Academic Emergency Medicine
Pitfalls of Posterior Leads for Posterior Occlusion MI
- Posterior leads can be misleading and do not have better sensitivity than ST depressions in V1-4 on a traditional lead placement.
Intravenous Thrombolysis for Minor Acute Ischemic Stroke
- Harms outweigh benefits in minor strokes (NIHSS </=5)
Annals of Emergency Medicine
Cool Running Water as a First Aid Treatment for Burn Injuries
- Running cool water over burned area for 20 minutes within 3 hours is recommended.
EMCRIT
EMCrit 416 – JanuAIRWAY – State of the Airway 2026
Awake?
- Anatomic Difficulty: Obstruction, Prior Difficult Airway, Difficult airway (MACOCHA), Open mouth move neck, upper lip test
- Hypotension (NEVER PARALYZE: PE, severe aortic stenosis, pericardial tamponade, right heart failure)
- Oxygenation
- pH
Always Have Triple SetUp
- Video
- Disposable bronch
- Cric
Positioning
- Earholes above sternal line (not notch!) xiphoid to manubrium
- As close as possible Face plane parallel to ceiling
Greenland on Positioning
1st step: head lift or flex lower Cx spine to flatten secondary curve (red curve):
A. obese patient: ~7cm head elevation – poor positioning (at least C&L Gr 3)
B. obese adult: 1x pillow under shoulders & 2x pillows (or equiv) under head = “ramped” or
C. head of bed elevated so ext meatus level with sternal notch
D. adult: normal pillow (~7 cm height)
E. child: small pillow
2nd step: ext upper Cx spine to flatten primary curve (green curve)
Preoxygenation-
- NC at 15L and NIV mask with straps and BVM with peep valve 5 (PreOxi trial) or 10 (Weingart study unless hemodynamic instability).
- After pushing meds disconnect straps do jaw thrust with 2 hands on mask give 6 breaths per minute during apnea and before complete relaxation
Bag During Apnea
- Unless massive SBO or stomach full of blood and you didn’t preemptively drain the blood.
Induction
- Induction Etomidate for RSI (less hypotension) and
- Ketamine .5-1mg/kg for DSI
Paralytics
- Roc or Sux
Laryngoscope
- Standard Geometry with video and bougie best for teaching
ETT Size
- ETT size 7 for women and 7.5 for men
Tube Confirmation
• • Tube confirmation 2 point (1 visual and 2 CO2 rising for 7 breaths after intubation)
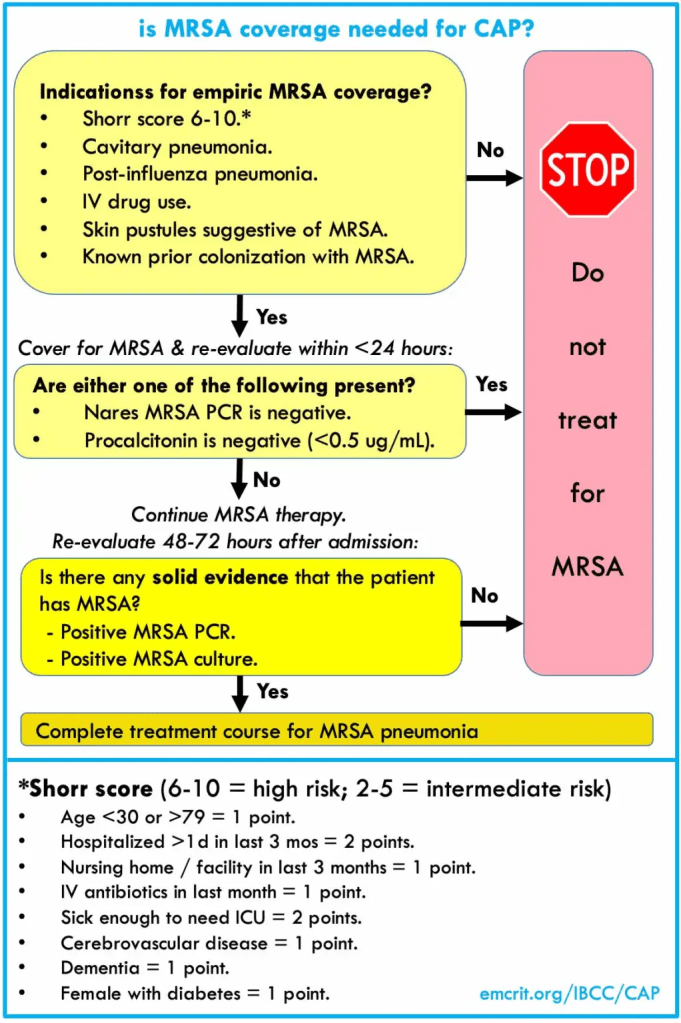
EMCrit 417 – The Antibiotics Show – Community Edition with David Talan
Septic shock early abx make a difference, otherwise not so much
Workup: low threshold for ct chest abdomen pelvis for super sick patients or patients without a source
Antibiotics:
- Renal Dosing: First dose always normal, only follow-up doses are renal adjusted
- UTI
- When to cover ESBL?
