Academic Emergency Medicine
- MELD 3.0 available on MDCALC if you search for MELD
Annals of Emergency Medicine
Risk of Delayed Intubation After Presumed Opioid Overdose in the Emergency Department
- Only 0.6% of patients with opioid overdose
- Of the 1,591 patients included, only 9 (0.6%) required delayed intubation. Eight of these patients had nonrespiratory-related conditions contributing to the need for intubation. One patient only had respiratory-related conditions, had respiratory acidosis, and received a total of 6.4 mg naloxone before intubation.
EMCRIT
EMCrit RACC-Lit Review – June 2025
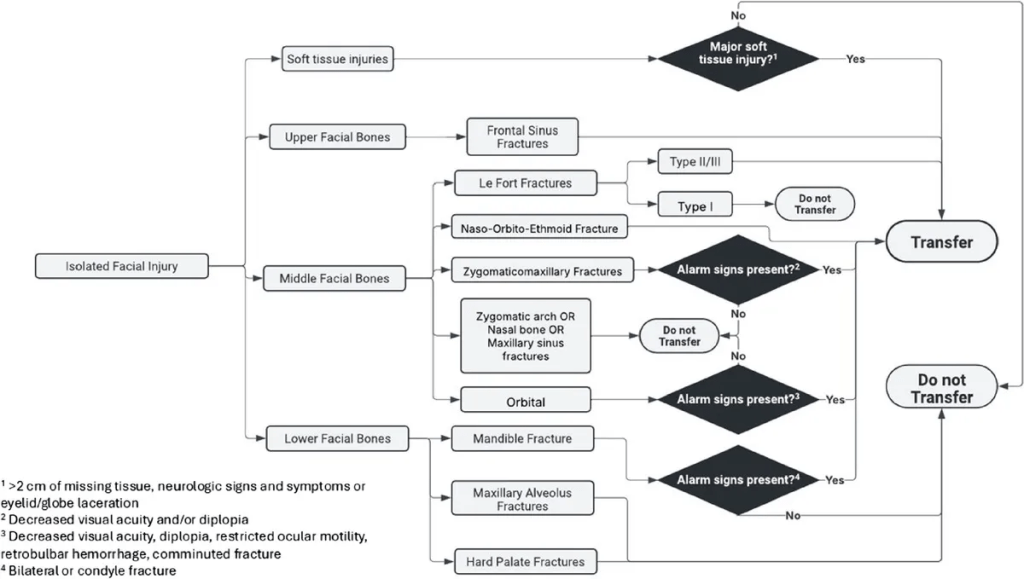
- Look Me in the Face and Tell Me That I Needed to Be Transferred: Defining the Criteria for Transferring Patients with Isolated Facial Injuries.” The Journal of Trauma and Acute Care Surgery, May 9,
- Shock index identifies compensated shock in the ‘Normotensive’ trauma patient
- Patients with SBP > 90 mmHg on arrival were identified from our trauma center registry. SI was calculated by arrival heart rate divided by arrival SBP. Patients were stratified by SI using the following thresholds: ≤ 0.7,
- > 0.7 to 0.9 odds ratio to receive blood within 1 hour: 2.5
- > 0.9 to 1.1 8.2
- > 1.1 to 1.3 24.9
- > 1.3 59
- Among 2846 patients, major adverse events occurred in 919 (32.3%) intubations, most frequently new hemodynamic instability (20.0%), followed by severe hypoxemia (12.5%) and cardiac arrest (3.5%). The overall 28-day mortality was 45.1%. Patients experiencing any major adverse event had a significantly higher 28-day mortality (57.6 vs 39.2%; aHR 1.43, 95% CI 1.26–1.62; p < 0.001). Sensitivity analyses confirmed these findings. Successful first-attempt intubation was associated with a reduced likelihood of major adverse events (aOR 0.52; 95% CI 0.41–0.65; p < 0.001).
- Results suggest that 0° head positioning for patients with acute LVO was a protective maneuver to maintain clinical stability in the prethrombectomy phase while awaiting definitive treatment.
