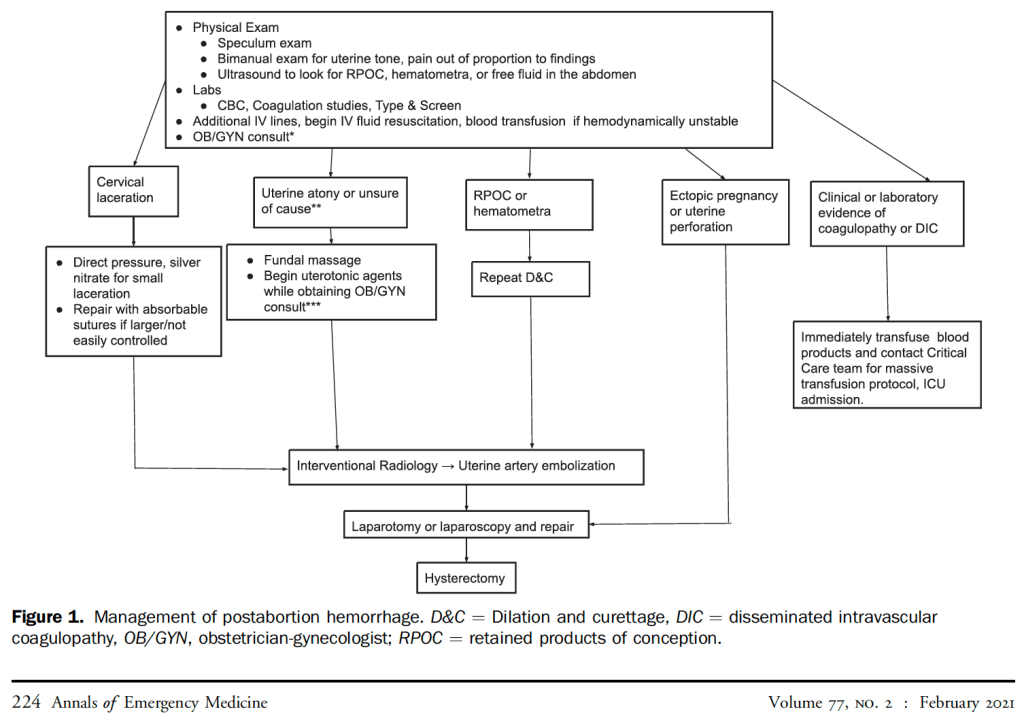
Management of Hemorrhage
_____________________________________________________________________________________________
Clinical Presentation
- Excessive bleeding is soaking through 2 pads per hours for at least 2 consecutive hours
- Heaviest bleeding is typically 3-8 hours after Misoprostol administration with a medical abortion as the tissue is expelled from the uterus and should then decrease
- Median duration of bleeding most women experience is 11-13 days although 25% of women bleed longer than 16 days
- Bleeding is typically heavier with a medical than a surgical abortion
- 5% of women who present to the ED for an abortion-related complication will require a transfusion.
Causes
- Uterine atony
- Cervical laceration
- Retained products of conception
- Uterine perforation
- Coagulopathy
- Less common
- Undiagnosed ectopic
- Uterine AVM
- Uterine artery pseudoaneurysm
Exam
- Pelvic Exam should performed to look for:
- Cervical lacerations
- Uterine atony (boggy uterus: enlarged, soft, tender)
- Quantity of bleeding
Labs
- CBC
- Type and screen
- Quantitative HCG (difficult to interpret but an 80% decrease in quant HCG 1 week after medical abortion is highly suggestive of a successful expulsion)
- Coagulation studies
Pelvic Ultrasound
May demonstrate:
- Retained products of conception
- Free fluid in the abdomen (suggests uterine perforation)
- Hematometra (accumulation of blood in the uterus)
Treatment
- Consult OB Gyn
- 2 large bore IVs
- IV fluids
- TXA 1gram IV should be “considered” according to Orlowski, Annals of EM2, TXA also recommended by UPTODATE for postpartum hemorrhage.
