Academic Emergency Medicine
American Journal of Emergency Medicine
None
Annals of Emergency Medicine
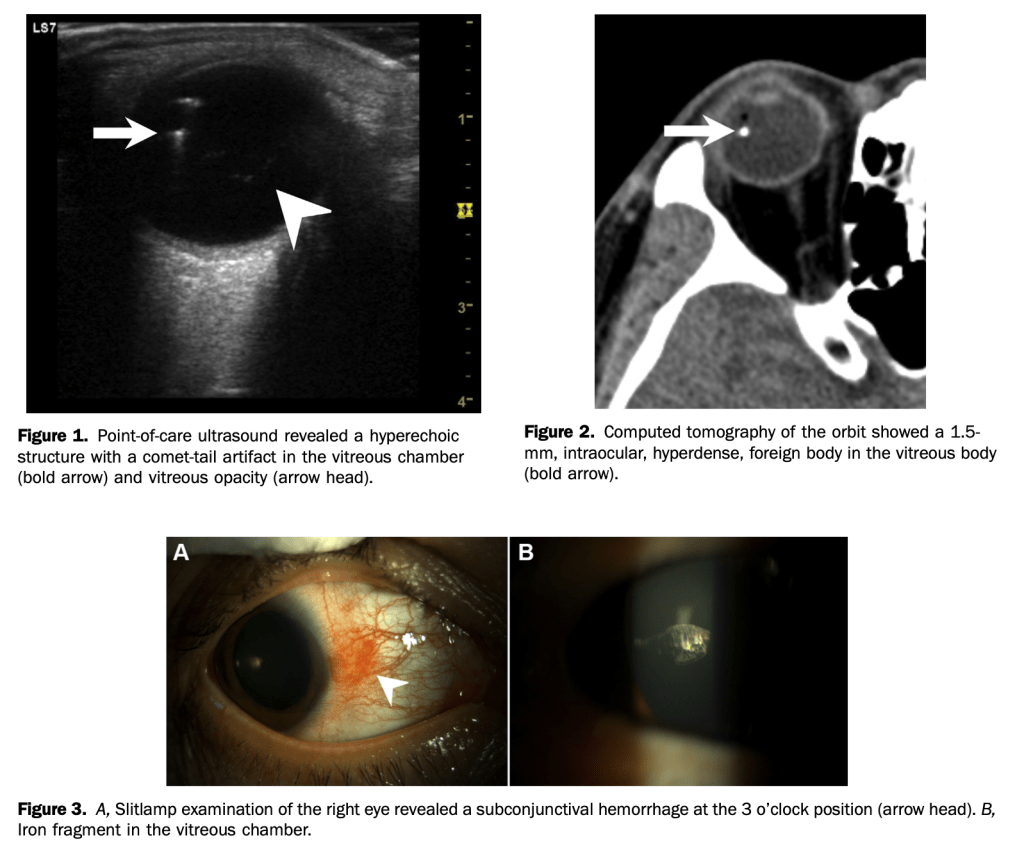
Man with right eye pain and decreased vision
Man presents to ED with right eye pain and decreased vision after hammering a nail.
BMJ
- 12 weeks better than 6 weeks
Circulation
None
CJEM
The HINTS exam is a skill emergency physicians need to learn, apply and master
Just the facts: point‐of‐care ultrasound for the diagnosis and management of acute heart failure
Just the facts: How to diagnose and manage acute preschool asthma in the ED
EMCRIT
Association Between Time to Source Control in Sepsis and 90-Day Mortality
Excluding Hollow Viscus Injury for Abdominal Seat Belt Sign Using Computed Tomography
- Like hip fractures, plain films also miss pelvic fractures
Emergency Medicine Journal
EMRAP
Macgyver Hacks: Bugs and Enemas
Shock Index and Diastolic Shock Index
First10em
Dose VF: A double sequential defibrillation game changer?