EMCrit Guest Post – In Defense of Dignity by Chris Hicks, MD
- Cites last month’s post Mind of the Resuscitationist 4 goals of the resuscitationist:
- Save Lives/Curative Care
- Relieve Suffering
- Enhance Dignity
- Find Connection
- Deep dive on enhancing dignity
- 1. Stop talking around your patients
- 2. Constant updates
- 3. Say their name
- 4. Shared decision making
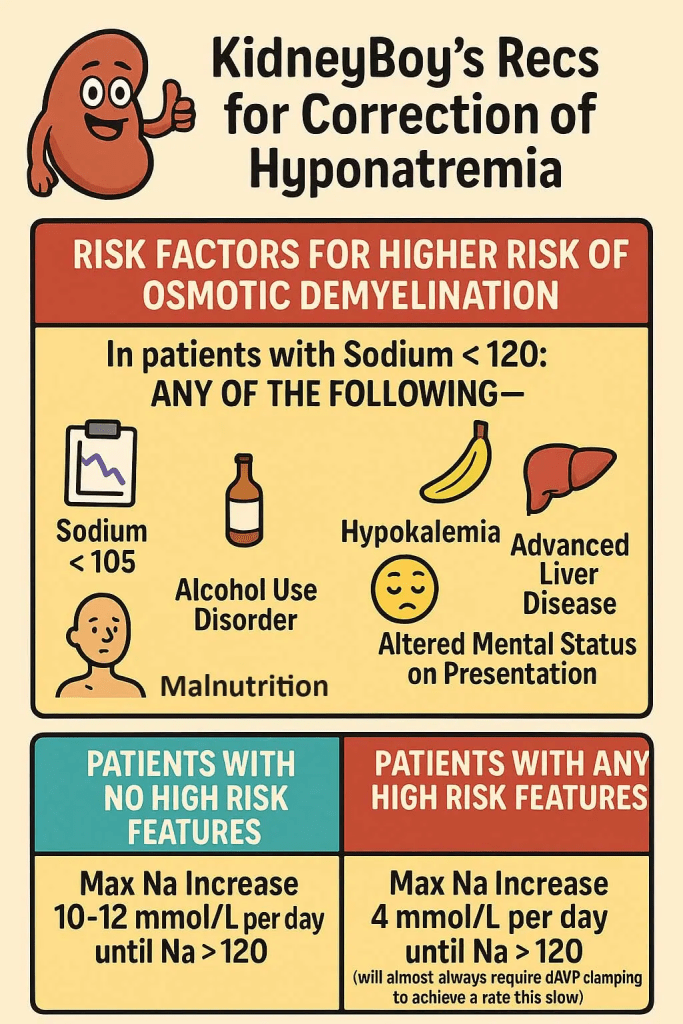
