Academic Emergency Medicine
Annals of Emergency Medicine
Outcomes of Older Adults With Delirium Discharged From the Emergency Department
- Delirium also know as acute (hours to days) confusional state defined in the study as a positive bCAM screen.
- Overall, 1 in 12 (8.4%) patients with delirium will die within 30 days versus 1.5% of delirium negative discharged patients.
- Delirium positive patients who were discharged had a 32.2% ED return rate versus 19.9% for those without delirium.
- Hospital admission is frequently the default management strategy for ED patients with delirium, however admission may not always benefit patients with delirium.
Comparison of Preoxygenation Strategies for Intubation of Critically Ill Patients
EMCRIT
EMCrit 413 – Translating Recent Sepsis Papers to the Bedside with PulmCrit (Farkas)
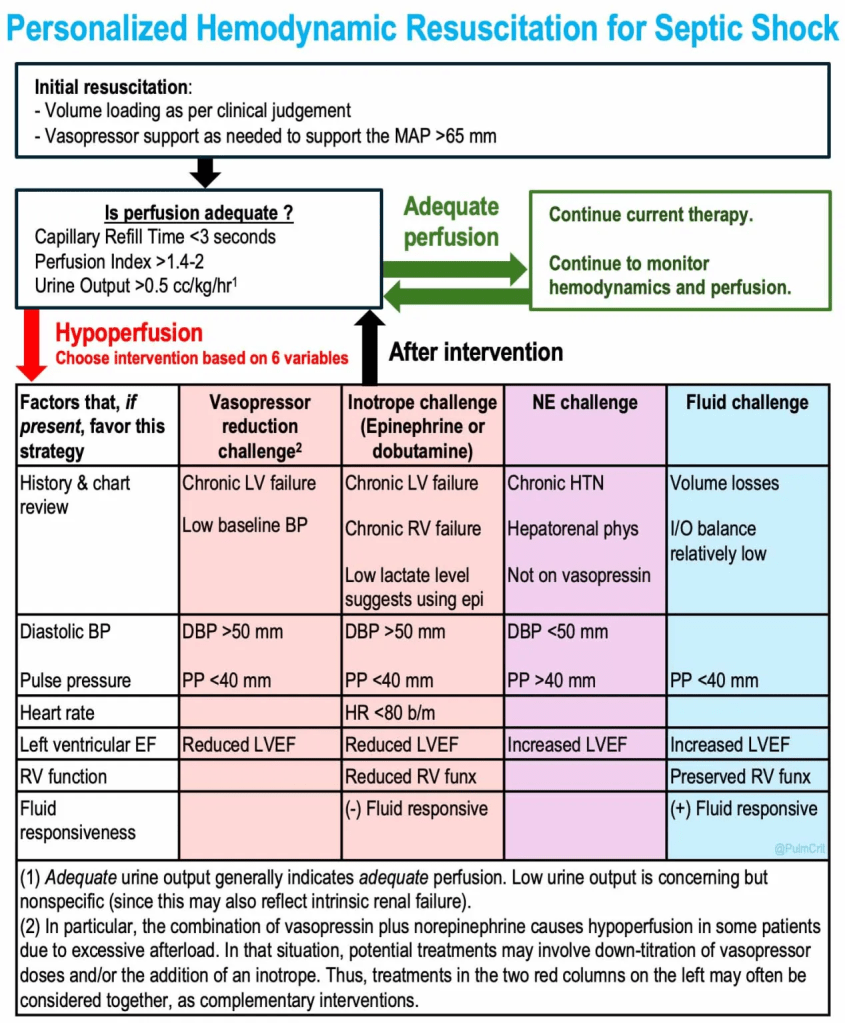
- The new sepsis trials are trying to move beyond BP and lactic acid to guide whether a patient is optimized with fluids and pressors to achieve adequate perfusion.
- Their recommendation is to follow capillary refill time, goal ❤ seconds.
- Farkas recommends adding perfusion index which apparently is generated on pulse ox machines (never heard of it!) and urine output.
