Academic Emergency Medicine
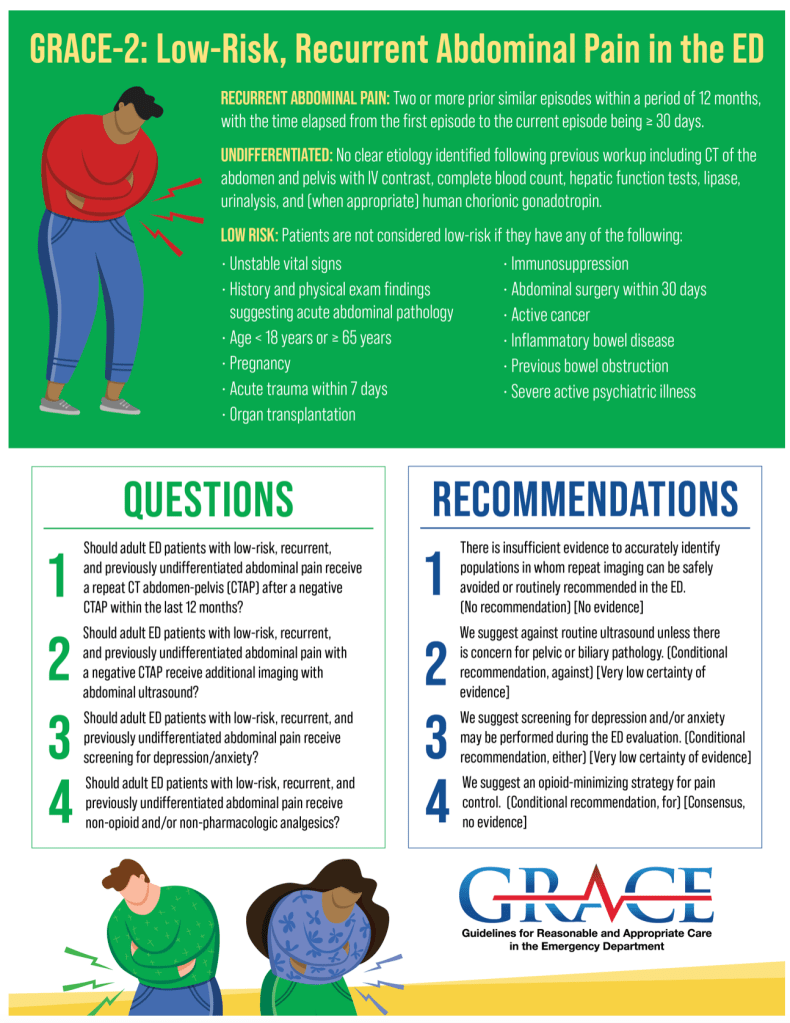
- GRACE-2 is the follow-up to the super helpful GRACE-1 released last year for recurrent chest pain.
- Unfortunately, GRACE-2 was not able to come up with any powerful recommendations other than the obvious: avoid opiates.
American Journal of Emergency Medicine
None
Annals of Emergency Medicine
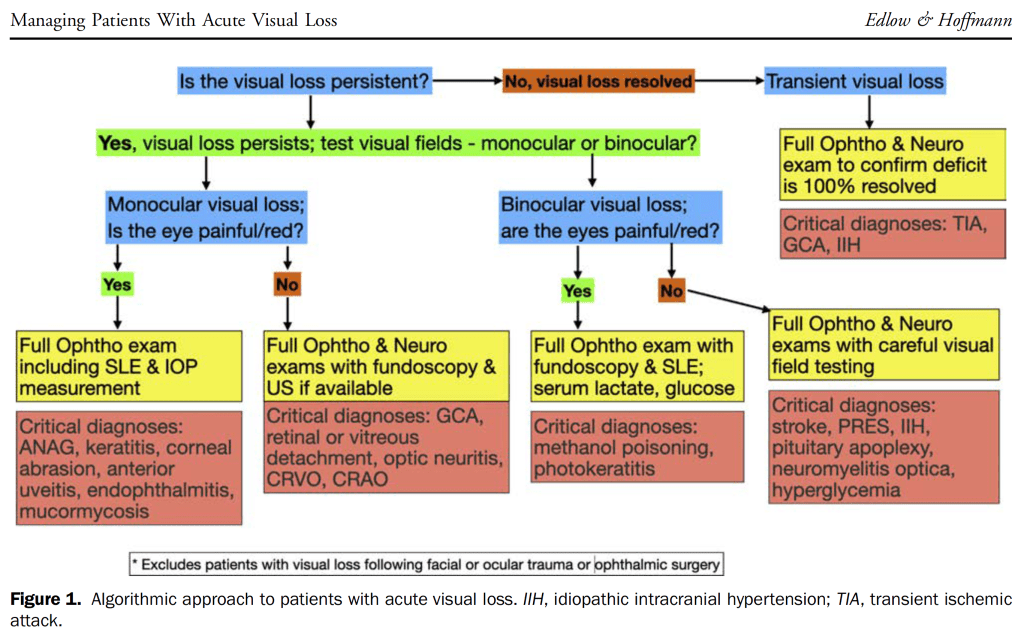
Managing Patients With Acute Visual Loss
BMJ
Monkeypox: What do we know about the outbreaks in Europe and North America?
