Academic Emergency Medicine
Annals of Emergency Medicine
- From January 1 to October 31, 2023, NOO syphilis cases in Chicago were identified more frequently in persons who did not have HIV and who were not MSM compared with cases identified in 2019.
- Clinicians should consider NOO syphilis even in persons who do not have HIV and who are not MSM. Enhanced surveillance efforts to better understand NOO syphilis trends are needed.
- Non treponemal testing (RPR, VDRL) is the typical screening test because it generates a titer to determine if the patient has active disease.
- A treponemal test is recommended by the CDC as a follow-up confirmatory test before treating.
- Bridge has a treatment algorithm based on a positive result but their endnote states that any positive screening test should be confirmed based on local protocol.
Bridging the Gap: Understanding “Normal” Osmole Gap in Theory and Clinical Practice - Given the limitations of an osmose gap, we suggest that an osmole gap be interpreted within the individual clinical context. In patients presenting with osmole gap elevations up to 25 mOsm/kg, without attendant metabolic acidosis and history of toxic alcohol ingestion, rule out ketosis and contracted plasma volume and obtain a confirmatory test for toxic alcohol before administering fomepizole. If confirmatory tests are unavailable or delayed, monitor acid-base status and osmole gap every 4 hours. Administer fomepizole with onset of acidosis and osmole gap decline. Conversely, in patients with features consistent with toxic alcohol toxicity such as metabolic acidosis with visual disturbances or oxaluria, promptly initiate fomepizole alongside confirmatory testing, irrespective of the osmole gap. Consult nephrology and toxicology for all patients on fomepizole to guide the need for hemodialysis and treatment duration.
Anticoagulation Should Not Be Routinely Used for Isolated Subsegmental Pulmonary Embolism
Patients With Isolated Subsegmental Pulmonary Embolism Should be Treated With Anticoagulation - This is another great pro/con that the Annals publishes on controversial topics.
- I side with no anticoagulation but would include shared decision making with the patient. The 2018 ACEP guideline and the 2021 ACCP offer a weak recommendation for surveillance over anticoagulation of isolated subsegmental PE if there is no proximal deep vein thrombosis (DVT) and low risk for recurrence. The authors of the pro anticoagulation argue that it is too much hassle to order a bilateral duplex of the legs after the CTA result comes back which is a valid point. Seems easiest to let the patient call the shots.
- ACEP policy statement recommending TXA for traumatic hemorrhagic shock
- TXA also beneficial for postpartum hemorrhage but not GI bleed.
EMCRIT
EMCrit 408 – Behind the Scenes of an Infuriating Medical Malpractice Trial
- 21yo presented with right sided pleuritic CP and h/o Covid, discharged and later died of massive PE
- EM physician successfully sued, despite patient being PERC negative because EKG showed deep (>2mm) TWI inferiorly and V1-4
- 2 good blog posts by Stephen Smith on this pattern which represents acute right heart strain: here and here.
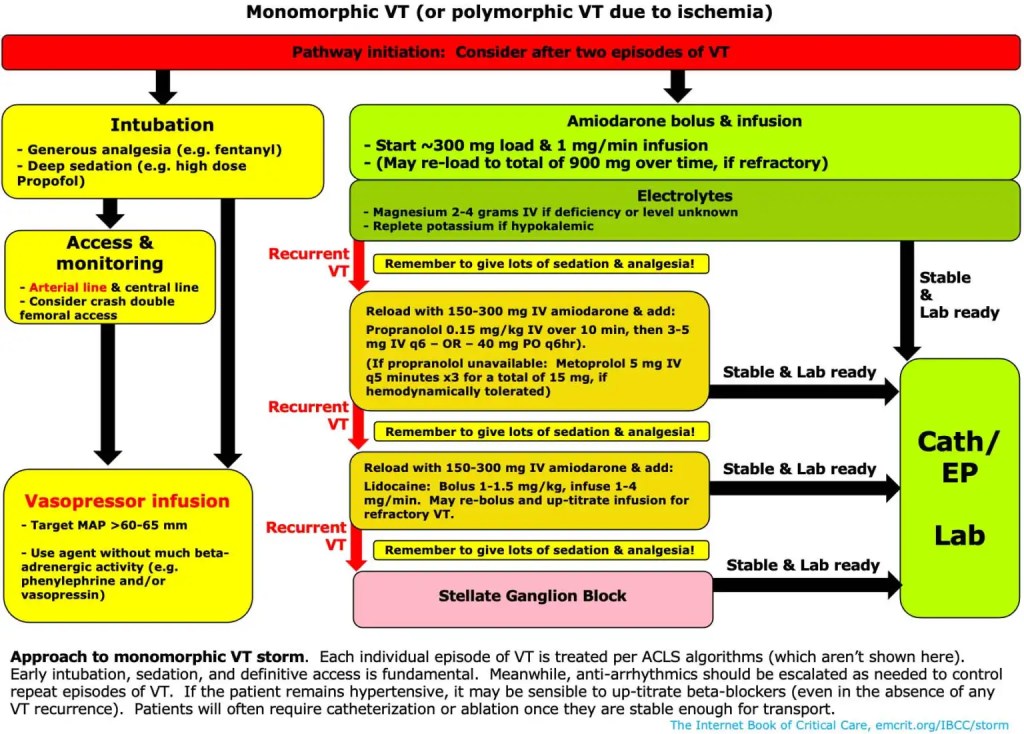
CV-EMCrit Wee – Electrical Storm: Surviving the Storm Part I
