Annals of Emergency Medicine
Antibody-Drug Conjugates: The Toxicities and Adverse Effects That Emergency Physicians Must Know
- Interstitial lung disease, which may mimic pneumonia and cause respiratory failure and death, has been seen with trastuzumab deruxtecan and mirvetuximab soravtansine; emergency treatment of this condition includes oxygenation, ventilatory support, and corticosteroids.
- Inotuzumab ozogamicin and gemtuzumab ozogamicin are both associated with sinusoidal obstruction syndrome, a potentially fatal liver dysfunction that presents with weight gain, fluid overload, and jaundice. Abnormal liver function tests in patients who have been recently treated with these agents should be cautiously evaluated.
- Ocular adverse events, especially blurred vision, and keratopathy, are common with mirvetuximab soravtansine and tisotumab vedotin
- Progressive multifocal leukoencephalopathy has been reported with brentuximab vedotin and polatuzumab vedotin.
- Tumor lysis syndrome may occur after treatment with gemtuzumab ozogamicin, polatuzumab vedotin, and brentuximab vedotin.
Take Home Point: For patients on chemo, consider ADCs as the cause for their symptoms, consider steroids for new “pneumonia”, check LFTs, urgent referral to ophthalmologist for eye issues.
Cephalosporins for Outpatient Pyelonephritis in the Emergency Department: COPY-ED Study
Take Home Point: These data support the use of oral cephalosporins in the outpatient treatment of pyelonephritis.
CJEM
CJEM debate: clinical decision rules–thinking beyond the algorithm
Diagnostic accuracy of D-dimer for acute aortic syndromes: systematic review and meta-analysis
- Abstract
- Background
- Diffusion weighted magnetic resonance imaging’s (MRI) role in predicting subsequent strokes beyond the validated Canadian TIA Score in in transient ischemic attack (TIA)/minor stroke patients with normal CT scans is unknown. In this study, we assessed the incidence of acute cerebral infarction on MRI in these patients, overall and stratified by the Canadian TIA Score levels and then we assessed subsequent stroke rates at 7, 30 and 90 days based on the presence of acute infarct on MRI.
- Methods
- This pre-planned substudy of the Canadian TIA risk score cohort was conducted across 13 Canadian emergency departments over an 11-year period. Eligible patients included adult TIA/minor stroke patients with negative CT scans who underwent MRI within 7 days.
- Results
- Among 11,507 patients, 1048 with negative CT scans had early MRI, which revealed infarction in 330 (31.5%) patients. Acute infarction rates varied by Canadian TIA Score risk group: 130 (15.4%) in low-risk, 754 (30.4%) in medium-risk, and 162 (50.0%) in the high-risk group. At 90 days, the rates of stroke in patients with a positive MRI were 2 (10.0%), 168 (22.3%), and 40 (24.7%) in low-risk, medium-risk, and high-risk groups, respectively. In comparison, in patients with a negative MRI the rate was 1 (0.9%), 7 (1.3%), and 4 (4.9%).
- Conclusions
- Combining the Canadian TIA Risk Score with follow-up MRI improves stroke risk assessment. MRI enhance the accuracy of diagnosis TIA, especially when CT is negative. The risk score helps prioritize MRI, benefiting medium-risk patients most, while high-risk patients need prompt management regardless of MRI results. Low-risk patients benefit from MRI for determining further investigations.
EMCRIT
EMCrit RACC-Lit Review – March 2025
- Early Ketamine for Status
- Weingart says add Ketamine with second dose of Midazolam at 5 min if first dose of Midazolam doesn’t work.
- From Othman et al. Paper: Participants with seizures lasting beyond the 5-min stabilization phase received 0.4 ml/kg (max 12 ml) over 2 min of the randomly assigned study drug (equivalent to ketamine 2 mg/kg (max 60 mg) in case of active drug) simultaneous with midazolam 0.2 mg/kg
- Cessation of clinical seizures at 5-min occurred in 76% of children in the Ket-Mid group compared with 21% in the Pla-Mid group (Risk ratio [RR] 3.7; 95% confidence interval [CI] 2.3-5.9; p <0.001). Compared with the Pla-Mid group, the Ket-Mid group had higher percentages of seizure cessation at 15-min (76.4% vs. 23.6%; RR 3.2, 95%CI 2.1-5.0), 35-min (83.3% vs. 45.8%; RR 1.8, 95%CI 1.4-2.4), and 55-min (88.9% vs. 72.2%; RR 1.2, 95%CI 1.04-1.45) study timepoints as well as lower percentages of repeating midazolam (23.6% vs. 79.2%; RR 0.3, 95%CI 0.19-0.46) and endotracheal intubation (4.2% vs. 20.8%; RR 0.2, 95%CI 0.06-0.66). Both groups showed no significant differences in other outcome measures.
