Academic Emergency Medicine
- The Hunt and Hess Scale (HHS) assesses headache severity, neck stiffness, neurological deficits, and consciousness level, with higher scores correlating with increased mortality.7 However, its subjectivity and lack of clarity have drawn criticism.
- The World Federation of Neurological Surgeons Scale (WFNS), incorporating the Glasgow Coma Scale (GCS) and assessments for hemiparesis or aphasia, is more objective and has demonstrated stronger predictive capabilities.8
- ED-initiated oral naltrexone is feasible and acceptable for patients with moderate to severe AUD. While engagement in treatment was moderate, significant reductions in alcohol craving and improvements in quality of life suggest potential benefits. Further research is warranted to confirm these findings.
- California Bridge Program recommendations:
- Gabapentin 600-900 TID for alcohol withdrawal
- Naltrexone for Alcohol craving, NNT 9, 50mg PO QD, #14, avoid if concurrent opioid use or AST and ALT >5x normal
Annals of Emergency Medicine
Lidocaine as First-Line Treatment for Pulseless Ventricular Tachycardia and Ventricular Fibrillation
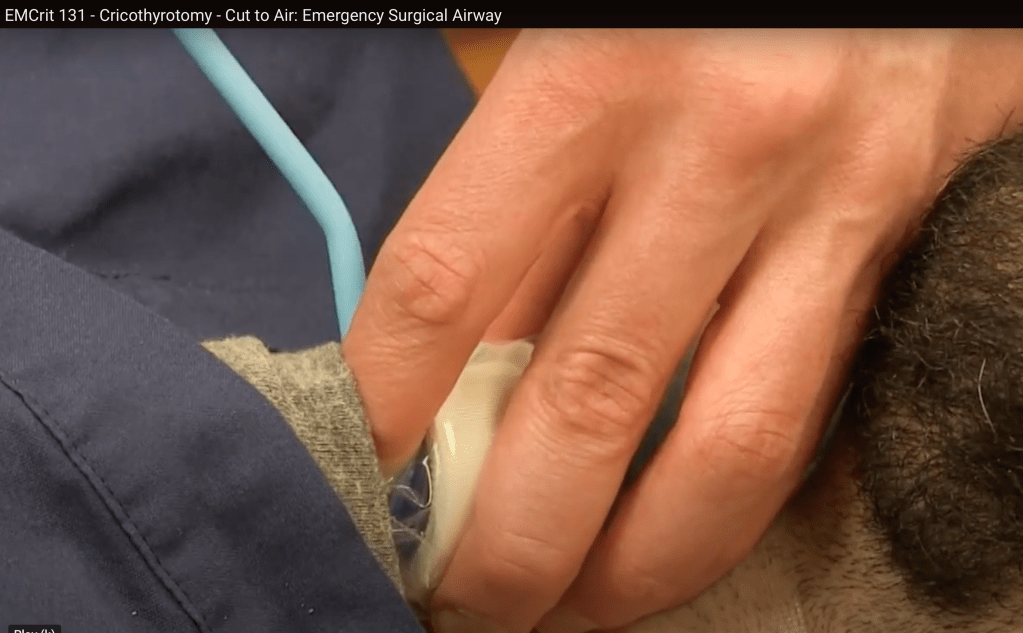
EMCRIT
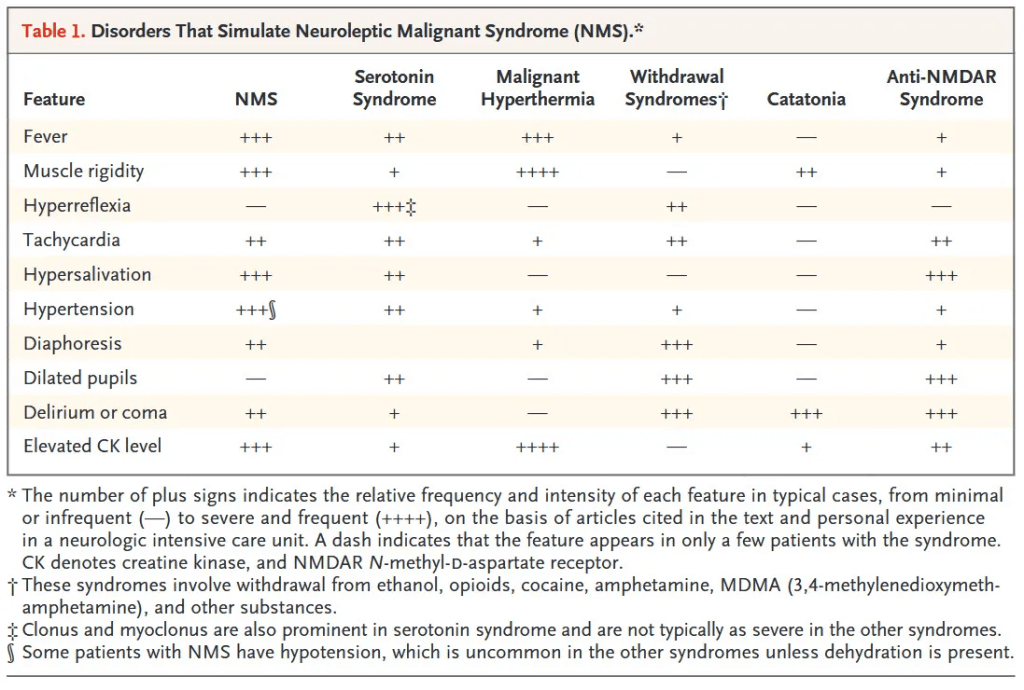
EMCrit Wee – Neuroleptic Malignant Syndrome (NMS) Explosion
- Rare
- Idiosyncratic
- Key symptoms
- High fever
- Severe muscle stiffness (rigidity)
- Confusion
- Autonomic instability
- NMS and SS do have similarities (hyperthermia, AMS, rigidity) but…
- Not hard to differentiate NMS from Serotonin Syndrome
- SS has marked hyperreflexia, clonus and myoclonus, NMS does not
- SS (when severe) has opsoclonus, random saccades of the eyes, NMS does not
- SS caused by an SSRI not antipsychotic
- SS much more common, NMS is rare
- NMS vs Catatonia
- Very difficult to distinguish
- Initially just hold antipsychotics
- Treatment
- Intubate when rigidity is affecting ventilation
- Dantrolene consider when CK rapidly rising
- Benzos are just as good
- Bromocriptine rarely used
EMCrit Ghali Grills 003 – Further Disambiguating “PEA”
- What is PEA?
- Cardiac rhythm that should produce a pulse but no palpable pulse
- Not a good term
- The real question is whether there is adequate perfusion to obviate CPR
- Is there adequate cardiac perfusion
- Is there adequate brain perfusion
- Where to Start?