- Great topic but the summary notes were too confusing for my small brain and short attention span.
- I like this simple algorithm from Josh Farkas on how he manages VT storm.
- The one thing I took from Trina Augustin is the vaspressor choice:
- Go-to agents: Norepinephrine (0.01- 0.2 mcg/kg/min) or vasopressin (0.01-0.04 units/min)
- Avoid: Epinephrine
- How I decide:
- Normal EF: Vasopressin first line (phenylephrine probably ok)
- Reduced EF / shocky: Norepinephrine typically favored
EMRAP
EMA 2025 August Abstract 1: Pneumonia Risk After Negative Chest X-Ray in the ED
EMA EDITOR’S COMMENTARY: In this large retrospective study designed to determine how often pediatric patients’ initial negative CXRs “blossom” and show radiographic pneumonia on subsequent CXR, only 0.27% were found to later turn positive. The study has several important take-home messages. First, a negative initial CXR can be relied upon in almost all cases. Second, tachypnea, hypoxemia, and dehydration are important clinical predictors that should prompt heightened vigilance and potentially closer follow-up, even after negative imaging findings. Third, if a child returns because of worsening clinical condition, the chance of pneumonia on that visit is approximately 1 in 10.
Critical Care Mailbag: Hyperangulated VL Tips
Anand Swaminathan, MD, and Scott Weingart, MD
Hyperangulated vs standard geometry blade laryngoscopy:
- Weingart does not recommend routine use of hyperangulated blades.
- Standard geometry laryngoscopy is a skill that deteriorates.
- It is best to maintain standard geometry skills and fall back on hyperangulated if needed.
- Hyperangulated allows clinicians to get away with bad technique and use a less precise technique.
- Similarities between hyperangulated and standard geometry blades:
- Patient positioning is the same:
- Face plane parallel to the ceiling
- External auditory meatus above sternal line
- Patient positioning is the same:
- Differences with hyperangulated laryngoscopy:
- The patient can be a little bit lower because the clinician does not need a direct line of sight with this blade.
- The patient does not need to be at the xiphoid process.
- Hyperangulated blades come with a rigid, premolded stylet.
- It is designed for the clinician’s thumb to be able to push it out.
- A standard stylet can molded to the same position:
- Lazy J formation
- The clinician must hold the tube differently:
- The endotracheal tube (ETT) must be held at the very top:
- Thumb is ready to push out the top
- With standard geometry, can hold half-way
- Weingart likes to hold the tube with index and middle finger in front of the tube, then use the pinky and ring finger behind the tube.
- Thumb would be on the stylet.
- The endotracheal tube (ETT) must be held at the very top:
- Blade insertion:
- Do not stick the hyperangulated blade straight in; this would lead to pushing against tongue and hard palate.
- Insert by rotation.
- To insert, look in the mouth (not at screen) to place the tip of the blade 1 inch in on the tongue, which requires the operator to flex the wrist (ulnar flex) toward the patient’s chest.
- Lubricating the top of the blade is beneficial.
- Continue to flex and de-flex the wrist to rotate along the tongue until seated into the vallecula.
