Contents
- Definition
- Epidemiology
- Pathogenesis
- Clinical Presentation
- Differential Diagnosis
- Approach to the patient with genital ulcers
- Approach to the patient with diffuse maculopapular rash
- Testing
- Whom To Test
- Treatment
- Disposition
- Key Concepts
- References
_____________________________________________________________________________________________
Definition
_____________________________________________________________________________________________
Syphilis: sexually transmitted infection caused by the bacterium Treponema pallidum, the specific bacteria is a spirochete.
Early syphilis: first year of the disease
- Primary syphilis: initial chancre
- Secondary syphilis: systemic illness that develops in 25-40% of folks with untreated primary syphilis.
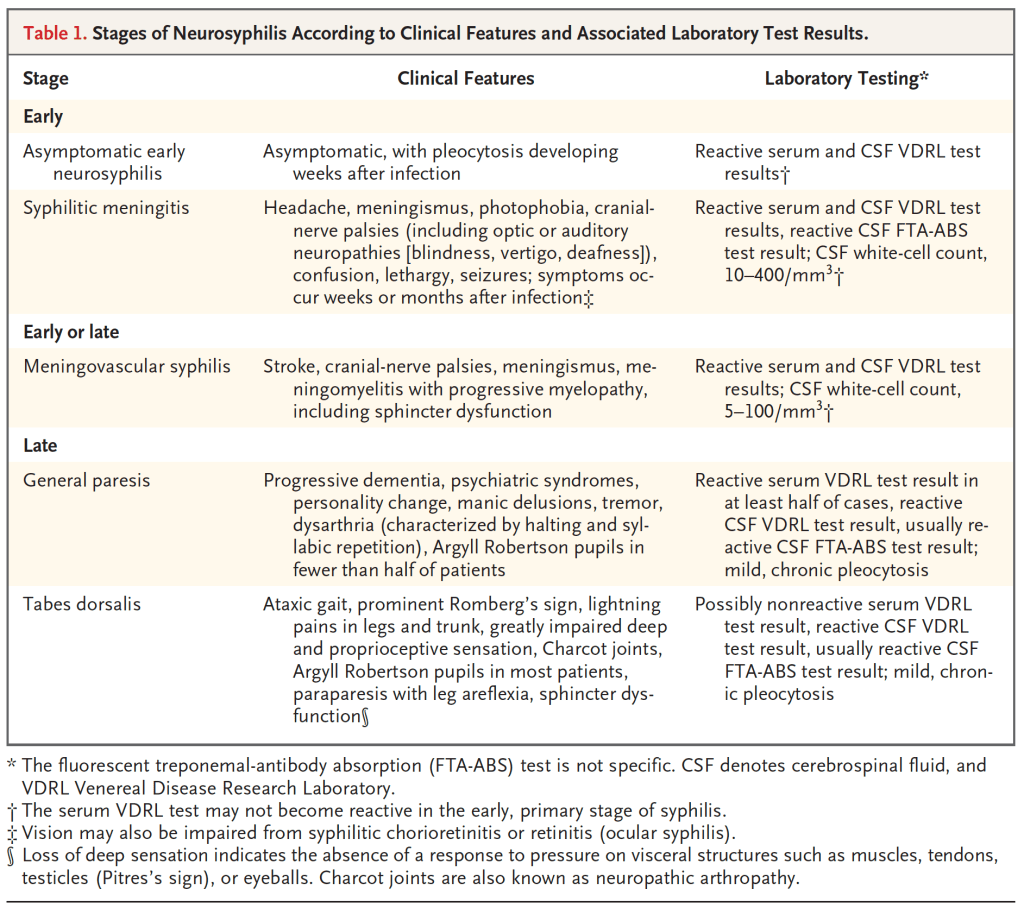
- Neurosyphilis: refers to infection of the CNS with T. Pallidum
Late Syphilis: syphilis beyond one year with or without symptoms
- Late latent syphilis- infected beyond one year but no clinical manifestations
- Tertiary syphilis- infected beyond one year with clinical manifestations
- Cardiovascular syphilis- vasculitis, especially of aorta (aortitis)
- Gummatous syphilis- granulomatous lesions in various organs, especially skin and bones
- General paresis and tabes dorsals (late neurosyphilis)
_____________________________________________________________________________________________
Epidemiology
_____________________________________________________________________________________________
- Case rates have been steadily climbing in the last 20 years and have surged in the last 10 years, increasing 400%.