- Blood or urine culture with resistant organism in the past 12 months
- Exposure to third-gen cephalosporin or quinolone in last 3 months
- Septic shock patients
Recommendations:
Most patients: Ceftriaxone 2g IV Q24hrs
If possible ESBL or really sick: Meropenem 2g IV then 1-2g IV Q8
2. Abdominal/GI
Piperacillin-Tazobactum 4.5g IV Q8 (given over 4 hours)
If at risk of ESBL:
Meropenem 2g IV then 1-2g IV Q8
3. Lung
Ceftriaxone 2G IV Q24 plus Azithromycin 500 mg IV Q24 or Doxycycline 200 mg PO/IV then 100 mg PO/IV Q12
Atypical Workup
Legionella urine antigen is universally sent, but sputum PCR is probably better
Do they need pseudomonal coverage?
- DRIP Score [10.1128/aac.03071-15
- P. aeruginosa isolated from respiratory cultures within the last year
- Recent Antibiotic Use (last 30-60 days; some say only IV count)
- Hospitalization in the last 60-90 days (some would say only if you got antibiotics)
- Neutropenic
- Solid Organ transplant <1 yr or treatment for rejection
- Stem cell transplant <1 year
If so,
change Ceftriaxone to Cefepime 2g IV Q8
MRSA
Do they need anaerobic coverage?
No, not for aspiration
Only for actual structural pathology: empyema, necrotizing pneumonia, lung abscess
[Stanford Bugs&Drugs Recs]
Do they need Steroids?
If going to ICU:
Hydrocortisone 50 mg IV Q6
4. Skin Necrotizing STI
- Piperacillin-Tazobactam 4.5g IV Q8 (given over 4 hours) or Meropenem 1 gm Q8
- Linezolid 600 mg IV q12h (or vanco)
- Clindamycin 900 mg IV Q8
5. CNS (Meningitis/Enecephalitis)
- Ceftriaxone 2g IV Q12
- Vanco or Linezolid- Resistant S Pneumo
- Ampicillin (Probably not necessary if on Linezolid)- Listeria If >50 or ETOH
- Dexamethasone 10 mg IV Q6 for all adults with bacterial meningitis
- not for neonates
- not for viral meningitis
- discontinue steroids if listeria grows out
6. Empiric Antibiotics (Source Not Yet Found)
- Low clinical suspicion, low severity of illness- Ceftriaxone 2g IV Q24
- High severity of illness- Meropenem 1g IV Q8h and Vanco
- Get CT Chest Abdomen Pelvis
EMRAP
Risk Management: Commonly Missed Pediatric Emergencies
Mike Weinstock, MD, and Ilene Claudius, MD
Ilene joins Mike to discuss how to pick up on diagnoses that are commonly missed in the pediatric ED.
Testicular torsion:
- 31% of torsion cases present as abdominal pain, not testicular pain.
- If there is testicular pain, lean toward obtaining an ultrasound.
- If there is a high level of concern, contact urology immediately.
- Aim to diagnose in <6 hours (97% salvage rate).
Appendicitis:
- One study demonstrated that two-thirds of appendicitis medical malpractice cases were from delay in diagnosis.
- You are more likely to miss the diagnosis when there’s concomitant constipation.
- Urinalysis can be abnormal in appendicitis.
- Shared decision-making and good discharge instructions are important.
- In kids ❤ years old, 70% will perforate within 48 hours from symptom onset.
- Have parents observe at home and perform serial exams.
Meningitis:
- Determine if there is an alternative diagnosis (eg, fever and headache commonly seen in upper respiratory infection).
- If the patient is confused or can’t remember simple things, this is concerning.
- Other concerning signs to look for include petechial/purpuric rash, poor capillary refill, confusion or change in behavior, and lack of an alternative diagnosis.
Fractures:
- Trauma and pain in a specific bone? Have a low threshold to x-ray.
- Slipped capital femoral epiphysis (SCFE) may not present as hip pain.
- X-ray may be negative initially, so it is better to treat as fracture if uncertain.