- Stop rotation when looking down the barrel of the trachea.
- At this point, glottic structures may still be obscuring the cords.
- If this is the case, gently lift to move structures out of line of sight.
- Avoid over-rotation to get a good view of the cords; this makes tube placement difficult.
- Over-rotation has occurred if the cricoid cartilage is visible.
- For tube placement, move eyes off screen and look at the mouth!
- Place it until the tip of the tube disappears.
- Move eyes back to the screen at this point.
- Using this technique decreases the likelihood of pharyngeal injuries.
- To maximize tube delivery, use the Cooper maneuver:
- Look in the mouth, insert the blade in rotatory motion, and move right along the tongue.
- As the tip disappears, look at the screen to continue rotation until dead center with the cords in horizontal plane.
- You want to be 1-2 cm back from the glottis and 1-2 cm below the glottis directly center in the horizontal plane.
- Lift up on the tube with a small tilt to advance forward, then insert.
- One downfall is a locked stylet, where it is difficult to remove the stylet from the tube in hyperangulated form
- “Popping it” – pulling the stylet back an inch – can help remove the stylet and help with delivery.
- Before removing the stylet, grab the tube with the hand that has the laryngoscope.
- To remove stylet, derotate the stylet out. If you pull straight out, the tube will also come out.
- Look in the mouth, insert the blade in rotatory motion, and move right along the tongue.
- The patient can be a little bit lower because the clinician does not need a direct line of sight with this blade.
Why are there issues with tube delivery when there is a pristine view of the cords?
- The tip of the blade is blocking the ingress of the tube, and the angle created limits tube delivery.
- If stuck with this situation, pull the blade back.
- Dr. Weingart mentions that the goal is to keep the camera angle parallel to the floor. This allows you to have a straight shot down the trachea when the patient is flat.
PEARLS:
- It is important to watch the patient’s mouth during hyperangulated blade laryngoscopy to visualize the blade and tube entering to avoid pharyngeal injuries.
- Using hyperangulated blades exclusively can lead to deterioration of standard geometry laryngoscopy skills.
- A lesser view is better for tube delivery!
- For blade insertion, tube delivery, and stylet removal, rotation is critical. The tube can be removed if the stylet is pulled directly up and out.
Nick Chrimes Video: Hyperangulated Videolaryngoscopy Virtual Workshop
Trauma Potpourri: Kenji’s Takes
- Abdominal Seatbelt Sign
- Case: A patient presents to the ED after a motor vehicle collision, with a seatbelt sign across their abdomen.
- Are modern computed tomography (CT) scanners missing hollow viscus and bucket handle tears associated with the abdominal seatbelt sign?
- The historical train of thought was that CT scan can miss hollow viscus and bucket handle tears.
- Bucket handle tears occur when the seatbelt compresses the gastrointestinal (GI) tract against the spine.
- Mesentery can shear away from the bowel.
- Previously, patients were admitted or serial exams performed if there was high clinical suspicion.
- Bucket handle tears occur when the seatbelt compresses the gastrointestinal (GI) tract against the spine.
- The historical train of thought was that CT scan can miss hollow viscus and bucket handle tears.
- Concern was for bowel necrosis that can develop over 24-72 hours.
- This question was answered by a prospective multicenter study conducted by the Pacific Coast Surgical Association.
- The study was designed to determine the likelihood of bucket handle or clinically significant hollow viscus injury with negative CT.
- Results showed that the likelihood of missing an injury was near zero.
- Kenji still recommends strict return precautions and monitoring of symptoms (nausea, vomiting, pain).
ENT on Ears
Ilene Claudius, MD, and Steven Rosenblatt, MD
Drs. Ilene Claudius and Steven Rosenblatt discuss various ear pathologies and acute otitis media (AOM), uncovering tips and tricks from an expert otolaryngology (ENT) specialist.
Examining the ear:
- Getting a good exam is key.
- Have parents help hold the patient down if they’re a fussy child.
- Hold the otoscope upside down and pull the pinna back for best exposure.
- Light reflex is not as meaningful as once taught.
Tympanic membrane (TM) appearance:
- Look for normal conical shape of the eardrum. Effusion or simple fluid behind the TM does not mean infection.
- A red eardrum does not necessarily mean AOM; it can be red from crying/hyperemia.