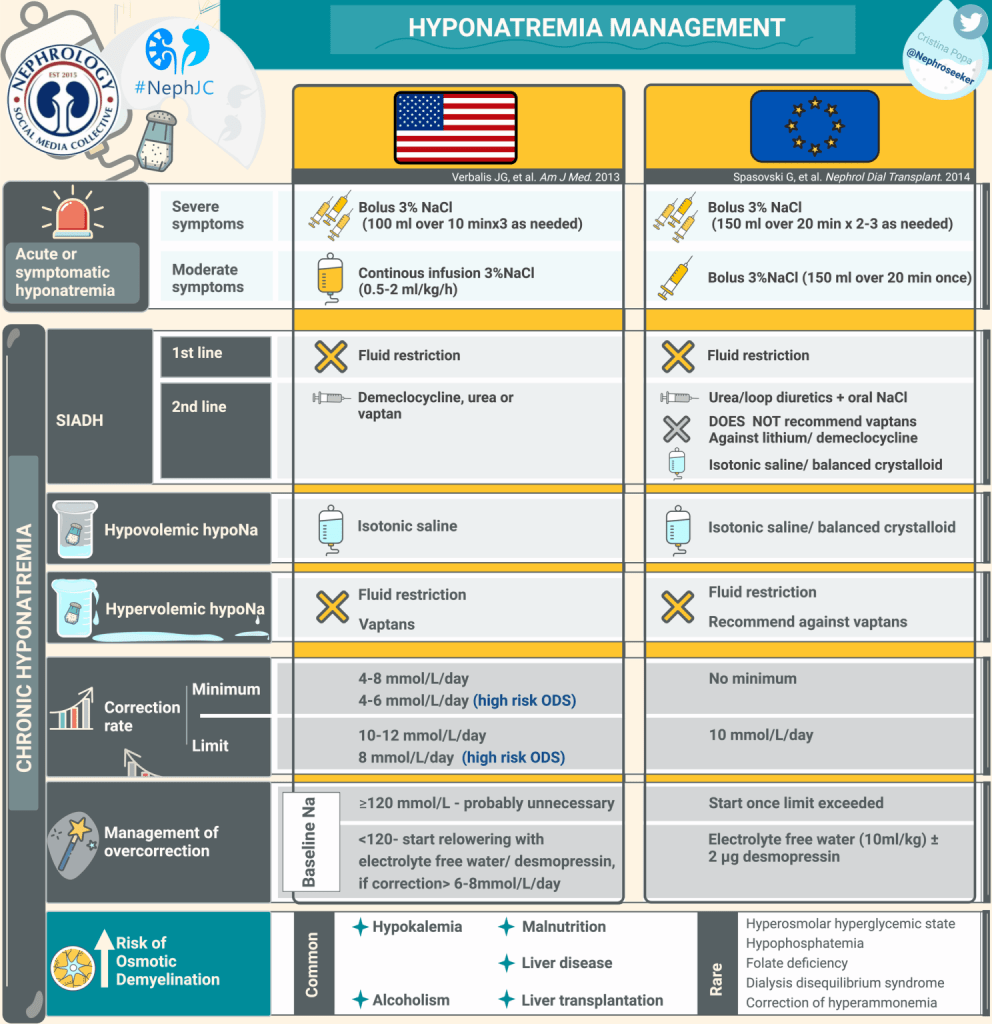
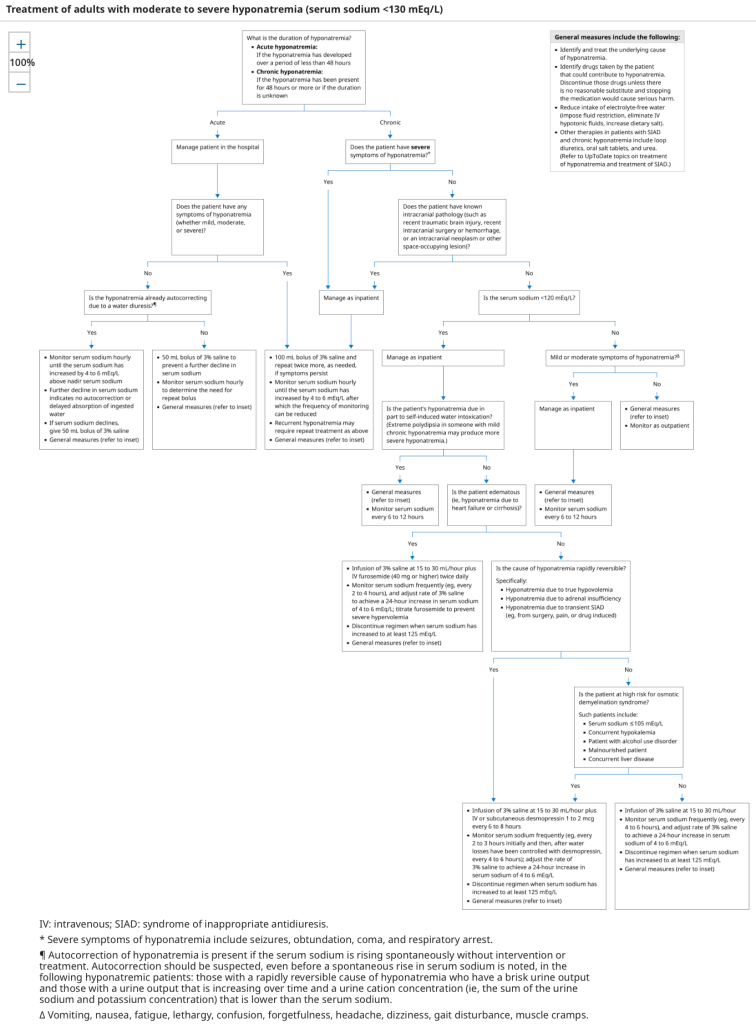
- New Systematic Review found that patient’s had worse outcomes with slow correction
- Comparative studies assessing
- rapid (≥8-10 mEq/L per 24 hours) vs
- slow (<8 or 6-10 mEq/L per 24 hours) and
- very slow (<4-6 mEq/L per 24 hours) correction of severe hyponatremia (serum sodium <120 mEq/L or <125 mEq/L plus severe symptoms) in hospitalized patients.