Pediatric Round Table: BRUE
Ilene Claudius, MD; Jeff Seiden, MD; and Al Sacchetti, MD
Definition and Criteria: A brief resolved unexplained event (BRUE) is defined in infants less than 1 year old where:
- Symptoms have resolved before the infant arrives at the ED;
- The event remains unexplained after a history and physical examination;
- The event includes at least one of these features:
- Cyanosis or pallor
- Absent, decreased, or irregular breathing
- Marked change in tone (hypertonia or hypotonia)
- Altered level of responsiveness
Lower Risk Features (must meet all)
- Age >60 days
- No history of prematurity <32 weeks or a current post-conceptual age >45 weeks
- This is the first and only BRUE
- The event lasted <1 minute
- No cardiopulmonary resuscitation was performed by a trained medical provider
Evaluation:
- Assess the family history for sudden death, long QT syndrome, or other congenital arrhythmias.
- Evaluate how comfortable the family is with caring for their newborn, especially following this event.
- During evaluation, keep the infant on pulse oximetry to monitor for similar or recurrent events.
- An ECG and pertussis screening may be helpful.
- A viral panel is likely of low utility due to the potential for false positives.
Risk Stratification and Management
- Patients who do not meet low-risk criteria should be admitted and monitored inpatient.
- If a patient has a prescribed apnea monitor at home, they may be at higher risk and warrant admission, where they should be monitored on both the hospital monitor and their own apnea monitor.
- If the patient is not admitted, ED observation for 1 to 2 hours should include a monitored feeding.
PEARL: The current BRUE guidelines help define low-risk patients; however, management and the decision to admit or observe is heavily affected by the specifics of the event and the comfort level of the family.
Critical Care Mailbag: Hodgepodge
Anand Swaminathan, MD, and Scott Weingart, MD
Drs. Swaminathan and Weingart discuss a variety of critical care topics, including post-intubation sedation, vasopressin in organ donation, methylene blue in shock, peri-arrest intramuscular (IM) epinephrine, and albumin in sepsis.
1. Post-intubation sedation
- Prioritize a sedation and analgesia plan when going through your airway checklist to minimize delay following intubation.
- Be prepared with vasopressors for sedation-related hypotension.
2. Vasopressin in organ donation
- For a patient with brain death, discuss with the organ procurement organization before initiating hormone replacement therapy.
- Hemodynamic stability takes precedence; if vasopressin is needed, use it.
- Consider vasopressin as the first-choice pressor in patients with brain death.
- May start vasopressin at 0.01 or 0.02 units/minute and titrate to hemodynamic effect.
- Most states do not want ED practitioners to discuss organ donation with families. If you don’t have training in discussion of organ donation and your state doesn’t explicitly encourage you to initiate the conversation, don’t do it.
- Contact the area’s designated Organ Procurement Organization (OPO) to begin the coordination process. The OPO will offer preliminary consultation and provide an expedited on-site response to assist with the transition of care.
3. Methylene blue in shock
- There are no major data supporting the use of methylene blue in severe shock or vasoplegia at this time.
- You may notice a transient elevation of blood pressure with no measurable lasting effect.
- If shock is refractory to high doses of multiple pressors and steroids, you can consider methylene blue; however, there are no supportive data and this is uncharted territory.
4. IM Epinephrine in peri-arrest patient
- This should be reserved for low-resource settings where you don’t have access to intravenous (IV) or intraosseous (IO) access, which is not generally the case in an ED.
- If you have IV or IO access, give 0.5 mL (50 μg) of cardiac epinephrine (code cart epi) for peri-arrest patients.
- Start with a lower IV dose (10-20 μg) for patients with severe asthma who require epinephrine.
5. Albumin in sepsis
- Cirrhotic patients may benefit from albumin resuscitation.
- Albumin does show benefit in spontaneous bacterial peritonitis (SBP) and large-volume paracentesis.
- Albumin is generally safe but has no data showing benefit in the general population.
- Stick with crystalloid empirically.
PEARL:
- Verbalize your post-intubation sedation/analgesia plan to the room before intubation and have the drugs ready at bedside. Also be prepared for post-intubation hypotension.
- Discuss with the organ procurement organization early when you have a patient with brain death.
- Methylene blue has no strong supporting evidence for use in shock at this time.
- In peri-arrest patients, you can use IM epi; however, use small doses from code cart epi as push-dose pressors.
- Albumin should not be the first-line resuscitation fluid in the general population.
References:
A comparison of albumin and saline for fluid resuscitation in the intensive care unit
Finfer S, Bellomo R, Boyce N, et al. N Engl J Med. 2004;350(22):2247-2256. doi: 10.1056/NEJMoa040232.