- Othman, Amr A., Abdelrahim A. Sadek, Esraa A. Ahmed, and Elsayed Abdelkreem. “Combined Ketamine and Midazolam vs. Midazolam Alone for Initial Treatment of Pediatric Generalized Convulsive Status Epilepticus (Ket-Mid Study): A Randomized Controlled Trial.” Pediatric Neurology, March 22, 2025. https://doi.org/10.1016/j.pediatrneurol.2025.03.011.
- Zitek, Tony, Kenneth A. Scheppke, Peter Antevy, Charles Coyle, Sebastian Garay, Eric Scheppke, and David A. Farcy. “Midazolam and Ketamine for Convulsive Status Epilepticus in the Out-of-Hospital Setting.” Annals of Emergency Medicine 85, no. 4 (April 1, 2025): 305–12. https://doi.org/10.1016/j.annemergmed.2024.11.002.
- Stand on the patient’s right side if right side dominant, patient’s left side if left side dominant.
- Grab trachea from above with non-dominant hand, using index finger to find cric membrane.
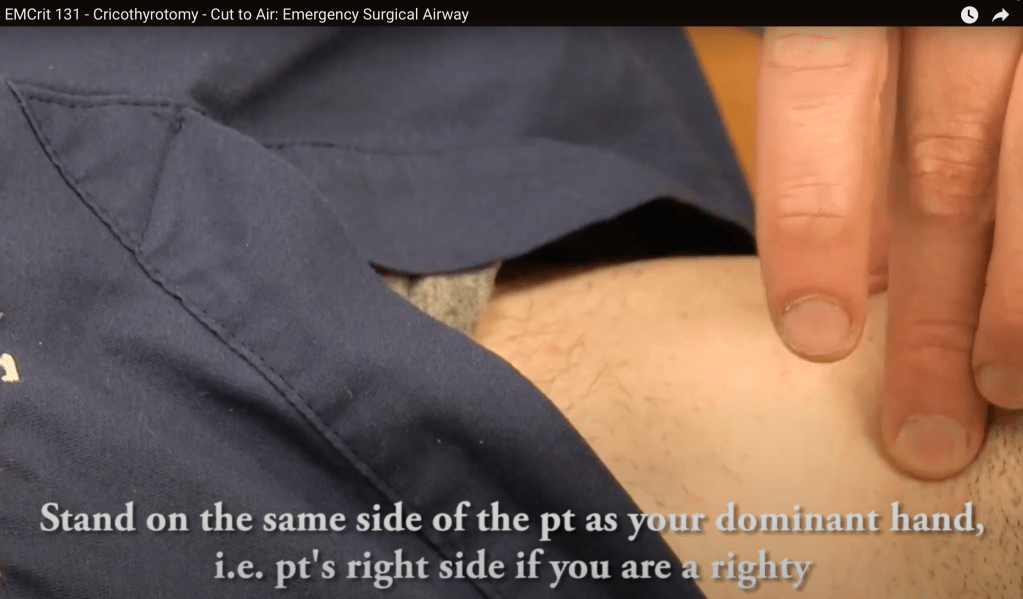
- Cut with dominant hand
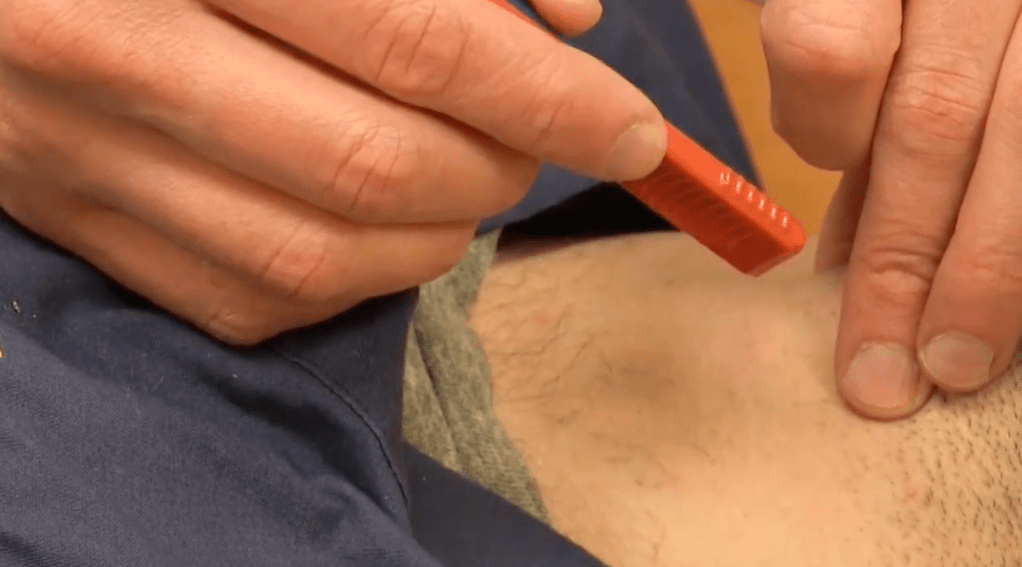
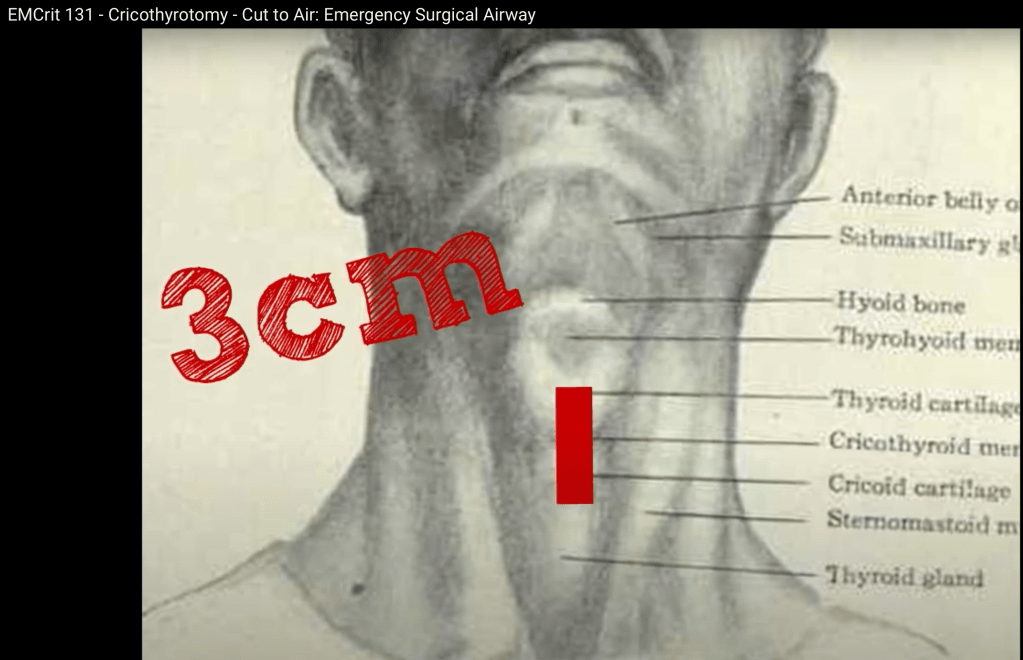
- First cut is 3 cm vertical cut
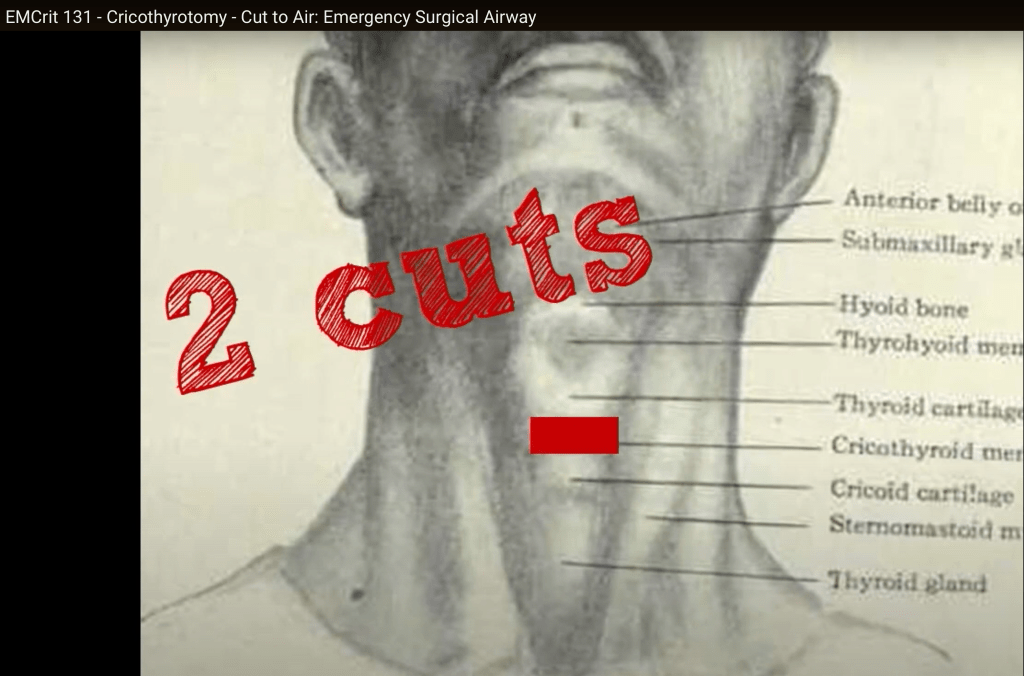
- Second cut is horizontal and is 2 cuts, cut one way and then reverse and cut in the other direction.
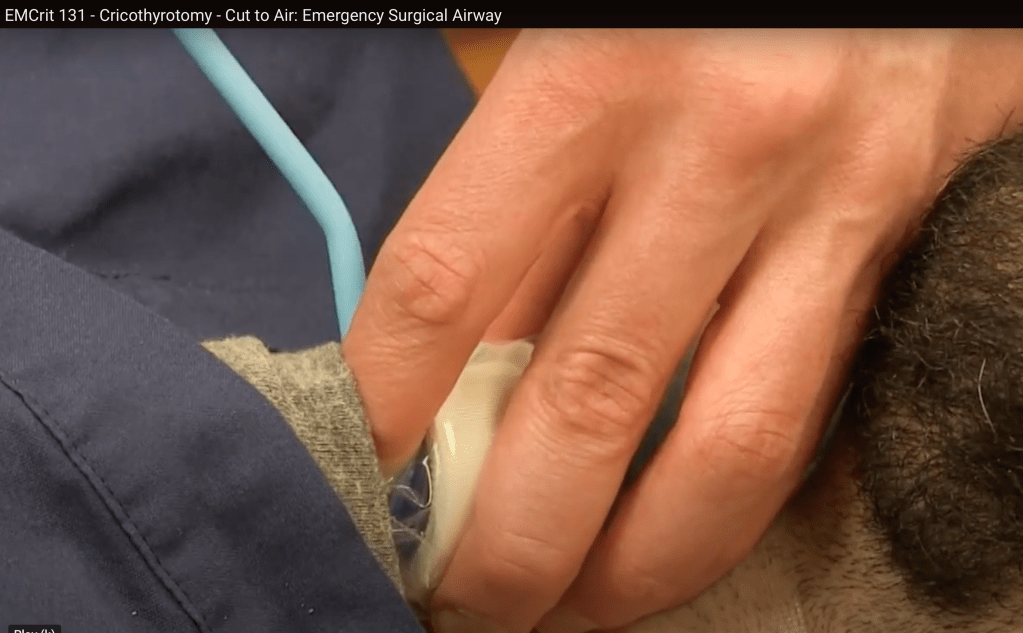
- Stick finger in the hole, confirm you can feel the cartilaginous back of the trachea and slide bougie down past the finger.
EMRAP
March 3- Case of the Week: Angioedema
Anand Swaminathan, MD, and Jan Shoenberger, MD
A 26-year-old man with a history of angioedema presents with rapidly progressing swelling of the upper lip and tongue. The patient has had 6 similar episodes in the past and has been intubated once. Despite treatment with intramuscular epinephrine and tranexamic acid (TXA), the swelling progresses. The patient is successfully intubated and later extubated after receiving icatibant.