- Slow correction and very slow correction of severe hyponatremia were associated with an increased risk of mortality and hospital LOS compared to rapid correction.
- Rapid correction was not associated with a statistically significant increased risk of ODS.
- Comparative studies assessing
- 2 Approaches offered in the post:
OR
Needles fail, use a knife.
EMCrit Wee – Ketamine for Early Status Epilepticus Debate with First10EM

EMRAP
Diabetes in Your Feeties
Whitney Johnson, MD, and Evan Laveman, MD
Treatment
- Do not give antibiotics if there is no erythema, local swelling, or signs of inflammation.
- Diabetic wounds can be chronic and can take a long time to heal.
- These patients respond well to long-term wound care.
- >50% of diabetic wounds that do appear to be infected are caused by Staphylococcus.
- The bioavailability of PO vs IV antibiotics is similar, and many DFIs can be treated with PO antibiotics.
- Mild infections: 7-14 day course of antibiotics
- Osteomyelitis: 4-6 weeks of antibiotics
Dressings
- Wet to dry dressing (once-a-day dressing change)
- Xeroform dressing with overlying gauze
- Gentle wrap (not tight or compressive wrapping)
- Do not use non-adherent dressing or leave wound open
- Do not use hydrogen peroxide on wound
Wound Care Centers
- Wound care centers provide management and long-term treatment of surgical wounds, diabetic foot infections, and chronic wounds.
- DFIs can take months to a year to heal completely.
- Wound care centers are a great resource for patients: someone is familiar with their wounds and knowledgeable about the entire course of treatment.
- Wound care centers can manage footwear, order orthotics and do vascular assessments, assess need for lower extremity stents, manage lower extremity edema, and speak with orthopedic surgery and vascular surgery.
Novel Therapies
- Hyperbaric oxygen therapy for DFIs
- Breathing in compressed oxygen in a compressed environment
- Taking place across the lungs and hyperoxygenating the blood
- Hyperbaric oxygen therapy is helpful for DFIs, wound healing, and osteomyelitis because these areas can have poor microvascular circulation and oxygen tension.
- Poor microvascular circulation = poor oxygen-mediated immune response, poor effectiveness of antibiotics, and poor wound healing.
- Generally, 4 weeks of aggressive wound care is required before considering hyperbaric therapy.
- It is used in cases where wounds are taking much longer to heal than anticipated or where there are elements of chronic/refractory osteomyelitis.
Disposition
- A patient who is not systemically ill and does not have any signs of severe peripheral arterial diseases can be discharged home:
- Palpable pulses, capillary refill ❤ seconds, no evidence of sausage digit swelling
- Can follow-up within 1-2 weeks with primary care or wound care physician
- Patients who do not have good outpatient follow-up can return to ED 2 weeks after antibiotic course for wound recheck.
- Consider referring patients to a wound care center or wound care physician.
- Look at the patient’s footwear.
