American J of Emerg Med
Electrocardiographic Manifestations of COVID-19
- COVID-19 is a potentially critical illness associated with a variety of ECG abnormalities, with up to 90%of critically ill patients demonstrating at least one abnormality.
- The ECG abnormalities in COVID-19 may be due to cytokine storm, hypoxic injury, electrolyte abnormalities, plaque rupture, coronary spasm, microthrombi, or direct endothelial or myocardial injury.
- While sinus tachycardia is the most common abnormality, others include supraventricular tachycardias such as atrial fibrillation or flutter, ventricular arrhythmias such as ventricular tachycardia or fibrillation, various bradycardias, interval and axis changes, and ST segment and T wave changes.
- Several ECG presentations are associated with poor outcome, including atrial fibrillation, QT interval prolonga-tion, ST segment and T wave changes, and ventricular tachycardia/fibrillation.
Annals of Emergency Medicine
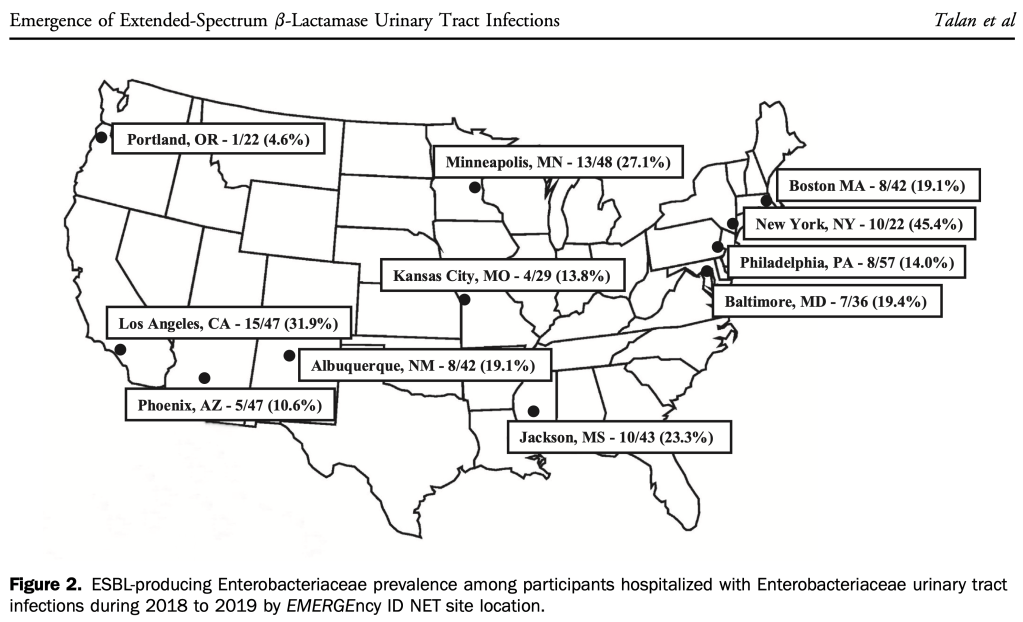
- Growing percentage of hospitalized patients with UTI have resistance to ceftriaxone (17% overall during the study period of 2018-2019) but some areas of the country are much higher.
- Authors cite a 2009 study by Kumar that showed a 5 fold reduction in survival for septic shock patients who received initial empiric antibiotics that lacked in-vitro activity against the offending pathogen.
- 24% resistance to Ceftriaxone among Enterobact. isolates, 3% resistance to Pip-Taz.
- Among ESBL-confirmed isolates, resistance to Pip-Taz was 18%.
- Resistance>10% is the recommended trigger to broaden coverage.
- Authors recommend a carbapenem or amikacin for hospitalized UTI and acknowledge there is no PO option for outpatients.
- Uptodate recommends a carbapenem for septic shock patients with suspected UTI.
- Per Johnson, Acute Pyelonephritis in Adults (NEJM 2018), choose an antibiotic of a different class for initial empirical treatment of pyelonephritis when the local resistance rate to the antibiotic being considered exceeds 10%, with a lower threshold for critically ill patients.
- Bottom-line: know your hospital’s antibiogram, upgrade from Ceftriaxome if resistance is >10%.
Improved Testing and Design of Intubation Boxes During the COVID-19 Pandemic
- Intubation boxes don’t reduce aerosol but adding a vacuum and active air filtration did.
Prevalence of SARS-Cov-2 Antibodies in Emergency Medicine Providers
- Although studies from NYC early in the pandemic showed a high prevalence of prior Covid infection (31.2% and 46%) among ED providers, this study from San Francisco showed a low seroprevalence of antibodies (1%).
- 2% of bacterial meningitis has normal CSF fluid cell count!
- 25% fatality rate among normocellular meningitis cases.
- Authors suggest empiric treatment in cases with a high suspicion despite normal CSF until cultures come back.
- The Pneumonia Severity Index (PSI) and CURB-65 decision aids can support clinical judgement by identifying patients at low risk of mortality who may be appropriate for outpatient treatment. Although both decision aids are acceptable, the PSI is supported by a larger body of evidence and is preferred by other society guidelines (ATS/IDSA 2019 guidelines).
- Given the lack of evidence, the decision to administer a single dose of parenteral antibiotics prior to oral therapy should be guided by patient risk profile and preferences (Consensus recommendation).