- TXA 1g IV may be repeated 30 minutes later if bleeding persists
- Tranfusion if hemodynamically unstable
- Begin with 2 units PRBCs
- If patient still unstable after 2 units of PRBCs, then activate the hospital’s Massive Transfusion Protocol with PRBC=FFP=Platelets (1 platelet pack, either apheresis pack from a single donor or pooled random donor concentrate from different donors, is equivalent to the platelets in 4-6 units of whole blood so one pack is given with each transfusion of 4-6 units of PRBCs)
- If cervical laceration
- Usually occur in the immediate postoperative period
- In the unlikely event that they are found in the ED, small ones can be treated with direct pressure and silver nitrate
- More extensive ones require suturing with absorbable suture (Gyn consult)
- If retained products or hematometra
- OB Gyn consult for repeat vacuum aspiration which allows the uterus to contract
- If uterine atony
- Fundal massage
- OB Gyn may recommend:
- Misoprostol 800-1000ug by rectum (safe)
- Methylergonovine 0.2mg IM (patients with hypertension should not receive)
- Carboprost (Hemabate) IM (not safe in asthma, active cardiac, pulmonary, renal or hepatic disease)
- If patient still unstable?
- OBGyn may recommend
- IR consult for uterine artery embolization
- Laparotomy or laparoscopy
- Hysterectomy
- OBGyn may recommend
_____________________________________________________________________________________________
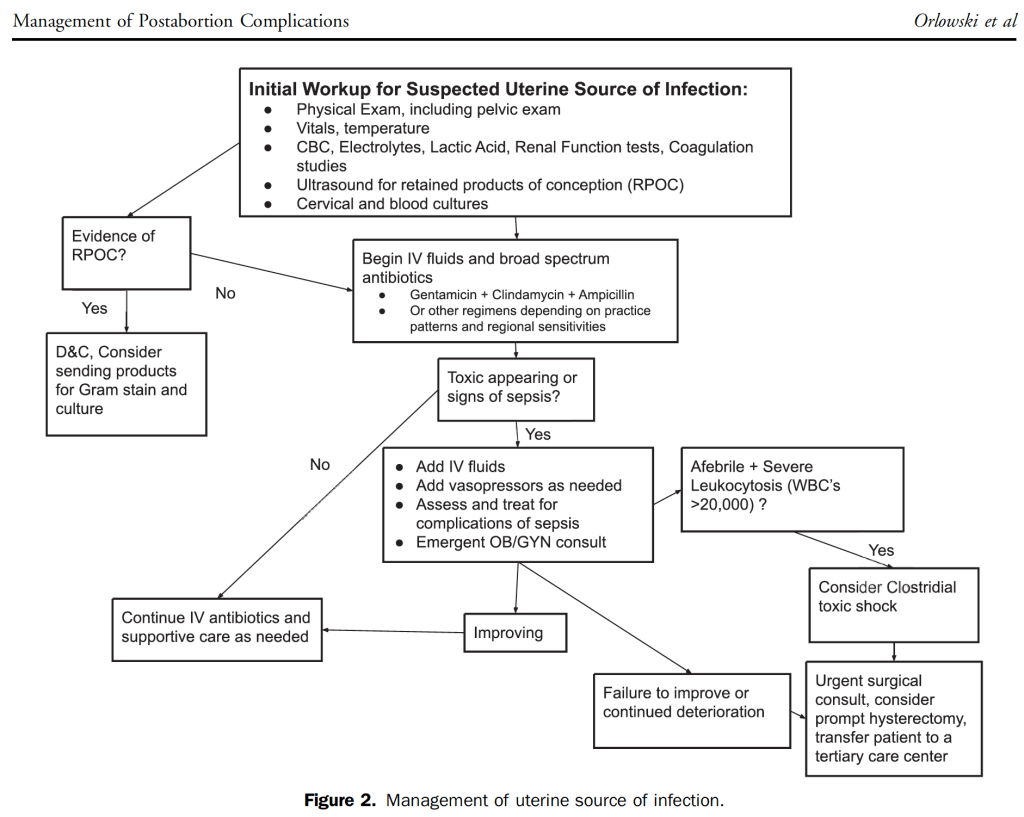
Management of Infection
_____________________________________________________________________________________________
Background
- Rates of infection are low: 0.016%-0.23%, but severity of infection can range from mild endometritis to fatal septic shock.