EMRAP
Case of the Week
Mizuho Morrison, DO, and Anand Swaminathan, MD
Case
- A 45-year-old woman with a history of lupus with shock
- Past medical history includes lupus, hip replacement the day before for avascular necrosis, Sjögren syndrome
- Vitals: Heart rate in 130s, systolic in 70s, afebrile
- Home medications: prednisone 5 mg for over 15 years, held nonsteroidal anti-inflammatory drugs (NSAIDs) prior to her surgery
Differential diagnosis for persistent hypotension in this case:
- Sepsis
- Hemorrhagic shock
- Obstructive pulmonary embolism (early, but possible)
- Adrenal crisis
Initial management:
- Fluids
- Antibiotics
- Ultrasound of hip, looking for hematoma/bleed
- Physical exam (evaluate the hip and surgical site)
- Panculture
- Vasopressors if needed
Physical exam:
- No large hematoma of the hip
- No erythema, edema, warmth, or drainage of surgical site
Case outcome:
- Despite fluid resuscitation, the patient was still hypotensive to the 70s and tachycardic to the 110s.
- Hemoglobin was normal.
- Adrenal crisis was moved higher on the differential due to persistent refractory shock.
- The patient received hydrocortisone sodium succinate (Solu-Cortef) prior to the surgery.
- The patient received steroids and was admitted to ICU.
Takeaways:
- Adrenal crisis patients likely will not respond to vasopressors.
- No laboratory test will come back in time to diagnose adrenal crisis; it is a clinical diagnosis.
- If a patient is on chronic steroids and is sick, they need stress-dose steroids, even in the absence of infection.
- Treat adrenal crisis with 100 mg of hydrocortisone intravenous push.
PEARL: For patients in refractory shock, consider adrenal insufficiency and stress-dose steroids.
EMA 2025 October Abstract 5: PENG Block vs Fascia Iliaca for Hip Fracture Pain Management
EMA EDITOR’S COMMENTARY: In this small but well-done trial, the PENG block had superior efficacy to the more traditional fascia iliaca block in decreasing pain in older ED patients with hip fractures. This finding, combined with the theoretical advantage of avoiding quadriceps motor blockade, suggests that the PENG block merits serious consideration as emergency providers expand their regional anesthesia capabilities, particularly as specialized training programs begin to incorporate PENG blocks into their curricula.
Critical Care Mailbag: Status Epilepticus Update
Anand Swaminathan, MD, and Scott Weingart, MD
Summary: The team discusses updates as well as helpful pearls when managing status epilepticus.
The seizing patient:
- In general, there is no need to give high-dose benzodiazepines to patients with seizures lasting less than 5 minutes, especially if it is a first seizure or there is low concern for status epilepticus.
- Most of these seizures self-terminate.
Concern for status epilepticus:
- Current guidelines suggest first-line IV lorazepam or IV diazepam or IM midazolam.
- IV midazolam is likely faster than IV lorazepam but it doesn’t last as long.
- Consider IV midazolam (5-10 mg) first for active seizure and then IV lorazepam after the patient wakes up.
- If the first dose of IV midazolam is ineffective, give a second dose a few minutes later.
- Consider using an adjunct of ketamine when giving the second dose of IV midazolam.
- You should see results within the first couple of minutes of administration. If the patient is still convulsing, consider intubation and propofol infusion in the ED.
- Once it is determined that the patient may be in status epilepticus, give levetiracetam load of 60 mg/kg up to 4.5 g; however, this agent is unlikely to terminate status epilepticus.
- 20 mg/kg of phenobarbital can also be used as the third line; however, if approaching this point, strongly consider ketamine and intubation.
- If no contraindication, use succinylcholine for rapid sequence intubation to preserve neuro exam and determine if the patient is still in status after intubation.
- Use high-dose sedation propofol (start 50-100 μg/kg/minute) after intubation and have norepinephrine at bedside for resultant hypotension.
PEARL: Consider early intubation and aggressive treatment of status epilepticus.
References:
Combined ketamine and midazolam versus midazolam alone for initial treatment of pediatric generalized convulsive status epilepticus (Ket-Mid Study): a randomized controlled trial
Othman AA, Sadek AA, Ahmed EA, et al. Pediatr Neurol. 2025;167:24-32. doi: 10.1016/j.pediatrneurol.2025.03.011. PMID: 40186980
A comparison of parenteral phenobarbital vs. parenteral phenytoin as second-line management for pediatric convulsive status epilepticus in a resource-limited setting
Burman RJ, Ackermann S, Shapson-Coe A, et al. Front Neurol. 2019;10:506. doi: 10.3389/fneur.2019.00506. PMID: 31156538
Mechanical Ventilation in Obesity
Anand Swaminathan, MD, and Steve Haywood, MD
Summary: Dr. Swaminathan sits down with Dr. Haywood to discuss nuances in the mechanical ventilation of the obese patient. It is important to consider that obese patients have chronic lung hypoxia, excess visceral adipose tissue, and decreased chest compliance, given their excess tissues and weight, etc.
