Academic Emergency Medicine
No Feb issue as of March 2, 2022, 2:20pm
American Journal of Emergency Medicine
Dispelling myths and misconceptions about the treatment of acute hyperkalemia
Annals of Emergency Medicine
Moving Upstream: A Social Emergency Medicine Approach to Opioid Use Disorder
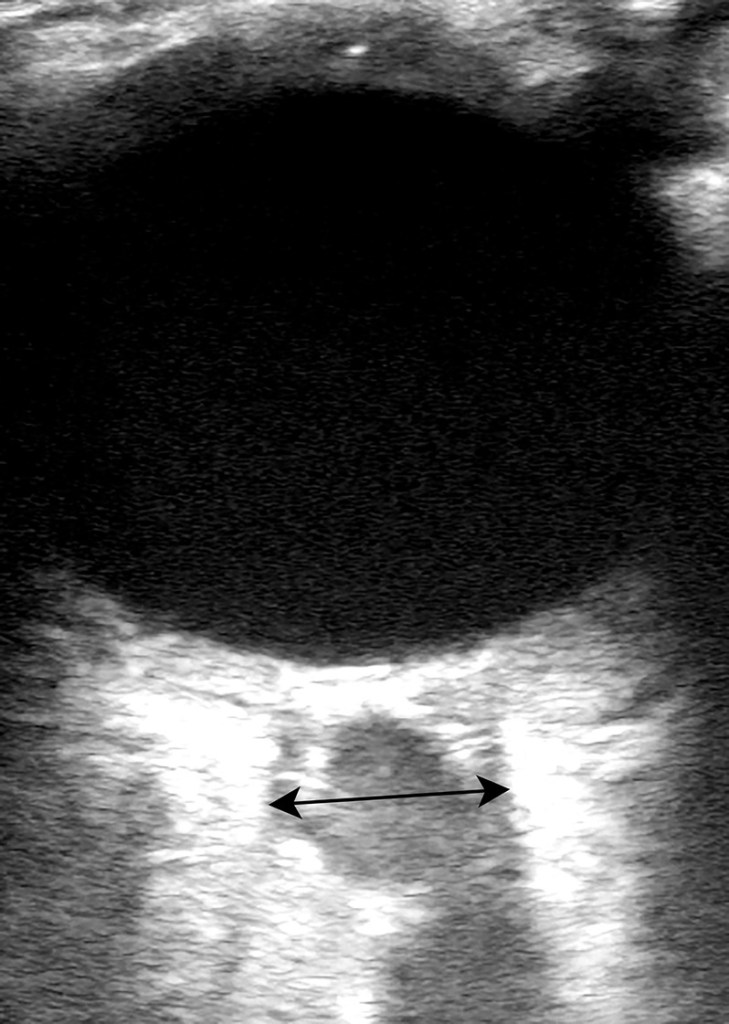
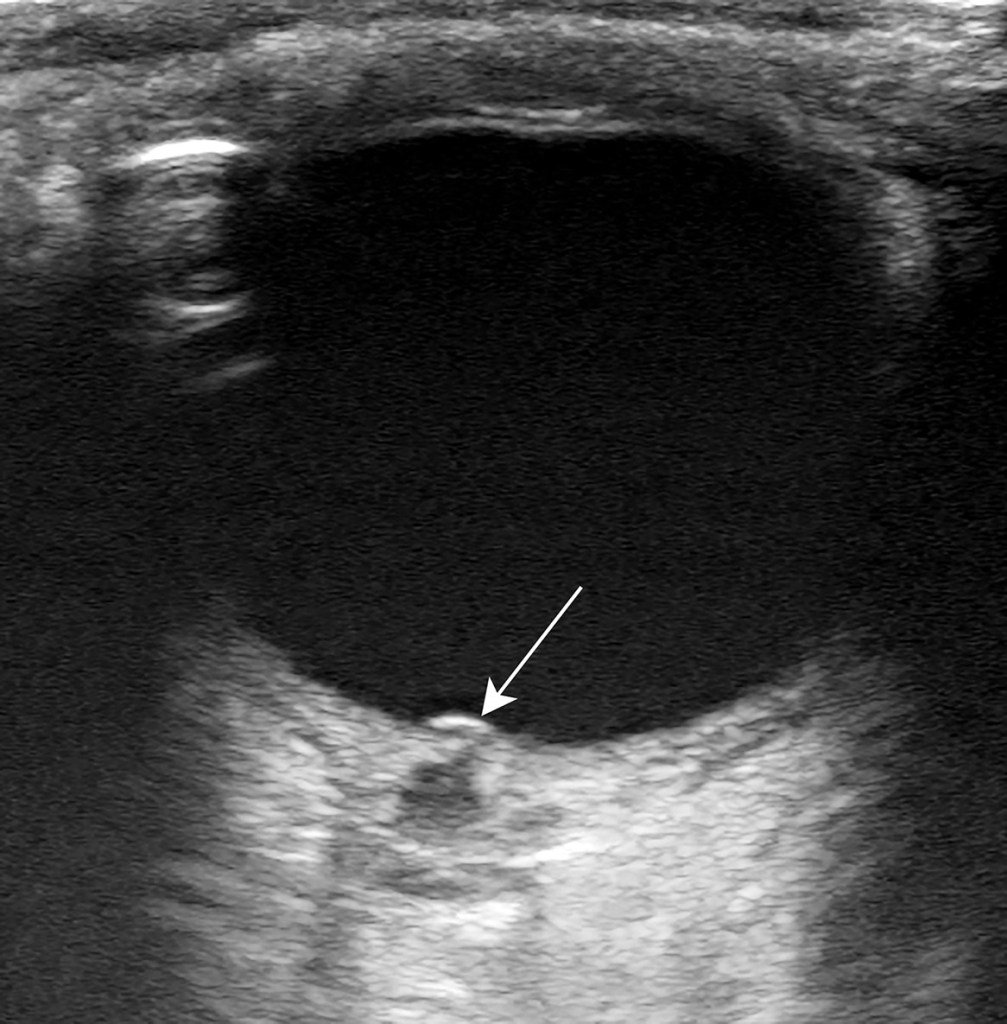
Man With Eye Pain and Decreased Vision
- A healthy 39-year-old man presented to the emergency department with 2 days of nontraumatic severe left eye pain and progressive visual loss to the point of blindness. Upon physical examination, the patient reported only flashes of light in the left eye, with sluggish pupillary response and painful extraocular movements. The result of slit lamp examination was unremarkable, and ocular pressures were normal. The result of right eye examination was unremarkable. An emergency physician conducted point-of-care ocular ultrasound, demonstrating evidence of papilledema and optic nerve inflammation
BMJ
- DVT was considered excluded without further testing by Wells low clinical pretest probability and D-dimer <1000 ng/mL or Wells moderate clinical pretest probability and D-dimer <500 ng/mL. All other patients had proximal ultrasound imaging. Repeat proximal ultrasonography was restricted to patients with initially negative ultrasonography, low or moderate clinical pretest probability, and D-dimer >3000 ng/mL or high clinical pretest probability and D-dimer >1500 ng/mL.
- Of the 1275 patients with no proximal DVT on scheduled testing who did not receive anticoagulant treatment, eight (0.6%, 95% confidence interval 0.3% to 1.2%) were found to have venous thromboembolism during follow-up. Compared with a traditional DVT testing strategy, this diagnostic approach reduced the need for ultrasonography from a mean of 1.36 scans/patient to 0.72 scans/patient (difference −0.64, 95% confidence interval −0.68 to −0.60), corresponding to a relative reduction of 47%.