- CDC review for clinicians
- Incubation: 7-14 days
- Transmission
- Transmission between people mostly occurs through large respiratory droplets, normally meaning prolonged contact face to face. But the virus can also spread through bodily fluids. The latest cases have mainly been among men who have sex with men.
- Symptoms
- Fever, headache, muscle aches, backache, swollen lymph nodes, chills, and exhaustion. Typically a rash will develop, which often starts on the face but can then spread to other areas such as the genitals.
- Shortly after the prodrome, a rash appears. Lesions typically begin to develop simultaneously and evolve together on any given part of the body. The evolution of lesions progresses through four stages—macular, papular, vesicular, to pustular—before scabbing over and resolving.
- Testing
- Contact local public health department.
- LA County 213-240-7941 8:30a-5p, after hours 213-974-1234
- Or contact CDC 1-770-488-7100
- Contact local public health department.
- Treatment
- None
- Prognosis
- Most cases mild but case fatality rate 3.6% among African studies
Circulation (need to review May 31)
- Guideline-directed medical therapy (GDMT) for heart failure (HF) with reduced ejection fraction (HFrEF) now includes 4 medication classes that include sodium-glucose cotransporter-2 inhibitors (SGLT2i): canagliflozin, dapagliflozin, and empagliflozin.
- SGLT2i have a Class of Recommendation 2a in heart failure with mildly reduced ejection fraction (HFmrEF). Weaker recommendations (Class of Recommendation 2b) are made for ARNi, ACEi, ARB, MRA, and beta blockers in this population.
- New recommendations for HFpEF are made for SGLT2i (Class of Recommendation 2a), MRAs (Class of Recommendation 2b), and ARNi (Class of Recommendation 2b). Several prior recommendations have been renewed including treatment of hypertension (Class of Recommendation 1), treatment of atrial fibrillation (Class of Recommendation 2a), use of ARBs (Class of Recommendation 2b), and avoidance of routine use of nitrates or phosphodiesterase-5 inhibitors (Class of Recommendation 3: No Benefit).
CJEM
No May issue, only abstracts supplement
EMCRIT
Cerebral venous thrombosis (CVT)
- CT without contrast is 70% sensitive for CVT which is pretty good considering this is a rare condition and according to J Edlow’s study, 94% have focal neurologic abnormalities.
- Cerebral Venous Thrombosis: Pearls and Pitfalls– EMDOCS
- Indications for CT Venogram (same thing as a CT arteriogram, except that there is more delay between the time that the contrast is administered, and the time that the sequences are acquired):
- Headache: in a pregnant female patient, in a young female on OCPs, or one that is atypical and persistent
- Stroke with no typical risk factors or in the setting of seizure
- Intracranial hypertension with no explanation
- Multiple hemorrhagic infarcts, or hemorrhagic infarcts not in a specific arterial distribution
- Objective neurologic symptoms in a patient with risk factors for CVT
- Indications for CT Venogram (same thing as a CT arteriogram, except that there is more delay between the time that the contrast is administered, and the time that the sequences are acquired):
Neurologic emergencies in pregnancy
Emergency Medicine Journal
EMRAP
- Bipap IPAP 10-15, EPAP 2
- If tidal volumes poor with Bipap they likely will not improve with noninvasive.
- Inaba recommends CTA of the neck for all near-hangings.
Cardiology Corner: JACC Chest Pain Update
- Best piece of the month by Mattu
- Recommends the term “low risk chest pain” rather than atypical chest pain or non cardiac chest pain.