Positioning:
- Laying the obese patient flat improves chest wall compliance, among other mechanics.
- Lying flat increases the risk of ventilator associated pneumonia (VAP), thus reverse Trendelenburg (head up, feet down) helps combat this.
- Try to keep the patient’s head above their feet.
Ventilator settings:
- Treat every obese patient as if they have acute respiratory distress syndrome (ARDS) with a lung protective strategy of ~6 mL/kg of ideal body weight.
- Take time to measure your patient’s height to determine ideal body weight.
- Do not be afraid to use positive end-expiratory pressure (PEEP). Obese patients have more external pressure and soft tissues pushing up on the diaphragm that can be counteracted by PEEP.
- Decremental PEEP titration is a useful tool in obese patients. Consider starting at 25-30 cm H2O and decrease by 2-3 cm H2O every 5-20 minutes, checking compliance each time.
- Aim for oxygen saturation (SaO2) of 94%-98%.
Transgender Care in the ED Part 1
Jan Shoenberger, MD, and Jailyn Avila, MD
- Cisgender: a person who is the same gender that they were assigned at birth
- Transgender: a person who is a different gender than they were assigned at birth
- Cis and trans: adjectives describing a person’s gender (eg, transwoman)
- Non-binary: a person who does not identify as a man or woman, typically using “they/them” as their preferred pronouns
Best practices for initial interactions:
- “I’m Dr. X, my pronouns are he/him (she/her, etc), what pronouns may I use to refer to you?”
- If you mess up, apologize, correct yourself, and move on.
- “May I share your preferred name/pronouns with the staff and/or registration?”
- Pins or badges highlighting your pronouns can greatly help trans patients feel more comfortable and trusting of the healthcare system.
Medications/hormones used by trans individuals:
5-alpha reductase inhibitors (eg, dutasteride, finasteride) are used to block testosterone.
- May cause orthostatic hypotension
Spironolactone is used at high doses (100-300 mg/day) to block testosterone and for its estrogenic effects.
- May cause orthostatic hypotension and potassium derangements, particularly when initiated
Estrogen can be taken orally, topically, or parenterally.
- Oral estrogen increases the absolute risk of venous thromboembolism (VTE) 2-fold but overall risk remains less than 1%.
Testosterone: high doses will also block estrogen and will lead to voice changes by thickening the vocal cords.
- Places the patient at the same risk for cardiovascular complications as a cisgender man
- Can increase hemoglobin and blood viscosity
PEARL: Medications and hormones are often vitally important to trans individuals. It is helpful to recognize the potential side effects or risks they may face and work with them to mitigate these effects.
Transgender Care in the ED Part 2
Jan Shoenberger, MD, and Jailyn Avila, MD
Gender-Affirming Surgeries:
- Vocal cord tightening/shortening: This may limit the size of endotracheal tube (ETT) that can be used for intubation; consider sizing down.
- Cricoid/thyroid approximation: This may obliterate the cricoid membrane, limiting the ability to perform a surgical airway in an emergency.
- Top surgery (breast reduction or augmentation): Watch for standard post-surgical complications.
- Metoidioplasty: Enlarges the clitoris and releases it to create a phallus to allow for urinating standing up. This may limit the ability to catheterize for urine.
- Phalloplasty: Creating a neopenis from skin grafts. Use of a foley catheter may be contraindicated and the patient may require suprapubic catheterization after discussion with urology.
- Vaginoplasty: Inversion of the penile shaft and scrotum, which may be prone to surgical complications like fistulas.
Non-Surgical
- Binding: using elastic binders to reduce the appearance of breasts
- The binder may place the patient at increased risk of hypoxia or difficult ventilation during procedural sedation. You may need to discuss temporarily removing the binder beforehand.
- Tucking: using special underwear or tape to minimize the appearance of the penis and testicles.
- Early on, this may place the patient at an increased risk of testicular torsion.