- Physical exam
- The patient’s upper lip and anterior tongue are significantly swollen
- The posterior oropharynx is spared
- Speech is normal
- Lungs are clear
- Treatment
- Epinephrine
- Consider IM epinephrine in angioedema particularly if the patient has a rash with it making anaphylaxis with angioedema more likely.
- If the patient has significant airway compromise or if it’s unclear if you are dealing with anaphylaxis or angioedema, it’s reasonable to give epi.
- TXA
- Little evidence but may have benefit
- Theoretically interferes with the metabolic pathway that produces bradykinin
- Fresh frozen plasma (FFP)
- Case reports showing benefit but no strong evidence. Literature basis is likely biased.
- May cause breakdown of bradykinin but also contains bradykinin
- Ecallantide/icatibant
- Hereditary angioedema may be responsive to these medications
- Expensive and may not be readily available
- No proven benefit in ACEI angioedema
- Discuss applicability with your pharmacist
- Epinephrine
- Intubation
- Evaluate the posterior oropharynx and cords using either flexible bronchoscope or laryngoscope.
- When possible, use local anesthetic.
- Ketamine may further facilitate scope.
- Be prepared to intubate depending on what you find.
- Use the approach you are most comfortable with.
- Consider nasal tracheal intubation to avoid oropharyngeal swelling or fiber optic through the mouth.
- Have a double set-up for cricothyrotomy if necessary.
- Laryngoscopy may increase oral trauma and risk of swelling.
- Use of a paralytic may remove tone that is maintaining the airway.
- Evaluate the posterior oropharynx and cords using either flexible bronchoscope or laryngoscope.
PEARL: Use the approach you are most confident in to intubate angioedema cases.
March 3- Critical Care Mailbag: Orbital Compartment Syndrome
Anand Swaminathan, MD, and Scott Weingart, MD
Dr. Swaminathan and Dr. Weingart discuss the vision-threatening diagnosis of orbital compartment syndrome. They review both the classic treatment of lateral canthotomy and cantholysis and the newer “one-snip” method.
- Diagnosis
- History of facial trauma
- Measure intraocular pressure
- Elevated pressure >40 mm Hg in the right clinical context
- Physical exam findings
- Visual acuity changes
- Proptosis
- Afferent pupillary defect
- Treatment:
- Lateral canthotomy and cantholysis
- Cut the canthal ligaments to release the eyelid and provide more room for the globe.
- Do not delay for ophthalmology consultation or transfer.
- When cantholysis is performed successfully, the eyelid will pull away from the eye.
- One-Snip Method
- This involves making a vertical cut 3-5 mm medial from the lateral canthus through the lower lid, including the tarsus.
- It likely results in comparable cosmesis but is worth discussing with your ophthalmologist.
- Sedate or intubate patients, if necessary, to facilitate the procedure.
- Medical management is a possible adjunct after relieving pressure procedurally.
- Most cases require transfer to a trauma center.
- Lateral canthotomy and cantholysis
PEARL: Do not delay lateral canthotomy and cantholysis in orbital compartment syndrome. The one-snip method offers better visualization than classic lateral canthotomy.

RhoGAM Updates
Anand Swaminathan, MD, and Kelly Quinley, MD
Dr. Swaminathan and Dr. Quinley discuss rhesus (Rh) immunoglobulin, Rh sensitization, and the American College of Obstetricians and Gynecologists’ (ACOG) updated recommendations on RhoGAM administration for miscarriage and abortion in pregnancies less than 12 weeks gestational age.
- Rh immunoglobulin
- Trade name RhoGAM, also known as RhD immunoglobulin or anti-D immunoglobulin
- Antibody that targets the Rh group on the outside of human red blood cells
- Used to prevent hemolytic disease of the fetus or hydrops fetalis in future pregnancies
- Rh sensitization
- Isoimmunization or sensitization occurs when an Rh- pregnant patient is exposed to the red blood cells of a Rh+ fetus
- Dependent on volume of fetal red blood cell exposure
- Can occur due to complicated labor or abdominal trauma
- Presents risk to a future pregnancy if there is transplacental passage of anti-Rh antibodies
- Updated recommendations
- Traditionally, RhoGAM has been recommended for all Rh- patients experiencing miscarriage and undergoing abortion.