- In AOM, the TM will lose concavity and appear white or purulent.
Ear pain beyond AOM:
- Most ear pain is not an ear infection.
- A sore throat can cause ear pain, so evaluate for causes of sore throat.
- Temporomandibular joint (TMJ) inflammation is common in teenagers and generally causes ear pain.
- Eustachian tube dysfunction may be a cause.
Perforated AOM:
- Treat similar to AOM but add ear drops to help wash out the ear canal and treat the lateral side of the TM.
- If there is no bleeding from the ear, you generally don’t need steroids added to drops.
- Ensure no swimming or submersion until the patient has finished treatment and had follow-up.
- If the patient has tympanostomy tubes and their ear is draining, they typically only need ear drops.
- Avoid ototoxic ear drops.
Foreign Bodies in the Ear:
- Remove foreign bodies in the ED if wet, organic material, bug, or water bead.
- If dry, inorganic, and non-expansile, do not undergo heroic efforts to remove them in the ED.
EMA 2025 August Abstract 11: Alzheimer Anti-Amyloid Therapy and ARIA for Emergency Docs
EMA EDITOR’S COMMENTARY: In this educational article, the authors describe new antiamyloid therapies for Alzheimer disease and explain that the medications themselves can cause neurologic symptoms including stroke mimics via the formation of new amyloid deposits that can be seen only on MRI. Simply put, if a patient taking 1 of these medications presents with what looks like a stroke, an MRI is necessary to make sure it is not actually ARIA. If it is an ischemic stroke, thrombectomy might be preferred, because the risk/benefit ratio of lytics is altered. Optimal pathways for management will need to be developed locally, and obtaining an MRI for each of these patients could be a nightmare, depending on where you work. For now, simple awareness of the issue is a good start.
Crit Bits: HFNC vs BPAP
Anand Swaminathan, MD, and Haney Mallemat, MD
Dr. Mallemat and Swaminathan discuss the benefits of high-flow nasal cannula (HFNC) and which cases or scenarios benefit the most from HFNC vs bilevel positive airway pressure (BIPAP).
- A nasal cannula (NC) can provide up to ~50% fraction of inspired oxygen (FiO2) but with limited flow.
- In respiratory distress, high inspiratory flow rates dilute the FiO2 delivered by NC or non-rebreather mask (NRB) with room air.
- HFNC can provide up to 70 L/minute depending on the model.
- They deliver higher flow than NC, blend the air with warmed humidified oxygen, and minimize turbulent flow.
- FiO2: Delivers high flow rates matching patient’s inspiratory flow rate to deliver accurate (non-diluted) FiO2.
- CO2: Washes out some CO2 in nasopharyngeal dead space, alleviating symptoms of respiratory distress.
- Positive end expiratory pressure (PEEP): In theory, PEEP can deliver 1 cm H2O for every 10 L of flow.
- PEEP is limited by patient compliance (keeping mouth closed), body habitus, and cannula fit.
- Who benefits from HFNC:
- Hypoxemic respiratory distress: Pneumonia, mild pulmonary edema, pulmonary contusions, mild chronic obstructive pulmonary disease (COPD) exacerbations, early acute respiratory distress syndrome (ARDS)
- Patient who is doing well on nasal intermittent positive pressure ventilation (NIVPP) but needs a break from the mask
- Good option for end-of-life care with symptomatic respiratory distress
- Avoid HFNC in the following cases:
- Bad COPD exacerbation: these patients benefit from the driving pressure of BIPAP to improve ventilation and CO2 clearance.
- Bad pneumonia or pulmonary edema: these patients may benefit from additional PEEP provided by well-fitting continuous positive airway pressure (CPAP) or BiPAP.
- Switch to BiPAP (or intubation) for anyone not improving on HFNC.
- Imminent respiratory failure: BiPAP may be a better rescue device and will provide better pre-oxygenation if a patient requires intubation.
PEARL: HFNC is a great tool for hypoxemic respiratory distress; it does not replace CPAP/BiPAP but may be a more appropriate modality when you do not need high PEEP or CO2 clearance.