PEARL: Look for signs of acute infection on top of chronic diabetic foot wounds. High-risk features include systemic signs of infection (tachycardia, fever) and/or erythema, edema (> 2 cm beyond wound), or warmth. Consider referring patients to a wound care center or wound care physician.
Hypokalemia
Anand Swaminathan, MD, and George Willis, MD
Dr. Anand Swaminathan and Dr. George Willis take a deep dive on hypokalemia. Their conversation will take your management of hypokalemia to the next level. Part 1 covers the clinical presentation of hypokalemia and potassium repletion.
- Clinical Presentation
- Patients may complain of fatigue or feeling run down.
- Cardiac effects include dysrhythmias, including torsades.
- There may be neuromuscular weakness and, in extreme cases, paralysis or rhabdomyolysis.
- Potassium Repletion
- There is no significant difference in efficacy between different forms of potassium:
- May administer potassium bicarbonate or potassium citrate in the acidotic patient
- May opt to avoid potassium chloride in the hyperchloremic patient
- May administer potassium phosphate in the hypophosphatemic patient
- 10 mEq of potassium repletion results in a 0.1 mEq/L change in serum potassium level.
- Potassium levels <3.0 mEq/L will require much larger amounts of repletion to affect serum levels.
- Oral repletion
- Preferred method of repletion
- Best suited for mild hypokalemia (>3.0 mEq/L)
- Can give 40-60 mEq/hour
- Peripheral IV lines
- Best suited for PO-intolerant patients or levels <3.0 mEq/L
- Maximum rate of 10 mEq/hour to avoid painful irritation to small veins
- Can achieve faster rates by giving through multiple IVs or mixed into IV fluids
- Central venous lines
- Reserved for profound hypokalemia and unstable patients
- As fast as 80 mEq/hour
- Patients should be on continuous cardiac monitoring
- For patients in cardiac arrest secondary to hypokalemia, you can push 40 mEq of potassium chloride through a peripheral IV.
- Recheck potassium levels at least 1 hour after IV repletion to allow time for intracellular shifts.
- There is no significant difference in efficacy between different forms of potassium:
- Magnesium Repletion
- Hypomagnesemia results in renal potassium wasting.
- IV, rather than oral, magnesium repletion is required for hypomagnesemic patients.
- Magnesium levels of 1.0 or less:
- Give 4 g of magnesium prior to potassium repletion
- Magnesium levels of 1.5 or higher:
- Give 1-2 g of magnesium prior to potassium repletion
- Disposition
- ICU indications
- Patients with neuromuscular complaints – require monitoring for diaphragmatic involvement and respiratory compromise
- Severe ECG findings, including non-sustained ventricular tachycardia, multiple premature ventricular contractions (PVCs), torsades, or prolonged intervals
- Level-specific hospital policy
- Admission
- Patients with levels <2.8 mEq/L will require ~30 mEq to cause 0.1 mEq/L change in serum potassium level
- Moderate to severe cases where a cause has not been identified
- Discharge home
- Patients with levels >3.0 mEq/L and mild symptoms can be discharged without repeat level after repletion.
- Patients with levels of 2.8 to 3.0 mEq/L can be discharged after repletion and a repeat level.
- If patients are taking thiazide or loop diuretics, consider starting low-dose potassium supplementation with close follow-up
- Counsel patients regarding high-potassium foods (eg, banana, orange juice, sweet potato, avocado).
- ICU indications
IV Antibiotics Aren’t Special
Justin Morgenstern, MD
Is the PO (oral) route the way to go? Intravenous (IV) antibiotics are NOT superior to oral antibiotics and show identical treatment efficacy in multiple studies for different types of infection.
Introduction
- The antibiotic (despite route of administration: PO or IV) is an identical molecule, no matter how it got into the body.
- The only thing that matters is the concentration of that molecule and how much actually makes it into the tissues (bioavailability).
- If there is a pill formulation of an antibiotic, it will have decent bioavailability.
- The oral route usually takes 30 minutes longer to absorb compared with IV.
- For oral antibiotics to work, the patient needs to have a functional gastrointestinal (GI) tract.