- New evidence shows fetal red blood cell exposure from these procedures in the first trimester is below the threshold required for sensitization.
- ACOG does not recommend routine Rh testing or Rh immunoglobulin administration in patients <12 weeks of gestational age who are experiencing miscarriage (regardless of management choice) or who are undergoing medication or procedural abortion.
- Can still be offered on an individualized basis
- There are no changes to recommendations for other patients including those with ectopic pregnancy.
- If dates are unknown, consider performing Rh testing while awaiting gestational age.
- These new recommendations will make RhoGAM more readily available for patients who truly need it.
PEARL: For abortion and miscarriage in pregnancies <12 weeks, RhoGAM administration is not routinely recommended.
Mild to Moderate DKA
George Willis MD and Anand Swaminathan MD
Patients with mild to moderate DKA are traditionally managed similarly to those with severe DKA: insulin drip and ICU admission. However, there is mounting evidence that a SQ insulin protocol and admission to the floor may be just as effective in this group.
Back to Basics
- DKA involves a combination of abnormalities in three parameters: anion gap metabolic acidosis, ketosis and hyperglycemia (typically).
- Standard management includes:
- Fluid resuscitation
- Checking and repleting potassium and other electrolytes
- Initiation of insulin with the target of closing the anion gap
- Searching for and treating the underlying cause
- Traditionally, patients are admitted to the ICU because of the level of nursing care and monitoring necessary to manage an insulin infusion
What About Mild to Moderate DKA?
- Patients with mild/moderate DKA have the same physiologic changes but clinically don’t appear sick or critically ill
- Using a scarce resource like an ICU bed (as well as a 2:1 nursing ratio) doesn’t seem necessary for this group
- Emerging evidence supports using a strategy based around SQ fast-acting insulin and less frequent labs allowing for a reduction in resource utilization with similar outcomes
SQ Insulin Protocol
- Excluded: severe DKA (pH < 7.0 patient is stuporous or comatose)
- Included
- Moderate DKA (pH 7.0 – 7.3 along with minimal altered mental status)
- Mild DKA (pH > 7.3, normal mental status)
- Fluids
- Patients are likely to be volume down
- 0.9% saline can complicate acid base status by adding a hyperchloremic acidosis
- Balanced solutions like lactated ringers are preferred
- Electrolytes
- Patients will be total body potassium depleted regardless of serum level
- Acidosis can mask degree of hyperkalemia as it will shift K out of cells into serum
- If patient can tolerate medications by mouth, can give both oral and parenteral repletion
- PEARL: If K < 3.5, hold insulin until K repleted above that level
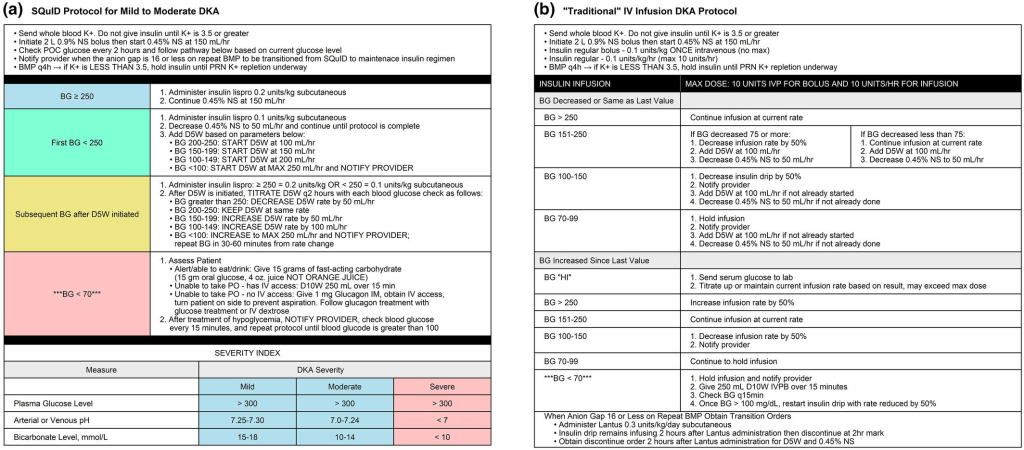
- Insulin Protocol (see images below)
REFERENCES:
Griffey, R. T.,et al. The SQuID protocol (subcutaneous insulin in diabetic ketoacidosis): Impacts on ED operational metrics. Academic Emergency Medicine, 30(8), 800-808. https://doi.org/10.1111/acem.14685
Andrade-Castellanos CA et al. Subcutaneous rapid-acting insulin analogues for diabetic ketoacidosis. Cochrane Database Syst Rev. 2016;1:CD011281.