- End Tidal CO2- is it >20? And what is the trend?
- Is there a pulse ox with a good wave form?
- Is there cardiac contractility
- Throw an A line in, is systolic> 60, is diastolic >/= 40, is MAP >/=40
- Weingart has Norepi at 50mcg/minute throughout the code
- If no A line, use doppler on femoral artery, is peak velocity of doppler is>20
- Turn on the doppler and make sure sync is on
EMCrit RACC Lit Review – May 2025
The Airway Lead and the Creation of a Comprehensive Emergency Airway Quality Program
- Interventions improved first pass success rate from 85% to 95%.
Preoxygenation Strategies for Intubation of Patients Who Are Critically Ill: A Systematic Review and Network Meta-Analysis of Randomised Trials (No PDF, just link to abstract)
- Preoxygenation with NIPPV or HFNC rather than facemask oxygen might prevent hypoxaemia during tracheal intubation of adults who are critically ill. Compared with HFNC, NIPPV probably decreases the incidence of hypoxaemia during intubation. Our findings will inform updated international guidelines on preoxygenation.
- Weingart’s preox uses HFNC at 15L underneath nonrebreather at 15L.
Preoxygenation With and Without Positive End-Expiratory Pressure in Lung-Healthy Volunteers
- In this crossover randomized clinical trial, preoxygenation with PEEP was more effective than preoxygenation without PEEP, resulting in higher FeO2 values and improved ventilation independent lung regions. These findings suggest that BVM plus PEEP (8cm adults, 5cm kids) should be prioritized for preoxygenation in emergency settings.
EMRAP
Cardiology Corner: PE in Pregnancy
Anand Swaminathan, MD, and Amal Mattu, MD
Dr. Mattu and Dr. Swaminathan discuss the challenges of diagnosing pulmonary embolisms (PEs) associated with pregnancy and how to manage these patients once the diagnosis is made.
Presentation: The physiologic changes of pregnancy make the diagnosis and risk stratification tricky.
- Pregnant women are hypercoagulable throughout pregnancy and they remain hypercoagulable for 4 to 6 weeks postpartum.
- Common symptoms: Tachycardia, tachypnea, dyspnea on exertion (DOE), shortness of breath (SOB), pleuritic chest pain
- Challengingly, all of these symptoms may be present in pregnant women at baseline.
Risk Stratification:
- YEARS score/criteria with a D-dimer has been validated prospectively in pregnancy.