REFERENCES:
High-flow nasal oxygen vs noninvasive ventilation in patients with acute respiratory failure: the RENOVATE randomized clinical trial
RENOVATE Investigators and the BRICNet Authors, Maia IS, Kawano-Dourado L, et al. JAMA. 2025;333(10):875-890. doi: 10.1001/jama.2024.26244. PMID: 39657981
Noninvasive ventilation for preoxygenation during emergency intubation
Gibbs KW, Semler MW, Driver BE, et al. N Engl J Med. 2024;390(23):2165-2177. doi: 10.1056/NEJMoa2313680. PMID:
Cardiology Corner: D-dimer in Renal Impairment
Anand Swaminathan, MD, and Amal Mattu, MD
Dr. Mattu and Dr. Swaminathan discuss the evidence behind and the utility of D-dimers in the evaluation for deep vein thrombosis (DVT)/pulmonary embolism (PE) in patients with renal insufficiency.
- D-dimer is partially cleared by the kidneys and may lead to “falsely” elevated D-dimers.
- In renal impairment, D-dimer is less specific and has more false positives.
- In renal impairment, D-dimer becomes more sensitive and negative results remain true.
- Age adjustment and YEARS criteria were not studied specifically in patients with renal insufficiency.
- A single-center retrospective study on critical care patients redefined cutoffs for DVT/PE in renal insufficiency:
- Glomerular filtration rate (GFR) >60: cutoff 333 µg/L
- GFR 30-60: cutoff 1,300 µg/L
- GFR <30: cutoff 1,663 µg/L
- Future tests, studies, and validation may give us new cutoffs for patients with renal insufficiency.
PEARL: In patients with renal impairment, D-dimer will often be elevated, leading to increased false positives, and this will factor into how you risk-stratify patients with potential DVT/PE. If you begin evaluating for a PE, be sure to carry out the algorithm/workup completely.
Testing and Treatment of Sexual Assault
Mel Herbert, MD, and Karen Serrano, MD
Patient-Specific Protocols for Testing and Treatment
- Adults:
- Treat empirically for sexually transmitted infections (STIs) but do not test unless the patient is symptomatic.
- A positive test may not be from the assault and could be from prior consensual contact.
- Draw baseline labs for HIV, rapid plasma reagin (RPR [syphilis]), and hepatitis B.
- Prepubertal Children (Tanner Stage 1):
- Test for everything but do not treat empirically.
- A positive test serves as legal evidence of abuse, so a confirmatory test is needed.
- The risk of pelvic inflammatory disease (PID) is very low in this group.
- Adolescents:
- Test for everything AND treat empirically.
- This approach is used because it’s unknown whether they are having consensual sex (making a positive test meaningful), and their estrogenized reproductive tract puts them at risk for complications.
Emergency Contraception
- Emergency contraception is offered to patients of childbearing age with a vagina.
- These are not abortion pills; they work by delaying ovulation.
- Drugs:
- Ulipristal (Ella) (noted as more effective)
- Levonorgestrel (Plan B)
STI Prophylaxis Regimen
- The goal is to provide the first dose of all medications in the ED.
- For Gonorrhea:
- Ceftriaxone 500 mg IM (intramuscularly).
- Dose increases to 1 g if the patient weighs over 150 kg.
- For Chlamydia:
- Doxycycline 100 mg twice a day (BID) for 7 days.
- Alternative: A single dose of azithromycin can be used if the patient is pregnant or if there are concerns about medication adherence.
- For Trichomonas:
- Metronidazole 500 mg twice a day (BID) for 7 days.
- This is generally not given to male patients unless they are symptomatic, as the infection is often transient and asymptomatic in men.
HIV Prophylaxis (Post-Exposure Prophylaxis [PEP])
- HIV prophylaxis is indicated for high-risk exposures (eg, receptive anal or vaginal intercourse) within a 72-hour window.
- Prescribe anti-nausea medication like ondansetron (Zofran) to manage side effects.
- Regimens:
- Single pill: bictegravir (Biktarvy).
- Multi-pill: emtricitabine + tenofovir (Truvada) plus a third drug like dolutegravir or raltegravir.
Other Important Considerations
- Hepatitis B: Offer the hepatitis B vaccine if the patient is not immunized.
- Herpes (HSV): Prophylaxis is not routinely given. Treat with acyclovir or valacyclovir only if active lesions are present.
- Syphilis: Prophylactic treatment is not standard. A baseline RPR test should be drawn.