Surgical history
- Surgical history should be obtained when it is clinically relevant and not because of curiosity. Explain to your patients why asking about specific surgeries is clinically relevant for their condition or symptoms.
Mental Health
- Gender dysphoria: Distress caused when an individual’s gender does not align with their gender assigned at birth.
- The inability to transition and treat gender dysphoria can create significant mental and emotional distress and higher rates of suicide.
- Trans people unfortunately see higher rates of violence and trauma.
Allies can help with their colleague’s transition in the workplace and support them by encouraging the use of appropriate pronouns with your colleagues.
PEARLS: Trans patients may have slightly different medical risks based on their prior medications and surgeries; however, the first step in providing excellent care is to be supportive and create an environment that they can trust and be open in.
EMA 2025 October Abstract 16: Atropine Versus Placebo for Neonatal Nonemergent Intubation
EMA EDITOR’S COMMENTARY: This very small RCT compared atropine vs placebo for intubating very premature neonates. The findings were mixed. Atropine decreased the incidence and duration of bradycardia, but the absolute number of events was small, and hypoxemia paradoxically occurred more often in the atropine group. Overall, this study does not provide compelling evidence supporting routine atropine use.
Pacemakers + AICDs
Anand Swaminathan, MD, and Tarlan Hedayati, MD
Summary: Dr. Swaminathan and Dr. Tarlan Hedayati discuss stepwise approaches to caring for patients with pacemakers and automated implantable cardioverter-defibrillators (AICDs) in the ED.
Interrogation of a pacemaker in the ED
- Interrogate if the chief complaint is seemingly related to pacemaker malfunction. This would include symptoms such as pre/syncope, chest pain, SOB, palpitations, etc.
- Obtaining a 12-lead ECG gives you a snapshot of that moment in time but interrogation provides a retrospective look at what was happening when the patient was symptomatic.
Pacemaker malfunction with symptomatic bradycardia or hypotension
- If the patient is pacemaker dependent and bradycardic, the problem could be secondary to oversensing. Place a magnet on the device as a first-line attempt.
- If the magnet doesn’t work, this is a failure to pace. Move toward transcutaneous pacing with anterior-posterior (AP) positioning of pads.
- Set rate around 60 BPM or higher and start around 60 mA. Confirm capture (echo, pulse, pulse ox, etc).
- Maximum transcutaneous output is around 140 mA. If approaching this, strongly consider transvenous pacing.
- Prefer right internal jugular (RIJ) for transvenous pacer placement. If the RIJ is not an option, choose the right femoral.
AICD
- Maintain a broad differential and perform a standard workup.
- The patient might not feel a shock when the device gets them out of an unusual rhythm.
- Syncope with AICD:
- Perform syncope workup as indicated and evaluate for causes unrelated to AICD.
- If there is no clear reason for a syncopal event from workup, you may need to interrogate the AICD.
- A single shock does not mean the patient requires admission; however, evaluate for ischemic causes of arrhythmia. A rising troponin indicates that a patient should be admitted.
- Multiple shocks require ED interrogation and admission. Also consider antiarrhythmics to help terminate abnormal rhythms.
PEARL: You can pace the patient via other means if the pacemaker is malfunctioning. Keep a broad differential and thoroughly evaluate patients who experience a discharge from their AICD.
NEJM
Medicaid Cuts and U.S. Children’s Health — Fixing a Broken System
Opioid Deprescribing in Patients with Noncancer Pain
Deferring Arterial Catheterization in Critically Ill Patients with Shock
- Among patients with shock, results for death from any cause at day 28 indicated that management without early arterial catheter insertion was noninferior to early catheter insertion.
REBELEM
REBEL Core Cast 144.0: Tourniquet Tips
- Tourniquets save lives and limbs: Apply immediately when you’ve got arterial bleeding.
- Placement matters: Position the tourniquet 5–6 cm proximal to the arterial bleed, or if you can’t identify the exact source, place it as high up on the limb as possible.
- Windlass technique: The windlass provides only a small amount of extra pressure. Tighten the velcro first, then twist the windlass 1–2 turns to complete compression.
MDCalc Wars: Winter is Coming: Are You Using the Right Pneumonia Score?
- PSI/PORT: In-depth and data-heavy — best for mortality risk and disposition decisions, but may miss early deterioration.