- Are there clinical signs or symptoms of a deep vein thrombosis (DVT)?
- Is there hemoptysis?
- Is PE the most likely diagnosis?
- If the answer is yes to any of these criteria, a D-dimer cut-off of 500 ng/mL FEU (250 ng/ml DDU) should be used. If the answer is no to ALL of the questions, a cutoff of 1,000 ng/mL FEU (500 ng/ml DDU) can be employed.
- The PERC (Pulmonary Embolism Rule-out Criteria) score should not be used in pregnancy, as it has not been studied in this population.
Imaging:
- Start with a chest X-ray (CXR); it may show an alternate diagnosis.
- If the CXR is normal, order a ventilation-perfusion (VQ) scan if feasible in your hospital.
- Access to a VQ scan may be limited by your nuclear medicine/radiology departments.
- If the CXR is normal, order a ventilation-perfusion (VQ) scan if feasible in your hospital.
- VQ scan is slightly less radiation than a computed tomography pulmonary angiography (CTPA).
- VQ scans may be read as indeterminate and require following with a CTPA.
- CTPA is more accessible and may provide alternative diagnoses.
- CTPA scans may have false negatives or may be nondiagnostic secondary to respiratory artifact or contrast timing.
- Lower extremity DVT ultrasound:
- If there is a positive DVT ultrasound and no evidence of massive PE, there is no need to pursue additional imaging as the treatment is the same.
Limitations:
- Ultrasound has the highest sensitivity when unilateral symptoms are present but sensitivity may be as low as 2% in asymptomatic patients.
- There is significantly less reliability of ultrasound to detect DVTs distal to the popliteal fossa.
- In pregnant patients, there is less reliability in detecting pelvic DVTs.
- A magnetic resonance venogram may be required to detect pelvic DVTs if there is high suspicion.
Treatment:
- Heparin and low-molecular-weight heparin (LMWH) are the only nonteratogenic treatment options.
- Submassive and massive PE should be discussed with the members of your PE response team and treated based on the resources/algorithms in your hospital network.
- Unstable massive PE: Thrombolytics are the first-line treatment and have a reported maternal survival of 92% but 20% fetal demise.
- Catheter-directed therapy and surgical or mechanical thrombectomy have been described in case reports and case series with good survival rates.
PEARL: The physiology of pregnancy makes PE both more common and more challenging to diagnose. The YEARS criteria tool is validated in pregnancy and helpful in stratifying this diagnosis.
Performance of individual criteria of the Pediatric Emergency Care Applied Research Network (PECARN) intraabdominal injury prediction rule Arnold CG, Ishimine P, McCarten-Gibbs KA, et al. Acad Emerg Med. Published online January 13, 2025. doi:10.1111/acem.15084
EDITOR’S COMMENTARY: The PECARN IAI prediction rule is highly sensitive and effective in identifying children at low risk of IAIAI, thus potentially avoiding unnecessary CT scans. However, it should not replace clinical judgment but instead should be integrated into a shared decision-making approach, considering patient factors, injury mechanisms, and local resources, before imaging is ruled out entirely.
Crit Bits: Esmolol in Sepsis
Anand Swaminathan, MD, and Haney Mallemat, MD
Dr. Haney Mallemat joins Dr. Anand Swaminathan to discuss the nuanced role of esmolol in managing persistent tachycardia in septic patients.
Background
- Esmolol is an ultrashort-acting cardio selective beta blocker (ie, beta 1 receptor) making it easily titratable as a continuous infusion.
- Esmolol has been studied in patients with sepsis with persistent tachycardia despite initial resuscitation to minimize potential adverse cardiac effects (eg, cardiomyopathy) associated with sepsis and unresolved tachycardia. However, septic cardiomyopathy is multifactorial (ie, cytokines, increased nitric oxide production, mitochondrial dysfunction).
- Several randomized controlled trials and meta-analyses have demonstrated that esmolol can effectively reduce heart rate in these patients without causing significant adverse effects on hemodynamics or tissue perfusion after resuscitation without alternative cause for tachycardia. This is generally done in the ICU although may be recommended by Intesivists in ED boarding patients.
Physiologic rationale for use of esmolol
- Early sepsis management focuses on fluids, vasopressors, antibiotics, and source control.
- A subset of patients will continue to experience sympathetic overstimulation in the form of severe sinus tachycardia.
- Persistent tachycardia can be maladaptive and actually worsen myocardial function and cardiac output.
- Esmolol has been shown in small studies and meta-analyses to reduce mortality, ICU length of stay, and time on the ventilator.