BMJ
Easily Missed? Cauda Equina Syndrome
- Red flags for caudal equina in patients with sciatica
- Onset of bilateral numbness or weakness in the legs
- Onset of any sense of numbness or pins and needles around the anus (a “numb bum”) or genitals
- Any alteration in the sensation of a full bladder, desire to pass urine, or awareness of passing urine
Emerg Med J
Identification of very low risk acute chest pain patients without troponin testing
- Providers completed HEAR assessments on 4979 patients and HEAR scores<1 occurred in 9.0% (447/4979) of patients. Among these patients, MACE at 30 days occurred in 0.9% (4/447; 95% CI 0.2% to 2.3%) with two deaths, two MIs and 0 revascularisations. The sensitivity and negative predictive value for MACE in the HEAR <1 was 97.8% (95%CI 94.5% to 99.4%) and 99.1% (95% CI 97.7% to 99.8%), respectively, and were not improved by troponin testing. Troponin testing in patients with HEAR <1 correctly reclassifi ed two patients diagnosed with MACE, and was elevated among seven patients without MACE yielding an NRI of 0.9% (95%CI −0.7 to 2.4%).
- Conclusion These data suggest that patients with HEAR scores of 0 and 1 represent a very low risk group that may not require troponin testing to achieve a missed MACE rate <1%.
EMRAP
- Syncope- Amal Mattu
- Canadian Syncope Risk Score recommended!
- Validated in JAMA March 2020 study: Multicenter Emergency Department Validation of the Canadian Syncope Risk Score
- Available on MDCALC
- Per Mattu:
- “Patients with very low to low risk (-3 to 0 points) can be discharged home with a low event rate
- Patients with intermediate risk (1-3 points) have an 8% risk of bad outcome at 30 days (0.1% risk of death). Shared decision making is appropriate here.
- Patients with higher risk (> 4 points) probably should be admitted in consideration of their high rate of bad outcomes, despite the low diagnostic yield.”
- Cranial Burr Hole (emergent epidural or subdural evacuation)- Jess Mason and David Beffa
- Free 5 minute “how to do it” video: https://www.emrap.org/episode/cranialburrhole/cranialburrhole
- “Steps of procedure (to be done on the side of the blown pupil) Knowing the anatomy from the CT head will be helpful. You can measure the thickness of the skull table so you know approximately how deep you need to go.
- Prepare the site using sterile technique.
- If no CT is available and the procedure is done blind, the entry site is 2 cm superior and 2 cm anterior to the tragus on the ipsilateral side of the blown pupil
- Have an assistant hold the patient’s head hard and steady during the procedure.
- Make a 3-5 cm vertical skin incision down to bone.
- Insert self-retaining scalp retractor to expose periosteum.
- Expose the skull and elevate the periosteum using the periosteal elevator.
- Trephination technique varies by device. You may feel a change from smooth to rough as you move from outer to inner skull table.
- An epidural hematoma will start to drain when you get through the inner table. If a subdural hematoma is present, an additional step is needed which involves a 3-sided incision to form a flap in the dura mater.
- Place a sterile dressing.”
- Eye vs Brain– Evie Marcolini, MD and Anand Swaminathan, MD
- Diplopia easy to distinguish, monocular diplopia most likely ocular pathology, whereas binocular diplopia is usually CNS .
- Cranial Nerve Palsy: 3, 4, 6 (think SAH when CN 3 palsy, abduction only -no adduction, supraduction or infraduction, with acute HA)
- Internuclear Ophthalmoplegia
- Hard to distinguish between ocular and CNS pathology with painless, non-red, non-post-op, atraumatic monocular vision loss!
- Uptodate has a nice algorithm for monocular vision loss.
- The challenge is the ddx for painless, non-red, non-post-op, atraumatic monocular vision loss includes both ocular and CNS etiology.
- Ocular: lens, vitreous hemorrhage, posterior uveitis, acute maculopathy, retinal detachment (peripheral or central loss), retinal vein occlusion, ischemic optic neuropathy (eg temporal arteritis).
- CNS- retinal or ophthalmic artery occlusion
- If after exam, history and ultrasound you’re not sure, patient needs transfer to tertiary center with both neurology and ophthalmology.
- Diplopia easy to distinguish, monocular diplopia most likely ocular pathology, whereas binocular diplopia is usually CNS .
JACEP Open
Not all HEART scores are created equal: identifying “low-risk” patients at higher risk
- ED patients being evaluated for acute coronary syndrome shows that HEART scores of 0–5 are generally at low risk for death or acute myocardial infarction within 30 days, but points obtained from different components of the score are associated with different risk elevations.
- Specifically, any points obtained due to elevated troponin values (even in the intermediate range, cor-responding to troponin = 1 or 2 points) as well as ST deviations (cor-responding to ECG = 2 points) were predictive of higher risk than an equal number of points obtained from the other components.
- Although the HEART score still reliably identifies low-risk ED patients, further research on refinements to the score (eg, allocating additional points to the troponin component and correspondingly recalibrating the cut-off score to better match a 1% acceptable risk threshold for further testing) may better assess the risks facing patients with suspected acute coronary syndrome, allow for better risk stratification of patients with chest pain, and merits further study.
NEJM
Bupropion and Naltrexone in Methamphetamine Use Disorder