Circulation
None
CJEM
EMCRIT
None
Emergency Medicine Journal
Teach-back of discharge instructions in the emergency department: a pre–post pilot evaluation
EMRAP
Devil’s Advocate- Traumatic Arthrotomy
- Konda SR et al. Computed tomography scan to detect traumatic arthrotomies and identify periarticular wounds not requiring surgical intervention: an improvement over the saline load test. J Orthop Trauma 2013; 27: 498-504.
- As good as saline load test
Drugs in Atrial Fibrillation with RVR
- Mag 2-4g IV
- Dilt 10 as good as .25mg/kg
- If BP low, give 2g CaGluconate
JAMA
- The requirement for tracheal intubation or mortality within 30 days was significantly lower with CPAP (36.3%; 137 of 377 participants) vs conventional oxygen therapy (44.4%; 158 of 356 participants) (absolute difference, −8% [95% CI, −15% to −1%], P = .03), but was not significantly different with HFNO (44.3%; 184 of 415 participants) vs conventional oxygen therapy (45.1%; 166 of 368 participants) (absolute difference, −1% [95% CI, −8% to 6%], P = .83).
- Proning not studied but probably more important than oxygen delivery system
Defining Optimal Respiratory Support for Patients With COVID-19
Journal of Emergency Medicine
None
Lancet
None
NEJM
Stabilizing Health Care’s Share of the GDP
Inherited Patients Taking Opioids for Chronic Pain — Considerations for Primary Care
PEDIATRICS
None
REBELEM
Andexanet Alfa Vs. Four-Factor PCC: Is Andexanet Alfa Worth The Hype?
- This limited study found no statistically significant difference in stability of oral FXi related ICH after the administration of AA or 4F-PCC. However, the inherent potential bias and small participant numbers limit generalizability and therefore larger prospective studies are needed. 4F-PCC is cheaper and more widely available than AA ($5670/patient, compared to $22,120-$49,500/patient);
Resuscitation
- Improved chance of ROSC but not statistically significant improved hospital discharge.