- Ideal candidates for this therapy have persistent sinus tachycardia despite adequate resuscitation; eg, elderly patients and those with pre-existing cardiac disease.
Key points for use of esmolol:
- When to consider esmolol
- Esmolol should not be used during early resuscitation.
- Consider only after standard therapies such as fluids, pressors, antibiotics, corticosteroids, and source control are in place and mean arterial pressure >65 mm Hg.
- This may be indicated many hours into the resuscitation or once a patient is in the ICU or prolonged ED patients.
- We recommend discussing with an intensivist if considering using esmolol in sepsis in the ED.
- How to use esmolol
- One suggested dosing regimen is to start with low-dose esmolol drip (eg, 25 μg/kg/minute) and titrate slowly every 15-20 minutes to a heart rate target between 80 and 94 bpm per the literature.
- Avoid bolusing due to potential hemodynamic instability.
- Use invasive monitoring (ie, arterial line) when starting esmolol.
- Final points:
- While the use of esmolol for patients with persistent tachycardia in sepsis is not currently standard ED practice, it is important to understand the rationale of therapy if your intensivist suggests it.
- In the ED, before attributing persistent tachycardia to the sympathetic overdrive, this is best thought to be unresolved tachycardia. We recommend not overlooking other causes of persistent tachycardia (eg, hypoxia, bleeding, pneumothorax, PE, myocarditis, under-sedation) before attributing it to isolated sympathetic overdrive.
- This therapy is not a quick fix; benefits are more long-term and subtle (ie, will not be noticed generally at the bedside).
PEARL: Esmolol may help mitigate harmful effects of prolonged sympathetic stimulation and severe tachycardia in septic patients, but only after careful resuscitation and in the right clinical context.
Pediatric Smackdown: GI Bleed
Ilene Claudius, MD; Jeff Seiden, MD; and Al Sacchetti, MD
Dr. Ilene Claudius, Dr. Jeff Seiden, and Dr. Al Sacchetti discuss the management of pediatric gastrointestinal (GI) bleed based on the age and general appearance of the patient. Their conversation covers can’t-miss diagnoses in patients with hematemesis or blood stool in both the neonate and infant/toddler age groups.
- Neonates with hematemesis
- Most cases are due to breastfeeding and maternal blood from cracked nipples.
- May perform an Apt test to confirm that it is maternal blood.
- Verify that patients have received their vitamin K shot at birth.
- Esophagitis and gastritis/stress ulcers are less common causes to consider.
- Most neonates who are well appearing and feeding normally can be discharged home without further workup.
- Most cases are due to breastfeeding and maternal blood from cracked nipples.
- Neonates with blood in the stool
- Evaluate for anal fissure.
- This is often due to a milk or soy protein allergy.
- May suggest dietary changes
- Dark blood mixed in with stool, especially loose stool, is more concerning.
- Consider necrotizing enterocolitis, even in full-term patients.
- May obtain a plain film of the abdomen to screen for pneumatosis
- Non-neonates with blood in the stool
- Meckel’s diverticulum typically occurs around 2 years of age.
- Consider admission for technetium-99m scan if there is a large amount of blood, persistent blood in the stool, or anemia on blood work.
- Mimics of blood in the stool:
- Patients who have eaten berries, beets or red food dyes (eg, Hot Cheetos, fruit punch)
- Cefdinir can cause stool to appear melanotic
- Meckel’s diverticulum typically occurs around 2 years of age.
- Non-neonatal patients with hematemesis
- Evaluate for epistaxis or other sources of swallowed blood.
- Patients with frank hematemesis or underlying liver disease should get blood work and be admitted.
PEARL: Most well-appearing pediatric patients do not require workup and can be safely discharged with good return precautions.
Rib Fractures + Pulmonary Contusion
Britt Guest, DO, and Kenji Inaba, MD
Dr. Guest and Dr. Inaba discuss what features of rib fractures require admission or necessitate transfer to a trauma center.
Criteria to consider when discharging a patient with rib fractures:
- Is there something in the pleural space that needs intervention (hemothorax/ pneumothorax)?
- Is the patient oxygenating well?
- Is their pain controlled with oral medications?
- Location: Higher rib fractures require more force and should be cautiously evaluated; however, if they meet the same original criteria, the patient may still be able to be discharged.
- Number of Fractures: There is no absolute number of rib fractures that automatically necessitates admission. A greater number of rib fractures suggests a more significant mechanism of injury and the patient should be thoroughly evaluated.
- Comorbidities: Older age and underlying pulmonary comorbidities should be factored into the decision to hospitalize patients with rib fractures. Both of these raise the mortality of rib fractures as these patients have less reserve.