- Agrees with a warranty period (very low risk of ACS) of 2 years for normal angio or clean CCTA, but disagrees that a stress test offers a 1 year warranty period.
- Agrees with JACC recommendation that intermediate or high risk patients can get further testing:
- If<65yo or less obstructive disease is suspected, prefer CCTA.
- If>65yo or more obstructive disease is suspected, prefer stress testing, if either is equivocal, then repeat with the other test.
- Patients with<1% risk of MACE do not require an urgent workup and can be discharged.
Medicolegal Briefs: Myocarditis
- Good warning that myocarditis does carry risk of sudden death from arrhythmia.
- Not sure I would have done an EKG and cardiac workup on a patient with cough, fever and pleuritic CP?
First10EM
Long-term cardiovascular outcomes of COVID-19
Intensive Care Medicine
Challenging management dogma where evidence is non-existent, weak or outdated
- loop diuretic treatment for acute heart failure
- the effectiveness of heparin thromboprophylaxis
- the rate of sodium correction for hyponatraemia
- mantra of “each hour counts” for treating meningitis
JAMA
- 35% increase in the firearm homicide rate in the US between 2019 and 2020
- Physicians can reduce gun violence and suicide by discussing gun safety with their patients.
Treatment of Menopause Symptoms With Hormone Therapy
- Studies have shown that systemic menopausal HRT is effective for treating vasomotor symptoms (hot flashes and night sweats). These treatments are also effective for treating genitourinary syndrome of menopause. However, for vaginal or urinary symptoms without vasomotor symptoms, low-dose vaginal estrogen is recommended.
- Individuals who have menopause-related hot flashes and/or night sweats that are negatively affecting their sleep and quality of life and who are not at high risk of blood clots, breast or endometrial cancer, or heart disease may be good candidates for systemic hormone therapy
Journal of Emergency Medicine
None
Lancet
None
NEJM
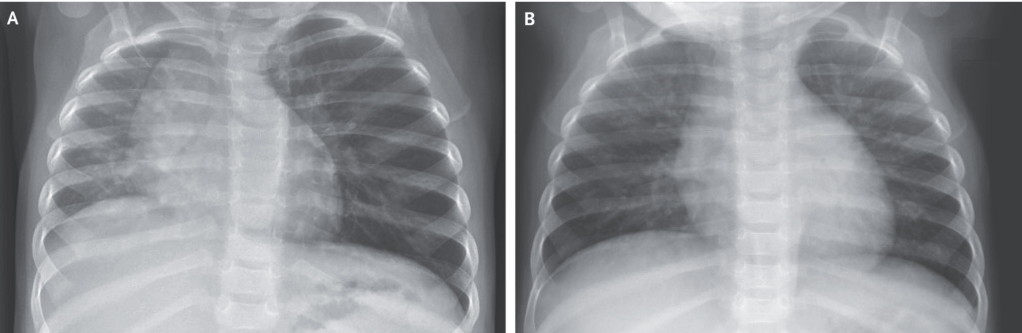
Foreign-Body Aspiration in a Child
PEDIATRICS
Nonoperative Management of Uncomplicated Appendicitis
- Retrospective
- 14.1% underwent NOM.
- The odds of NOM significantly increased (odds ratio 1.10 per study quarter, 95% confidence interval [CI] 1.05–1.15).
- The 1-year and 5-year failure rates were 18.6% and 23.3%, respectively. Children who experienced failure of NOM had higher rates of perforation at the time of failure than did the general cohort at the time of initial presentation (45.7% vs 37.5%, P < .001).
- Patients undergoing NOM had higher rates of subsequent related emergency department visits (8.0% vs 5.1%, P < .001) and hospitalizations (4.2% vs 1.4%, P < .001) over a 12-month follow-up period.
Weighing the Risks and Benefits of Nonoperative Management of Appendicitis
- There are several multi-institutional prospective trials underway which should help guide the decision.