- Most cases are polymicrobial vaginal flora or preexisting infections (Chlamydia, Gonorrhea, Trichomonas)
- Most dangerous infections are group A strep and clostridial species
Evaluation of suspected postabortion infection
- Pelvic exam
- Labs: CBC, BMP, lactic acid, blood cultures, cervical cultures (order may be “genital culture”, send in aerobic bacterial culture transport medium), coagulation studies
- Pelvic ultrasound
Treatment
- Antibiotics (triple antibiotic regimen):
- Clindamycin and
- Gentamycin and
- Ampicillin or Unasyn
- Source control vacuum aspiration dilation and curettage if patient has retained products of conception
Clostridial Toxic Shock
- Leading cause of death after first-trimester abortion
- Rare (roughly 1 case per year in the US) but almost universally fatal condition
- Can occur postpartum or postabortion
- Presentation
- Abdominal pain/cramping
- N/V/D
- Initially nonspecific symptoms but progresses to septic shock
- Most patients are afebrile but have a massive leukocytosis (eventually >100k)
- Treatment
- Abx: Clindamycin and PCN
- Gyn surgical removal of the toxin source and consider hysterectomy
_____________________________________________________________________________________________
Complications of Cervical Dilators
_____________________________________________________________________________________________
- Rare complications:
- Bleeding
- Infection
- Allergic reaction
- Retained cervical dilators (shouldn’t happen because abortion physicians count cervical dilators on removal)
- Discovered when seen on imaging when a patient presents with pelvic pain and vaginal discharge
_____________________________________________________________________________________________
Amniotic Fluid Embolism
_____________________________________________________________________________________________
- Rare
- More commonly described during or immediately postpartum
- Pathogenesis is theorized to involve a breach in the maternal fetal barrier, with entry of amniotic fluid and fetal antigenic material into the maternal circulation
- Produces a cytokine storm with hypotension, acute dyspnea, desaturation, pulmonary edema, cardiovascular collapse and DIC.
_____________________________________________________________________________________________
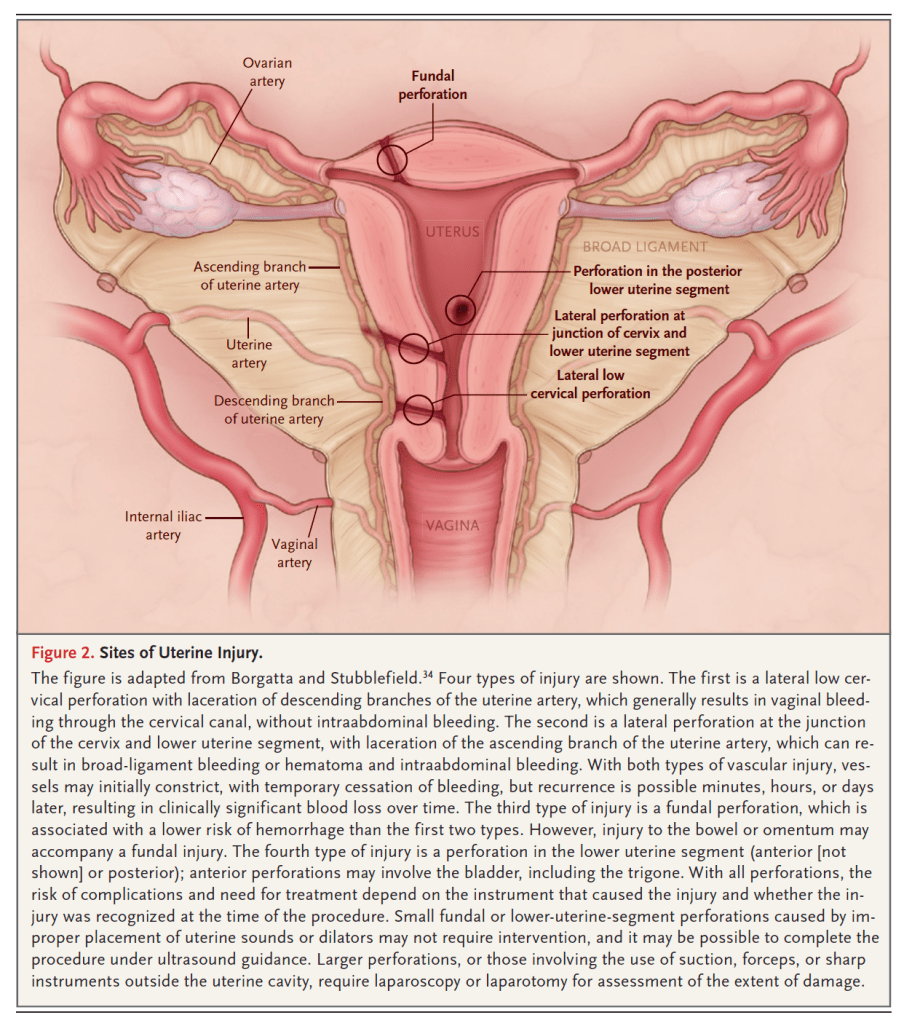
Uterine Perforation
_____________________________________________________________________________________________
- Rare
- Most cases require only observation, cases requiring intervention range from 0.1% to 2.3%
- Ultrasound is the best initial imaging study with findings including:
- Defects in the uterine wall
- Abnormal uterine contents
- Abdominal free fluid
- Visualized fetal tissue
- If perforation is suspected and US in inconclusive, abdomen/pelvis CT or MRI can be used
- Surgical management for complicated perforations may require OB/Gyn and general surgery depending on whether there is bowel involvement
_____________________________________________________________________________________________
Self-managed Abortions