- IV is a better route for patients who may be hypoperfusing their GI tract (eg, critically ill or vomiting patient).
- To date, there are no articles on PubMed that demonstrate that IV antibiotics are superior to oral antibiotics.
Pyelonephritis
- 2014 Cochrane Review
- 27 randomized controlled trials (RCTs) with 4,500 patients across a range of outcomes:
- No differences between IV and oral
- 27 randomized controlled trials (RCTs) with 4,500 patients across a range of outcomes:
- 2007 Cochrane Review
- 15 RCTs with both adult and children with severe urinary tract infection (UTI)/pyelonephritis:
- No evidence that oral antibiotics are less effective than IV
- 15 RCTs with both adult and children with severe urinary tract infection (UTI)/pyelonephritis:
- An RCT in pregnant women with pyelonephritis (excluded patients with bacteremia):
- IV and oral antibiotics had identical outcomes
- An RCT that compared IV and oral ciprofloxacin for hospitalized patients with severe pyelonephritis:
- Outcomes were identical
Pneumonia
- Multicenter RCT of 1,700 children comparing IV penicillin to amoxicillin:
- Treatment failure was identical
- Multicenter RCT with more than 2,000 children comparing IV ampicillin to oral amoxicillin:
- Oral antibiotics were just as good as IV
- Multicenter RCT with only 100 adult patients:
- Oral fluoroquinolone is equal to IV cefotaxime
- Single-center RCT with 85 hospitalized patient with non-severe pneumonia were randomized to receive IV versus oral antibiotics:
- No difference between IV and oral
Other Types of Infections
- There are good data for endocarditis, febrile neutropenia, and acute osteomyelitis, showing that oral antibiotics are as good as IV antibiotics.
- The OVIVA trial had more than 1,000 patients with complex orthopedic infections:
- Septic arthritis, prosthetic joint infections, vertebral osteomyelitis, and discitis
- Patients needed 6 weeks of antibiotics (randomized to receive oral vs IV) and outcomes were identical
Oral vs IV Antibiotics in the Hospital
- Oral antibiotics promote movement and ambulation, whereas IVs can keep patients bed bound.
- IV supplies are more expensive than pills.
- IV placement and maintenance is more time consuming for nursing staff.
- IVs have high risk for infection, clotting, and patient harm.
PEARL: IV antibiotics are NOT superior to oral antibiotics. Take into consideration when IV antibiotics may be the better treatment choice (eg, for critically ill patients or patients who cannot tolerate PO or are vomiting).
First10 EM
None
NEJM
None
REBELEM
REBEL Core Cast 138.0: A Simple Bedside Approach to Shock
- Narrow Pulse Pressure? Cardiogenic, hypovolemic, or obstructive shock
- Wide Pulse Pressure? Distributive shock
REBEL Core Cast 134.0 – Acetaminophen Toxicity
Definition and Physiology
- After ingestion of a therapeutic dose, immediate release APAP is absorbed with a time to peak concentration anywhere between 30-45 minutes. In the context of extended-release, formulations, full absorption is typically reached by 4 hours post-ingestion.1
- In therapeutic dosing, the vast majority of APAP undergoes hepatic conjugation with glucuronide or sulfate to form benign metabolites that ultimately get excreted in the urine. The remaining ~5% is oxidized by CYP2E1 to form N-acetyl-p-benzoquinoeimine (NAPQI). NAPQI is hepatotoxic. Glutathione combines with NAPQI to generate non-toxic metabolites that are also eliminated in the urine.
Clinical Manifestations and Diagnostic Evaluation
- The clinical course of acute APAP toxicity is classically broken into four different stages.
- Stage1: this is generally within 24 hours. Patients are either asymptomatic or have non-specific GI symptoms (nausea, vomiting, malaise). At this point, hepatic function testing is normal.
- Stage2: ~24-72 hours. The onset of hepatic injury marks this stage. Aspartate aminotransferase (AST) is the most sensitive marker to detect hepatic dysfunction; AST elevated is nearly universal by 36 hours post-ingestion.