- The rise is primarily attributed to men who have sex with men (MSM), 80% of syphilis cases are in men.
- Risk factors for syphilis include methamphetamine use and acquiring sexual partners on social media.
- There is a high rate (46%) of HIV coinfection among MSM with syphilis.
_____________________________________________________________________________________________
Pathogenesis
_____________________________________________________________________________________________
Transmission
- Occurs via direct contact with an infectious lesion during sex.
Early infection
- T. Pallidum gains access to subcutaneous tissues via microscopic abrasions.
- Establishes the initial ulcerative lesion, the chancre.
- The host immune response is paradoxical:
- Immune response resolves the initial lesion without treatment
- But allows the widespread dissemination of spirochetes at the same time, leading to secondary and tertiary syphilis.
Late infection
- Prolonged latent period suggests immune response may be involved in one of two ways.
- 1) Waning immunity may allow a small number of treponemes to multiply.
- 2) A partially immune hypersensitive host may react to the growing treponemes with a chronic inflammatory response (gummas consist of granulomas which are inflammatory response, aortic syphilis is a vasculitis of the aorta).
_____________________________________________________________________________________________
Clinical Presentation
_____________________________________________________________________________________________
Early Syphilis
- Primary Syphilis (chancre)-
- Begins as a papule, typically painless (30% are painful), appearing at the site of inoculation.
- Evolves into a 1-2cm painless ulcer with a raised margin
- May appear on parts of the body other than the genitals, for example can be inside/outside the mouth, anus, vagina.
- Heals spontaneously in 3-6 weeks.

Secondary Syphilis
- Within weeks to months after the initial chancre develops, 25% of untreated individuals will develop a systemic illness comprised of:
- Generalized symptoms
- Constitutional symptoms: fever, headache, malaise, anorexia, sore throat, myalgias, and weight loss. This probably reflects the immunologic response to widespread dissemination of T. Pallidum.
- Adenopathy: lymph node enlargement in cervical, axillary, inguinal, femoral and epitrochlear (elbow- particularly suggestive of syphilis) regions.
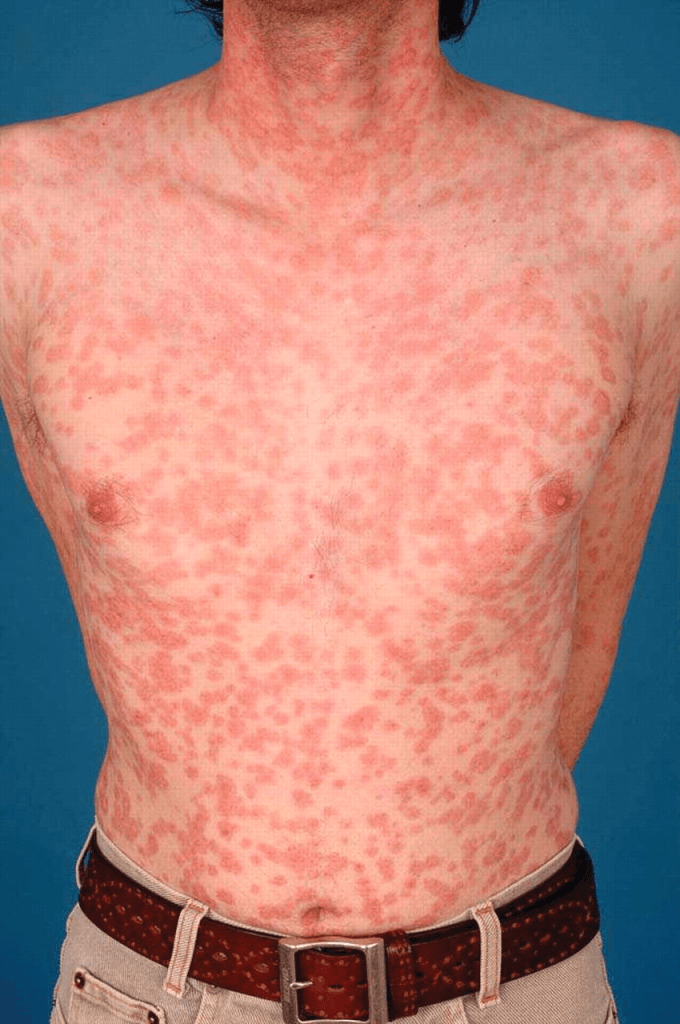
- Dermatologic findings
- Rash- can take almost any form
- Classically diffuse, symmetric macular or papular eruption involving the entire trunk and extremities including the palms and soles.