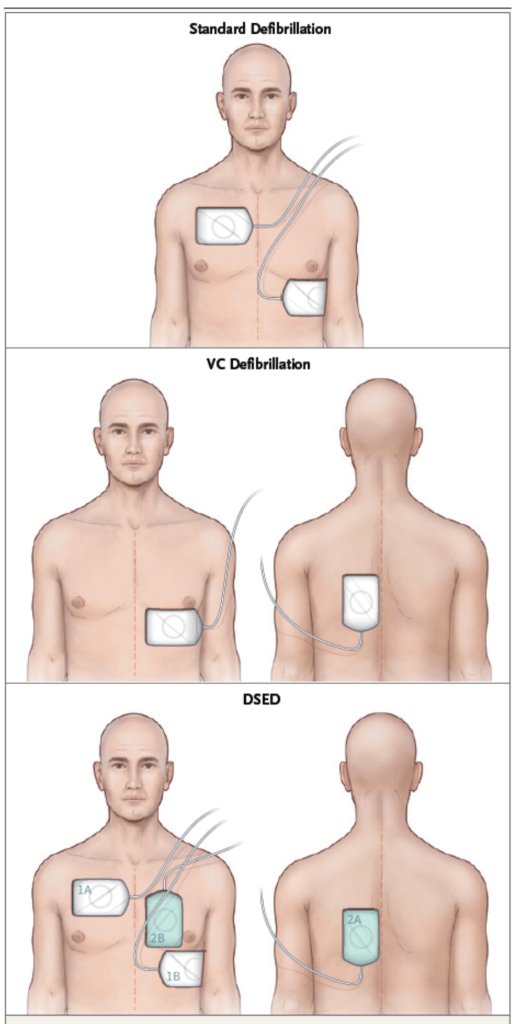
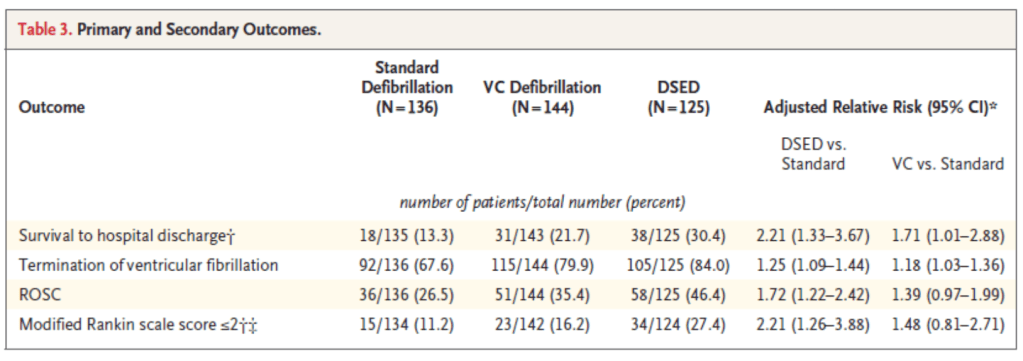
- Study in NEJM looked at out of hospital arrest with refractory vfib or pulseless Vtac after 3 failed attempts at defibrillation.
- Commentary by First10em:
- It has never made any sense to continue to provide the same unsuccessful therapy over and over again, so I think all of us have been changing something after 3 unsuccessful shocks, whether it was simply changing pad position, or adding a second machine.
- Working in a community hospital without access to ECMO or the cath lab, if I have a patient in refractory ventricular fibrillation after 3 shocks, I will perform one of these techniques, but that actually isn’t a change from current practice. I think the plan that might make the most sense is to apply a new set of pads in the anterior-posterior position after the 3rd unsuccessful shock, provide one vector change shock (to limit the risk of machine damage while still gaining potential benefit), and then if that didn’t work try double sequential for the next attempt. I think the potential benefit is worth the relatively limited risk in a hospital setting.
- However, I will continue to emphasize that this is not standard of care, and this is not definitely proven, and we definitely need to see follow-up RCTs.
Are sterile gloves necessary when repairing lacerations in the emergency department?
- No
JAMA
None
Journal of Emergency Medicine
November not yet available
Lancet
None
NEJM
Focused Cardiac Ultrasonography for Right Ventricular Size and Systolic Function
Defibrillation Strategies for Refractory Ventricular Fibrillation
Oxygen-Saturation Targets for Critically Ill Adults Receiving Mechanical Ventilation
Noninvasive Respiratory Support for Adults with Acute Respiratory Failure
PEDIATRICS
None
REBELEM
None
Resuscitation
None