- Follow-Up Testing: Patients require follow-up testing for HIV and RPR (syphilis) at 4 to 6 weeks, 3 months, and 6 months.
- Trauma-Informed Care: It is critical to make patients feel safe, state that you believe them, and affirm that the assault was not their fault.
- Sexual Assault Nurse Examiner (SANE) Programs:SANE programs provide specialized, trained nurses to conduct detailed forensic exams, which can take 4-5 hours and are crucial for legal proceedings.
Sickle Cell Disease + Acute Pain
Anand Swaminathan, MD, and Jeff Glassberg, MD
Swami and Dr. Glassberg cover management strategies for acute and chronic pain in patients with sickle cell disease (SCD).
Treatment of Pain in SCD
- General:
- Make an effort to differentiate between acute vaso-occlusive crisis pain and chronic pain exacerbation.
- Always believe the patient’s story and expression of pain but consider providing follow-up if concerned for a chronic pain component.
- Make an effort to differentiate between acute vaso-occlusive crisis pain and chronic pain exacerbation.
- Look at the patient’s pattern of utilization.
- More than 2 or 3 visits for pain per year increases suspicion for chronic pain.
- Refer patients to care coordination teams such as case managers and social work.
- No objective data are available to differentiate the two presentations.
- Determine whether there may be other medical explanations for new acute pain presentation to the ED:
- Bone infarct, acute chest syndrome, depression, etc
- Are intravenous (IV) fluids indicated for all SCD patients with acute pain without other indications of dehydration?
- Focus on gentle hydration; use hypotonic fluid
- Weak evidence that hypotonic fluids will enter red cells and hydrate them
- One liter of ½ normal saline over 4 hours
- Focus on gentle hydration; use hypotonic fluid
- Is supplemental oxygen recommended for acute pain crises even with normal saturations?
- No, supplemental oxygen is not recommended if the patient is not hypoxic.
- Hyperoxia can be dangerous.
- Some patients request IV diphenhydramine (Benadryl) with each dose of opiates due to the itching associated with these medications. Is IV diphenhydramine indicated with every dose of opiates for itching?
- Dosing of diphenhydramine is every 6 to 8 hours.
- IV diphenhydramine with opiates can give patients a euphoric sensation.
- Avoid giving medications that can cause euphoria sensations.
- This can create inappropriate narcotic cues.
- Use oral diphenhydramine rather than IV diphenhydramine.
- Only use IV diphenhydramine when patients cannot tolerate oral dosing.
- Swami recommends an established protocol within departments to avoid variation in provider prescribing.
- Dosing of diphenhydramine is every 6 to 8 hours.
- Are adjunctive medications for pain helpful for vaso-occlusive crisis?
- Yes, use acetaminophen (Tylenol) and nonsteroidal anti-inflammatory drugs (NSAIDs) in addition to opiates.
- Should patients receive IV opiates immediately upon presentation to the ED?
- Some patients have access to oral opiates at home, but some do not.
- Don’t be surprised if patients do not have access to opiates at home.
- Starting with oral opiates may waste time; start with parenteral opiates to get ahead of a patient’s pain.
- Make sure to take into account tolerance to opioids before ordering IV opiates:
- Eg, Every 1 mg of oxycodone is the same as 0.5 mg of IV morphine.
- Convert home dosing to determine optimal dosing of IV opiates.
- Some patients have access to oral opiates at home, but some do not.
- If giving parenteral opiates and there is no improvement, is there a role for ketamine or haloperidol to provide a synergistic effect with opiates?
- These can be beneficial.
- Consider whether the patient is extremely tolerant to opioids or whether there could be an institutional prescribing pattern that is not being addressed.
- Be a good steward of opiates in outpatients to avoid tolerance.
PEARLS:
- If a patient with SCD presents with pain, treat the pain with IV opiates. However, consider referrals if concerned about a chronic pain component.
- Use hypotonic IV fluids but focus on gentle hydration.
- Oxygen is not indicated if the patient is not hypoxemic.
- Diphenhydramine (Benadryl) can be used orally for itching but should not be dosed more frequently than every 4-6 hours.
- Use NSAIDs and acetaminophen with opiates as synergistic medications for pain crises.
- Start with parenteral opiates in the ED to manage pain quickly. Consider opiate tolerance and use conversions to ensure proper dosing of opiates.
NEJM