- On occasion the rash may be pruritic.
- Individual lesions are discrete copper, red or reddish brown, often scaly.
- Pustular syphilis
- Mucous patches: white erosions on the tongue, lips or oral mucosa
- Lues maligna (malignant syphilis)- a severe ulcerative form of secondary syphilis mainly in patients with HIV with a compromised immune system, only form of secondary syphilis that is nonresolving
- Alopecia, Gastrointestinal, Hepatitis, Musculoskeletal, Renal
- Rash- can take almost any form
- Generalized symptoms
Neurosyphilis
- Infection of the CNS by T. Pallidum
- Can occur at any time after initial infection
- Early neurosyphilis usually involves the CSF, meningitis and vasculature
- Late in disease the most common forms involve the brain and spinal cord
- Lumbar puncture?
- Since secondary syphilis has constitutional symptoms including headache, the ED provider may need more than moderate headache to proceed with LP for the patient who presents with a secondary syphilis rash.
- If the headache is severe, or there are other concerning features (eg, stiff neck, photophobia, AMS, hearing loss), LP is warranted.
- CDC recommends LP for:
- Neurologic or ophthalmic signs or symptoms in any stage of syphilis.
- Evidence of active tertiary syphilis affecting other parts of the body.
- Treatment failure (including failure of serum nontreponemal tests to fall appropriately) in any stage of syphilis.
Ocular Syphilis
- Can involve any eye structure but posterior uveitis is most common and presents with decreased visual acuity
Otosyphilis
- Hearing loss and tinnitus are considered part of neurosyphilis.
Late neurosyphilis
- General paresis- progressive dementing illness
- Tabes dorsalis (locomotor ataxia)- sensory ataxia and lancinating pain
_____________________________________________________________________________________________
Differential Diagnosis
_____________________________________________________________________________________________
Genital Ulcer
- Infectious causes
- HSV 1/2- multiple, shallow, tender, painful ulcers that may be vesicular
- Treponema Pallidum- usually painless
- Chancroid (Haemophilus ducreyi)- Africa, Asia, Latin America, Caribbean
- Lymphogranuloma venereum (LGV)- Africa, Caribbean, India, parts of Southeast Asia, localized outbreaks in North America and Europe among MSM.
- Granuloma inguinale (donovanosis)- India, South Africa, South America.