_____________________________________________________________________________________________
- Definition: abortion attempted outside the formal healthcare system
- Currently, most self-managed abortions use misoprostol and mifepristone and evidence from other countries show that using these medications outside of clinical supervision is effective and has a low rate of complications2.
- Other methods of self-managed abortions are not effective or safe:
- Ingesting toxins such as rue, St. John’s wort, black or blue cohosh
- Vaginal insertion of objects
- With the recent reversal of Roe vs Wade, some of the nearly 1 million people seeking abortion care annually will travel for medically supervised, legal care
- But 75% of patients seeking abortion are poor or low-income, and may seek dangerous methods to terminate a pregnancy if they lack access or rely on misinformation
_____________________________________________________________________________________________
Patients Requesting Abortion Reversal
_____________________________________________________________________________________________
- Some patients may present to the ED requesting a reversal of a medical abortion when they have ingested mifepristone but have yet to ingest mifoprostol
- A 2019 randomized controlled trial was halted prematurely because of safety concerns of hemorrhage when patients did not receive misoprostol
- The process of abortion reversal is an experimental treatment with possible risks and is not supported by ACOG
- Trials that have looked at fetal outcomes after mifepristone without misoprostol showed continued pregnancy rates of 8% to 46%.
- Patients who elect to attempt continued pregnancy should be advised to follow up closely with OBGyn and be given return precautions.
_______________________________________________________________________________
Key Concepts
______________________________________________________________________________
- Medically supervised medical and surgical abortions are extremely safe but rare complications including ectopic, hemorrhage, infection, uterine perforation and amniotic embolism can be deadly.
- Self-managed abortions are far less safe and are expected to rise with the reversal of Roe vs Wade.
- Pelvic exam, labs, ultrasound and rarely CT should identify complications.
- Consult OB Gyn for:
- Severe pain
- Abnormal Vitals
- Signs of infection
- Concerning ultrasound findings (e.g. retained products of conception, free fluid, adnexal mass)
- Persistent heavy bleeding
- Remind patients who are discharged that they need immediate contraception as they can become pregnant again in as little as 10 days.
_______________________________________________________________________________
References
_____________________________________________________________________________________________
- Orlowski, MH et al. Management of Postabortion Complications for the Emergency Medicine Clinician. Annals of Emergency Medicine. 2021; 77(2): 221-232.
- Harris, L and Grossman, D. Complications of Unsafe and Self-Managed Abortion. NEJM 2020; 382(11): 1029-1040.