- Pulmonary Contusions: Small pulmonary contusions that do not impede the patient’s oxygenation or pain control can similarly be managed conservatively.
- You do not need to observe or reimage specifically for concern of “blossoming contusions.”
- Admission:
- What level of care do they need (ward, telemetry, ICU)? Can you provide that level of care at your hospital?
- The majority of care is supportive with oxygenation and pain control.
- They may need transfer if epidurals or regional blocks are required in addition to traditional multimodal pain control.
- Do they need evaluation for surgical fixation? If so, transfer to a trauma center.
- Flail segment/ flail chest
- 3+ rib fractures with significant displacement (no overlap)
- with pulmonary complications and/or difficulty with pain control
- Studies examining patient experience with hospital transfer note that there is significant distress and inconvenience in being far away from their home, family, and support. Transferring is not a benign procedure and should be assessed carefully.
PEARL: Not all rib fractures require admission. If patients do not have a hemothorax/ pneumothorax, are oxygenating appropriately, and have adequate pain control with oral medications, they may be able to be discharged.
Mailbag: Bronchiolitis Paper
Ilene Claudius, MD, and Larry Mellick, MD
Dr. Ilene Claudius and Dr. Larry Mellick discuss his latest umbrella review published in Pediatric Pulmonology, examining the effectiveness of albuterol, inhaled epinephrine, and hypertonic saline in bronchiolitis treatment.
- Albuterol
- Four of six studies in Dr. Mellick’s review showed that nebulized albuterol significantly reduced respiratory distress and severity scores compared with placebo.
- While guidelines discourage routine use, a trial of 1 or 2 doses may benefit select patients.
- Inhaled Epinephrine
- Three of four studies showed clinical improvement and a reduction in hospital admissions.
- Concerns about symptom relapse after discharge were not supported by the referenced studies.
- Findings suggest that epinephrine may be useful in some cases.
- Hypertonic Saline
- Nine of eleven studies reported decreased hospital admissions, and seven showed improved clinical severity scores.
- It has significant benefit only when combined with albuterol or epinephrine.
- Take-Home Points:
- Current guidelines emphasize supportive care.
- These findings support selective use of these additional medications.
- A trial of albuterol, epinephrine, and/or hypertonic saline is reasonable.
- Treatment can be continued if effective or discontinued if ineffective.
PEARL: Trial therapies with albuterol, inhaled epinephrine, and hypertonic saline can be considered on a patient-dependent basis alongside supportive care for pediatric bronchiolitis.
Mellick, L., Walsh, P., Clanton, C., Kalra, S. and McKinney, S. (2025), Outpatient Medications Deimplemented by the AAP Bronchiolitis Guidelines: An Umbrella Review of Meta-Analyses. Pediatric Pulmonology, 60: e27391. https://doi.org/10.1002/ppul.27391
First10 EM
None
NEJM
Anticoagulation or Antiplatelet Therapy for Device-Detected Atrial Fibrillation
- Pro and con for anticoagulation versus antiplatelets
Case 13-2025: A 70-Year-Old Man with Weight Loss, Weakness, and Anorexia
The Power of Physicians in Dangerous Times
Identification and Treatment of Alcohol Use Disorder
- The oft-repeated statement that naltrexone should be avoided in patients with chronic liver disease is not firmly supported. Nal-trexone previously carried a black-box warning that was issued by the Food and Drug Administration owing to concerns about hepatotoxicity — name-ly, transiently elevated liver-enzyme levels. This warning was removed in 2013. Evidence linking naltrexone to harm in patients with chronic liver disease is lacking. Conversely, alcohol is hepato-toxic. Several sources support that naltrexone is safe in patients with cirrhosis across the spec-trum of disease severity.2-4 Yet, many clinicians remain wary of prescribing naltrexone to patients with liver disease. One reason for this hesitancy is the perpetuation of the unsupported claim in lit-erature and practice that naltrexone is harmful in patients with chronic liver disease.
Hanna Blaney, M.D., M.P.H.,1 and Elliot Tapper, M.D.2
1 MedStar Georgetown University Hospital, Washington, DC; 2 University of Michigan, Ann Arbor.
Dr. Blaney can be contacted at hannablaney@ gmail . com. Dr. Tapper reports receiving grant funding from Madrigal Pharmaceuticals and Salix Pharmaceuticals and consulting fees from Ipsen. No other potential conflict of interest relevant to this letter was reported.
REBELEM
MDCalc Wars: NEXUS Criteria Vs Canadian C-Spine Rules
- Rules out >99% of clinically-significant injuries. CCR may result in lower imaging rates than NEXUS. CCR may be more accurate and is more extensively validated.