- Monkeypox- can present with genital lesions
- Noninfectious Causes
- Behcet’s Syndrome- genital lesions in 75% of patients with Behcet’s
- Drug Eruption
- Crohn’s
- Neoplasm
- Infectious causes
- HIV: fever, lymphadenopathy, rash fatigue, diarrhea, mucosal sores (will catch this with baseline testing)
- Toxic shock syndrome- sick! high fever (>/=39), hypotension, desquamating rash, multiple organ systems
- Measles- blanching erythematous brick red maculopapular rash beginning in head neck
- Mumps
- Chicken Pox
- CMV
- Coxsackie Virus
- Rubella
- Lyme disease
- Scarlet Fever- red macula’s on hard and soft palate (Forchheimer’s spots)
- Rocky mountain spotted fever- maculopapular rash, petechial rash
- Kawasaki disease- can occur in adults, peeling skin hands, feet, conjunctivitis
- Monkeypox
- Mononucleosis
- Noninfectious causes
- Erythema Multiforme- target lesions
- Stevens-Johnson- fever, sore throat, maculopapular rash that forms
- Drug eruption/Drug fever
- Pityriasis rosea
_____________________________________________________________________________________________
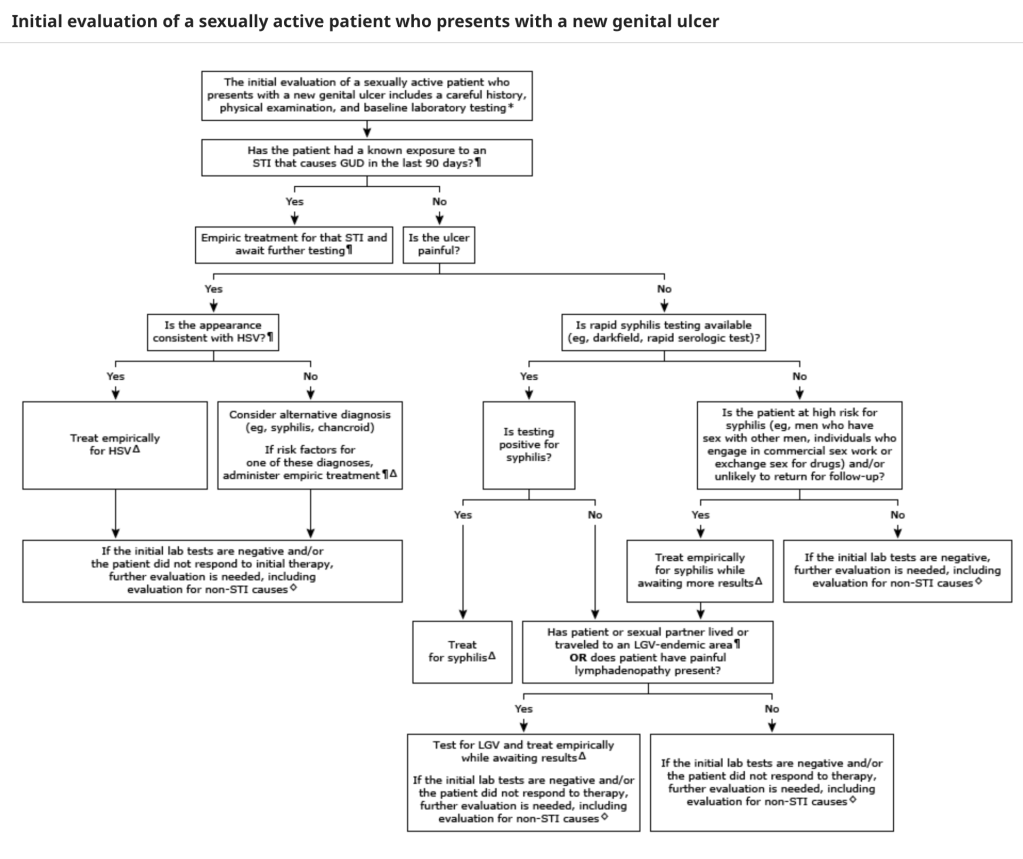
Approach to the patient with genital ulcers
_____________________________________________________________________________________________
- History: travel, sexual history, exposure, new drug, h/o Crohn’s or Behcet’s, dysuria (suggests possible concurrent GC/Chlamydia), constitutional sxs seen with HSV or secondary syphilis.