First10 EM
Unfortunately the
Byrne A, Macdonald DB, Kirkpatrick IDC, Pham M, Green CR, Copaescu AM, McInnes MDF, Ling L, Ellis A, Costa AF.CAR/CSACI Practice Guidance for Contrast Media Hypersensitivity. Can Assoc Radiol J. 2025 Aug;76(3):400-416. doi: 10.1177/08465371241311253. Epub 2025 Jan 11. PMID: 39797723
The recommendations
1: Documenting
“The dose and precise name of any contrast media must be documented in the patient’s electronic health record, such that it can be easily retrieved in the event of an acute or delayed hypersensitivity reaction. If a patient experiences an acute contrast agent hypersensitivity reaction, the precise name of the offending contrast should also be documented in the patient’s radiology report, which is sent to the referring provider and stored on PACS. The onset and nature of the reaction as well as treatment should also be documented. Ideally, a reporting mechanism should also be in place for delayed hypersensitivity reactions.”
Comment: No argument here. Don’t just say “contrast allergy.” That is sort of like saying “antibiotic allergy”. Be specific.
2: Allergies are to a specific contrast agent, not general
“Patients (adults and pediatric populations) should only be considered at risk for a hypersensitivity reaction if they had a previous hypersensitivity reaction to the same type of contrast agent. That is, HR to LOCM ICM is a risk factor for future HR to LOCM ICM, and HR to GBCA is a risk factor for future HR to GBCA. There is insufficient evidence to support routine screening of other risk factors. It is important to distinguish between a true hypersensitivity reaction and a physiological reaction.”
Comment: Again, this is very good advice. This is becoming less of an issue, as most places have been using low osmolar agents for a long time, but there is a big difference between low and high osmalar CT contrasts. It is also important to actually make a diagnosis. Too many documented “allergies” have no symptoms of allergy. (This is a broader issue in medicine. I get flagged all the time that a patient is allergic to morphine because it made them nauseous or constipated in the past. Please stop. Allergy means something medically. Let’s use the word correctly.)
3: The best protective measure is to use a different agent
“For patients with a history of a mild, moderate, or severe hypersensitivity reaction to ICM or GBCA, switching to a chemically different contrast agent is the single best protective measure to avoid a breakthrough reaction (Figure 1). For patients with a history of mild or moderate breakthrough reaction after contrast switching, a third agent should be administered. Contrast switching requires institutions and health authorities to have at least 2 different contrast agents. Single vendor contracts should allow for purchasing a second agent for this purpose.”
Comment: Unfortunately, financial conflicts of interest are rampant in hospital purchasing departments. Contracts often prevent you from buying from other companies. I have never worked in a hospital with multiple contrast types available (as far as I know), but the primary responsibility for preventing allergic reactions lies with the radiologist ordering the contrast material, not with the emergency department (because as we will see in a second, we need to abandon our current ridiculous pretreatment strategies.)
4: You can infer the prior CT contrast agent based on year
“For patients with a history of HR to ICM but the offending agent is not known, management is based on the date of the reaction (Figure 2):
- If the reaction occurred before the year 2000, it can be reasonably assumed that the offending agent was not a low-osmolality contrast media (LOCM) agent, and the patient is then cleared to be administered LOCM administered without premedication.
- If the reaction occurred on or after the year 2000, and the reaction was severe (acute or delayed), consider another imaging modality to answer the clinical question. Consider referral to an allergist if access and urgency of imaging allows. Premedication is not recommended.
- If the reaction occurred on or after the year 2000, and the reaction was mild or moderate, consider premedicating with second generation antihistamines and monitoring the patient during and immediately after contrast media injection for any hypersensitivity reaction.”
Comment: The middle point will be difficult for emergency departments. Allergist referral is never going to be realistic, and we rarely have access to reasonable alternatives. (Sometimes an MRI would adequately answer the question we are asking on CT, but that would require having urgent access to an MRI.)
5: Steroids are out
“In patients with a history of hypersensitivity reaction to LOCM iodinated contrast media, premedication with steroids is not supported by high quality research. What evidence exists is methodologically flawed and pertains to HOCM. Due to lack of efficacy and likely harms associated with steroid pretreatment prophylaxis, the working group recommends against routine use of steroids in high-risk patients. This practice should be discontinued.” (Emphasis added.)