REBELEM
REBEL Core Cast 81.0 – Priapism
- Ischemic (low flow)
- Emergency
- Much more common
- Blood gas (perform when cause is uncertain) of corpus cavernosa shows black blood which has pO2<40, pCO2>60, pH<7.25 (UPTODATE)
- Causes
- Pediatric: Sickle cell disease, leukemia
- Adult: Intercavernosal injection (papaverine, phentolamine, PGE1), Anticoagulation, Pharmaceuticals (SSRIs, sedative-hypnotics, erectile dysfunction medications), Illicit drugs (cocaine, ecstasy)
- Noniscemic (high flow)
- Excess arterial inflow resulting in priapism
- Often painless
- Blood gas: pO2>60, pCO2<40, pH>7.25
- Common causes
- Arterial laceration
- Spinal trauma
- Orders
- CBC, Retic count (for sickle cell disease patients)
- Cavernosal blood gas
- 1% lidocaine
- Sterile drapes, Betadine, Sterile Gloves
- Needles: 19g butterfly, 27g needle, 18g needle
- 2 sterile bowls (one holds the NS mixed with phenyl, one to dispose of aspirated blood)
- Or you can use a 3 way stopcock with tubing directly connected to the 500cc NS bag with phenylephrine.
- 10cc syringe x 3
- 500cc NS mixed with 1mg phenylephrine for irrigation.
- 500mcg phenylephrine mixed with 1cc NS for injection.
- Management
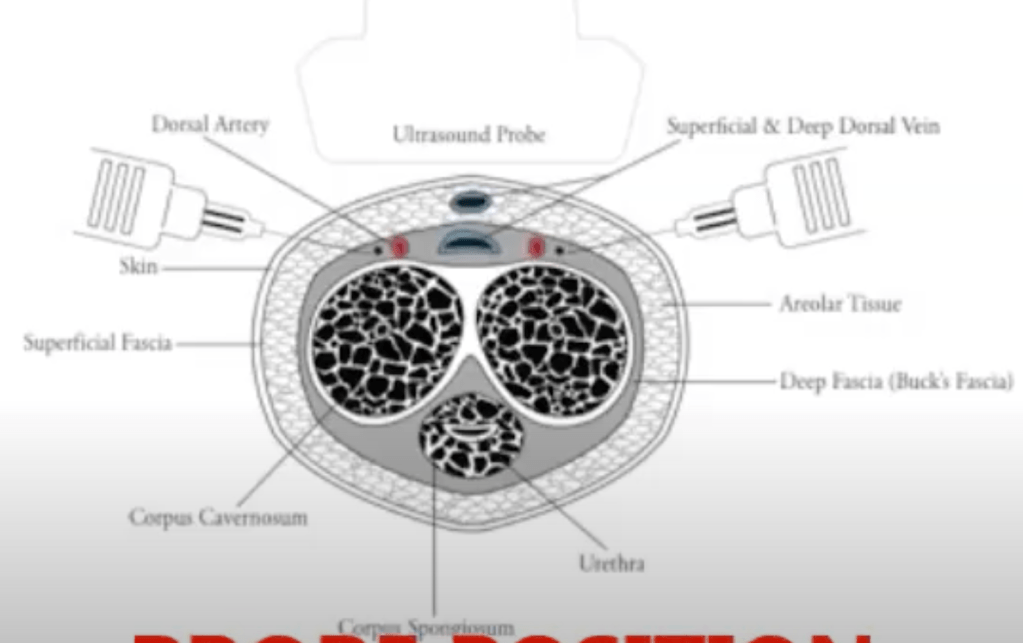
- Dorsal Nerve ultrasound guided block https://www.youtube.com/watch?v=lCZq-LEcrjA from the ventral probe position and https://youtu.be/ddpp_wfqNjk which shows the block from the dorsal probe position (see picture below), performed at the base of the penis.
- Can also do a local weal at injection site or a penile ring block.
- If priapism < 4 hours UPTODATE recommends starting with phenylephrine injection (500mcg phenylephrine mixed with 1cc NS for injection).
- If priapism > 4 hours, UPTODATE recommends combining aspiration with irrigation and phenylephrine injection.
- Inject Phenylephrine 200 – 500 mcg (diluted in 1 ml of NS) intracorporal (can use the same 19g butterfly needle per UPTODATE)
- Aspirate using 10ml syringe
- All injecting and aspirating can be done from the base of one corpus cavernosum at either 10 or 2 o’clock because the two cavernosa communicate.
- Dorsal Nerve ultrasound guided block https://www.youtube.com/watch?v=lCZq-LEcrjA from the ventral probe position and https://youtu.be/ddpp_wfqNjk which shows the block from the dorsal probe position (see picture below), performed at the base of the penis.
REBEL Core Cast 80.0 – Compartment Syndrome
Resuscitation
None