- Exam
- Baseline Testing (see below)
- Empiric treatment (see algorithm)
_____________________________________________________________________________________________
Approach to the patient with diffuse maculopapular rash
_____________________________________________________________________________________________
- History- drug history, travel history (northeast Lyme, Southeast/Atlantic- RMSF), sexual history, exposures (Monkeypox), immunization history (MMR immunized)
- Exam
- Palms and soles- T. Pallidum, Coxasckie, RMSF (especially the wrist), Janeway lesions, Kawasaki disease, Measles, Toxic Shock Syndrome, Meningococcemia
- Vessicles/Bullae/Pustules– T. Pallidum, Staph, RMSF, Neisseria, Coxsackie, HSV, Varicella, Monkeypox
- Labs
- CMC, BMP, LFTs, UA to look for organ injury
- Blood cultures if febrile to look for endocarditis
- Other serologies: HIV, Hepatitis, Mono, Syphilis, Chlamydia, Gonorrhea
- Send vesicle fluid for HSV and possibly for Monkeypox PCR if suspicious
- Empiric treatment for:
- Palms and soles
- Recent primary syphilis or exposure to syphilis
- Risk factors: MSM, sex worker, methamphetamines
_____________________________________________________________________________________________
Testing
_____________________________________________________________________________________________
Baseline Testing
- Patients who present with genitals ulcers or diffuse rash suggestive of secondary syphilis should get baseline testing for STIs:
- HSV: swab lesion and send for HSV 1/2 PCR (higher sensitivity than cx), if no PCR, send cx, vesicular fluid preferred.
- HIV, Gonorrhea, Chlamydia, Hepatitis
- Monkeypox (if vesicular lesions or history of exposure or patient is MSM)
Syphilis Testing Options
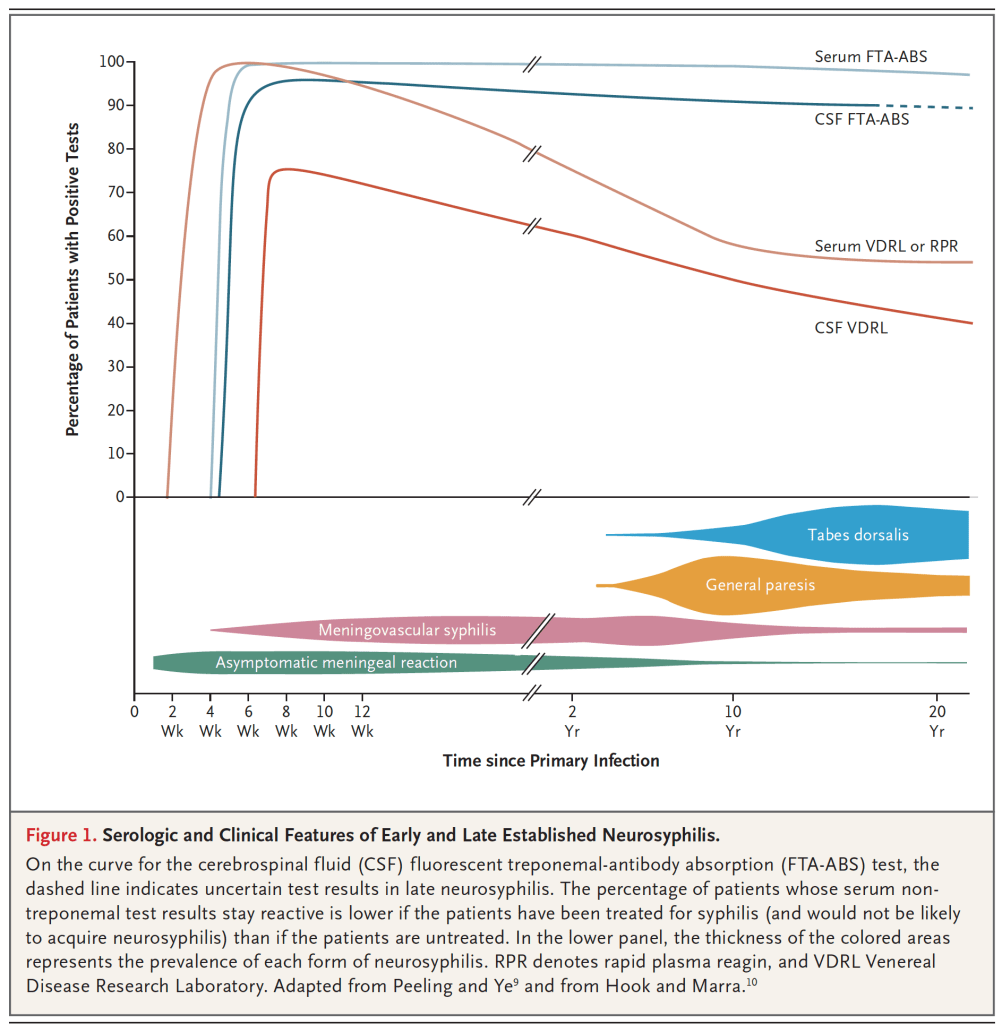
- Treponemal test
- Detect antibodies produced by the body only after infection with T. Pallidum
- More sensitive than nontreponemal tests early in disease
- Patients may still test positive after completing treatment
- Now the preferred initial screening test
- FTA-ABS. Hospital lab may do this as a send out.