Comment: We have known this for a long time. It is incredibly nice to see this laid out clearly in guideline format. There is really no evidence that steroids change anything except for minor rashes after contrast, but these authors are optimistic, and suggest that steroids might be a number needed to treat of 56,900 to prevent one death and an NNT of 569 to prevent one severe reaction. That might be fine if these steroid protocols were harm free, but in addition to the massive increases in length of stay (25 hours on average), steroids also have other side effects, such as infection. Given the NNT of 56,900, they estimate that in order to save on life from an allergic reaction you will end up causing 551 hospital acquired infections and 32 infection related deaths. We do this a lot in medicine. We become so myopic on a topic (in this case, trying to prevent allergic reactions at all cost), that we lose track of the bigger picture. This is the section of the paper that needs to be shared far and wide. The best evidence, as agreed on by the radiologists and allergists, is that steroid pretreatment protocols are killing patients. Harms outweigh benefits. This needs to stop now.
6: Steroids are also out for gadolinium
“In patients with a history of hypersensitivity reaction to gadolinium-based contrast agents, premedication with steroids is not recommended. The evidence supporting steroid premedication to prevent a breakthrough reaction is mixed, but overall shows little benefit, with risk of potential harm.”
Comment: Probably not very relevant to most emergency department practices (although I did recently see a doctor successfully advocate for his pregnant patient with an equivocal ultrasound to get an MRI rule out appendicitis, so I guess you never know).
7: Antihistamines might prevent a bit of itching
“Second-generation antihistamines can protect patients with history of mild hypersensitivity reaction from a breakthrough reaction. The added benefit of antihistamine after contrast switching is less clear and can be considered optional. Ideally, oral second-generation antihistamines should be given at least 1 hour prior to initiation of contrast.”
Comment: I haven’t had time to dig deeply into this literature, and given how minor an issue it is to give an anti-histamine I doubt I ever will. That being said, I would never delay a critical STAT scan by an hour just to give the antihistamine time to work.
8 and 9: I am skipping
Basically, there is no reason to pick one specific CT contrast agent or gadolinium agent. Doesn’t really matter to us in emergency medicine.
10: For anaphylaxis, consider alternative tests. If there isn’t one, use a different agent and proceed.
“For patients with a history of anaphylaxis to contrast media, the risk of a breakthrough reaction can be limited by switching to a different imaging modality, if diagnostically acceptable. If not, switching to a different contrast agent is recommended. The patient should be monitored during and after the contrast media injection. Premedication is not recommended.”
Comment: This is basically a repeat of the above. The reminder to consider alternative testing is reasonable, as long as it doesn’t result in silly suggestions. (“I have this crashing patient that I think might have a PE… why don’t you order a VQ scan tomorrow?”) For emergency medicine, the key point of these guidelines is that if there is not a viable alternative, prior allergy is not a reason to avoid or delay a test. Just proceed, and monitor the patient appropriately.
11: Collect serum tryptase?
“For patients who experience an anaphylaxis reaction, once the patient has stabilized, collection of serum tryptase may help to determine if the reaction was an immediate hypersensitivity reaction. Serum tryptase should be collected 30 to 120 minutes after the onset of symptoms. Consider referring to allergy, when possible.”
Comment: I don’t know that this needs to be done routinely. Anaphylaxis is probably best left as a clinical diagnosis. Indeed, the few patients I have seen where I questioned the diagnosis, and have had negative serum tryptase levels come back, the allergists still suggest treating as if it was anaphylaxis, so I am not sure this test is helping anyone clinically. That being said, if the patient was already labelled as “allergic” in the chart, but has atypical symptoms, I suppose this might help you to remove that label. (Although, the label will be far less detrimental if we can get radiologists to follow these guidelines and do away with prolonged pretreatment regimens.)
12: Nonvascular contrast is the same
“For patients with a history of hypersensitivity reaction to nonvascular contrast, contrast switching without premedication is recommended for future administrations of non-vascular or vascular contrast. Adverse reactions to non-vascular contrast media are limited to case reports and small series. Based on a lack of evidence and overall rarity of these events, the expert consensus recommends against a pre-medication protocol.”
Comment: No real comment. Not sure how many of the patients I see generically labelled as “contrast allergy” were actually allergies to non-vascular contrast, but it sounds like it doesn’t matter, so I will continue to live in the dark.
13: Fasting is not required (obviously)
“It is recommended that patients not be instructed to fast prior to receiving intravascular contrast media, unless required for the specific imaging examination (eg, CT or MR enterography).”
Comment: Of course fasting is not required. In fact, I had never even known this was a radiology myth until recently. This had never been a thing in any of the hospitals I worked at in the past, but when trying to change our NPO culture at my current hospital, this myth was raised. It is a nice bonus that they addressed it here.
NEJM
Sudden Cardiac Arrest in Athletes
A Randomized Trial of Tenecteplase in Acute Central Retinal Artery Occlusion
REBELEM
MDCalc Wars: Alcohol Withdrawal–When CIWA-Ar Breaks Down, mMINDS Score Still Works