- Stage3: defined as peak hepatotoxicity; generally between 72-96 hours post-ingestion. Patients may manifest hepatic encephalopathy or coma. AST and/or ALT might rise above 10,000 IU/L. Other lab abnormalities include: INR/PT, glucose, lactate, pH, and creatinine. Death from fulminant hepatic failure usually occurs anywhere between 3-5 days after an acute ingestion. Mortality is often secondary to multiorgan failure, ARDS, sepsis, or cerebral edema.
- Stage4: often called the “recovery phase.” Patient who survive demonstrate complete hepatic generation without any evidence of hepatic dysfunction.
- The following labs should be obtained for severe APAP ingestions:
- APAP Concentration, hepatic panel, pH, coagulation panel, renal function, lactate and phosphate. These labs will ultimately dictate disposition (see King’s College Criteria below)
Management
- Consider GI decontamination with activated charcoal as this can reduce systemic absorption and limit subsequent clinical sequalae.
- Ingestions should be classified as acute or repeated supratherapeutic (“chronic” ingestions)
- Single Acute Ingestion
- If feasible, obtain a 4 hour post-ingestion APAP concentration. Any concentration earlier than 4 hours is uninterpretable as subsequent concentrations may increase or decrease depending on the clinical scenario.
- Concentrations between 4-8 hour post-ingestion can be plotted on the Rumack-Matthew nomogram to determine when NAC should be initiated.
- If the APAP concentration is above the plotted line, NAC should be started.
- NAC is nearly 100% effective if started within 8 hours post-ingestion.2
- If an APAP concentration is unable to be drawn before 8 hours or if LFTs are already elevated, NAC should be empirically started if the pre-test probability is high enough for clinical concern.
- Repeated Supratherapeutic/Chronic Ingestions
- Cannot apply the Rumack-Matthew Nomogram
- If LFTs are elevated or if there is a positive APAP concentration, NAC should generally be started however consultation with a toxicologist or Poison Control Center is advised as these cases are often complicated.
- Single Acute Ingestion
- N-Acetyl-Cysteine (NAC)Dosing
- “3 Bag Protocol” – 21 hour regimen
- 150mg/kg over 1 hour loading dose
- 50mg/kg over 4 hours = 12.5 mg/kg/hr
- 100mg/kg over 16 hours = 6.25 mg/kg/hr
- Risk: anaphylactoid reaction
- Reaction is rate related and typically occurs during the loading dose
- Symptoms: flushing, urticaria.
- NAC should be continued until all of the following criteria are met:
- Negative APAP concentration
- “Significant Decreased in AST”: defined as either <1000 IU/L or a 25-50% drop from the peak.
- No evidence of hepatic failure
- If criteria are not met, the third bag should be extended indefinitely.
- “3 Bag Protocol” – 21 hour regimen
- The King’s College Criteria should be used as this set of lab work is used to determine which patients should be referred for possible liver transplant evaluation.3, 4
Take Home Points
- In overdose, acetaminophen leads to generation of NAPQI which is hepatotoxic. N-Acetylcysteine (NAC) is the antidote of choice and ideally should be administered within 8 hours of an acute ingestion.
- To determine which patients should be treated with antidotal therapy, the Rumack-Matthew Nomogram should be utilized. Of note, this nomogram was validated for a single concentration obtained at or greater than 4 hours after a single, acute ingestion. (i.e. patients with repeated ingestions cannot be applied to the nomogram).
- In patients with a high pre-test probability of APAP poisoning, the King’s College Criteria should be considered; this is a set of lab markers that help determine when patients should be immediately referred for liver transplant.
- While physiologic plausibility exists for the use of fomepizole to treat severe APAP toxicity, no large scale human studies exist at this time to suggest that it should be routinely given for toxicity. As with all cases of toxicity, please call your local poison control center for assistance.
Combination Inhalers in Asthma: Time to Switch?
- Prescribe comb inhalers (LABA/ICS) for rescue therapy to patients with asthma in addition to their maintenance medications. The inhaler of choice may vary based on cost and availability.