- Nontreponemal test
- Detects antibodies that are not specific to T. Pallidum
- Although these antibodies are usually produced when a person has syphilis they can be produced in response to other conditions.
- Patients normally test negative with these tests after successful syphilis treatment
- Positive nontreponemal tests are reported as a titer of antibody (eg, 1:32, which represents the detection of antibody in serum diluted 32-fold).
- RPR- blood but not CSF. Hospital labs may run in batches 1x/day.
- VDRL- seen in blood and CSF, positive 1-2 weeks after initial infection
- Detects antibodies that are not specific to T. Pallidum
- Rapid Serologic Tests
- Most are treponemal specific tests
- Although they have been found to have good sensitivity/specificity, most have not been formally assessed by regulatory agencies yet.
- Darkfield microscopy and direct fluorescent antibody are not routinely used because they require special equipment to perform.
Approach To Testing
- Asymptomatic Patients
- Either FTA-ABS or RPR alone will rule out disease (rare exception in patient with recent infection <4 weeks)
- Symptomatic Patients
- Serologic testing includes the use of both nontreponemal and treponemal tests to improve accuracy, either can be used as the initial test.
- FTA-ABS better initial test, if not planning to treat empirically, because more sensitive but needs a follow-up RPR to confirm it is not a false positive result.
- If you plan to treat empirically (usually the case in the ED), UPTODATE recommends ordering a pretreatment nontreponemal titer (RPR or VDRL) to be able to trend response to treatment so just do the nontreponemal alone if doing empiric treatment.
- Testing for neurosyphilis
- CSF-VDRL is highly specific but only 70% sensitive, if CSF-VDRL is negative and neurosyphilis is suspected, a CSF FTA-ABS test can be ordered.
Interpretation of Serologic Testing
A. Positive Treponemal/Positive Nontreponemal
- Supports a diagnosis of syphilis
- Patients without a history of syphilis
- Symptomatic- stage as primary, secondary of tertiary and treat accordingly
- Asymptomatic- patient has either early latent or late latent syphilis
- Patients with a history of syphilis
- Treponemal tests usually remain positive for life
- Nontreponemal titers usually decline over time
- If nontreponemal is positive, compare to prior titers to determine if:
- New infection- >/=4 fold increase in titer from prior (eg, 1:4 increases to 1:16)
- Evolving response to treatment (declining titer: eg, 1:16 decreases to 1:8)
- Treatment failure
- Serofast state- complicated, refer to public health or ID
B. Positive nontreponemal/negative treponemal
- Generally considered to be a false positive result
C. Positive Treponemal/Negative Nontreponemal
- Seen in patients with successfully treated syphilis
- If a chancre or rash suggests early rash, a nontreponemal test should be repeated to assess for seroconversion.
_____________________________________________________________________________________________
Whom To Test
_____________________________________________________________________________________________
- Painless genital ulcer (primary syphilis)
- Diffuse, symmetric macular or papular eruption involving the entire trunk and extremities (secondary syphilis)
- General paresis or tabes dorsalis (tertiary syphilis)
- Any sexually active person with an undiagnosed genital ulcer or a rash that involves the palms and soles.
- Patients who present with signs and symptoms that are less specific for syphilis (eg, cranial nerve dysfunction, chronic headache, aortic insufficiency, meningitis, other signs of meningovascular disease, including CVA) particularly if no alternative etiology is identified.
_____________________________________________________________________________________________
Treatment
_____________________________________________________________________________________________
Empiric Treatment for primary and secondary syphilis
- Suspected chancre
- Known exposure (condomless oral, anal or vaginal sex with
- Suspected secondary syphilis rash, especially if follow-up poor.
Early Syphilis (primary or secondary syphilis)
- Preferred: PCN G Benzathine 2.4 million units IM once
- Alternatives (choose one):
- Doxycycline 100mg PO BID for 14 days
- Ceftriaxone 1g daily IM or IV for 10-14 days
Late syphilis (tertiary syphilis or late latent syphilis)
- Preferred: PCN G Benzathine 2.4 million units IM once weekly for 3 weeks
- Alternatives (choose one):
- Doxycycline 100mg PO BID for 4 weeks
- Ceftriaxone 2g daily IM or IV for 10-14 days
Neurosyphilis
- Preferred: PCN G 3-4 million units IV Q4hrs
- Alternative (choose one):
- Ceftriaxone 2g IV QD for 10-14 days
Jarisch-Herxheimer Reaction
- Acute, self-limited febrile reaction that usually occurs within the first 24 hours after the patient receives therapy for any spirochete infection, including syphilis
- Occurs in 10-35% of cases, so warn patients that this may occur
- Most common after treatment of primary syphilis
- The reaction often resolves within 12-24 hours and can be treated with NSAIDS or Acetaminophen
- Uncommon manifestations include meningitis, respiratory distress, stroke, seizures, AMS, renal and/or hepatic dysfunction
_____________________________________________________________________________________________
Disposition
_____________________________________________________________________________________________
Hospitalization
- Hospitalization is recommended for:
- Neurosyphilis
- Patients with PCN allergy who will not reliably take Doxycycline
- Patients with penicillin allergy who require desensitization prior to penicillin therapy:
- Pregnant women with syphilis or congenital syphilis (PCN is the only accepted therapy).
Outpatient Teachable Moment
- Most patients can be managed as an outpatient
- The diagnosis of syphilis or any STI provides the physician with a teachable moment:
- Explain the nature of infection and how it is transmitted
- Importance of using condoms and other safe sex practices
- Importance of contacting any sexual partners to get tested/treated
- Importance of compliance with therapy to avoid complications
- Importance of follow-up with a PCP or public health department for follow-up titers, to ensure therapy was effective.
- Warning of potential Jarish Herxheimer reaction
______________________________________________________________________________________________
Key Concepts
_____________________________________________________________________________________________
- Syphilis typically presents to the ED with either a genital ulcer or a diffuse maculopapular rash.
- See Approach to Genital Ulcers and Approach to Diffuse Rash
- Testing is usually a sequence of both a nontreponemal (RPR or VDRL) and a treponemal (eg, FTA-ABS) test, start with nontreponemal in ED if you plan to treat empirically and lab may have a reflex algorithm to send out the FTA-ABS if RPR is positive.
- Empirically treat if known exposure, suspected chancre or suspected secondary rash.
- Send baseline labs for other STI: HIV, Chlamydia, Gonorrhea, Hepatitis
- Send nontreponemal (RPR or VDRL) if treating so a pretreatment titer is done.
- Take advantage of the teachable moment: safe sex, compliance with treatment, send in partners for test/treat, beware of Jarish Herxheimer, follow-up for titers.
______________________________________________________________________________________________
References
_____________________________________________________________________________________________
Rosen’s Emergency Medicine: Concepts and Clinical Practice. Tenth Edition. 2023. Chapter 84- Sexually Transmitted Infections. Author: Jeffry McKinzie.
UPTODATE: Syphilis. Authors: Hicks and Clement. July 2022.
Ropper, A. Neurosyphilis. NEJM 381:14, Oct 3, 2019.
Workowski KA, Bolan GA, Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines, 2015. MMWR Recomm Rep. 2015;64(RR-03):1.

{kind=link}
{kind=link}