Umpierrez GE et al. Hyperglycemic Crises in Adults With Diabetes: A Consensus Report. Diabetes Care 2024
AFib + Troponin
Anand Swaminathan, MD, and Tarlan Hedayati, MD
How to use troponins in patients with atrial fibrillation (Afib), when to get them, when not to get them, and how to accurately interpret those levels.
Back to the Basics
- Risk factors for acute coronary syndrome (ACS) risk factors are the same as those for Afib:
- Older age, hypertension, diabetes, obesity, chronic kidney disease (CKD), sleep apnea, tobacco use
- New Afib in the setting of ACS has a worse prognosis compared to presenting with sinus rhythm.
- Presence of occlusion at the level of the proximal portions of the right coronary artery (RCA) and the circumflex artery (CIRC)
- Sinoatrial nodal artery comes off the RCA in most patients (60%) and off the left CIRC in 40%
- Did the Afib start because of the ACS or is the patient having ACS and the Afib was already there, asymptomatic, and just discovered?
ECG changes
- Can have rate-related ST segment changes or ischemic changes that are not true ischemic changes but rather just an electrical phenomenon
- Especially in patients with Afib rapid ventricular response (Afib RVR)
- Up to half of Afib patients have some underlying coronary artery disease
- Can become complicated because patients with Afib have prevalence and increased risk of ACS
- Are the ECG changes really rate related or is due to underlying coronary artery disease causing supply/demand mismatch?
New-Onset Atrial Fibrillation
- Should you get a troponin? It depends!
- Ask yourself: what is the likelihood that this new-onset Afib reflects underlying coronary artery disease or ACS?
- Example: Afib in a 22-year-old patient with thyrotoxicosis or 30-year-old with alcohol withdrawal? Don’t need to order troponin.
- Example: Afib in a patient coming in with tachycardia and symptoms like chest pain or shortness of breath or dizziness? Need to order troponin.
- History and underlying comorbidities of the patient will help determine if troponin is necessary in the ED.
Thelin, J., Melander, O. Dynamic high-sensitivity troponin elevations in atrial fibrillation patients might not be associated with significant coronary artery disease. BMC Cardiovasc Disord 17, 169 (2017)
- Low-risk patients with paroxysmal Afib
- They studied a cohort that had no history of coronary artery disease or heart failure and presented with RVR and minor high-sensitivity troponin elevations.
- Those patients were then discharged in normal sinus rhythm (cardioverted vs spontaneous conversion from Afib).
- Then, a follow-up stress test was done to find out if there was any underlying coronary artery disease.
- The study found that these patients were not found to have increased incidence of abnormal stress test compared to patients who had negative high-sensitivity troponin values.
Thelin, J., Gerward, S., & Melander, O. (2021). Low risk patients with acute atrial fibrillation and elevated high-sensitivity troponin do not have increased incidence of pathological stress tests. Scandinavian Cardiovascular Journal, 55(5), 259–263
- The same Swedish lead author did another study looking at patients without coronary artery disease who presented with Afib RVR and dynamic troponin elevations.
- They compared these patients with those who had normal high-sensitivity troponins and again they were unable to demonstrate any increased risk of ACS, revascularization, or death due to ischemic heart disease.
Chronic Atrial Fibrillation Patient
- Elevated high-sensitivity troponins are a strong independent risk factor for cardiovascular events and mortality.
- Higher risk of stroke, myocardial infarction, and cardiac mortality
- Chronic Afib patients can have minor increased troponin elevations within assay thresholds.
- These patients are typically older with comorbidities.
- Cardiac troponins and adverse outcomes in European patients with atrial fibrillation: A report from the ESC-EHRA EORP atrial fibrillation general long-term registry
- Elevated troponin levels were associated with increased risk of all-cause mortality, adverse cardiovascular events, hemorrhagic events, and then subsequent hospital admissions (even after they excluded patients with known coronary artery disease or history of coronary artery disease).
- High-risk patients can have troponins trended.
- We may need to have a lower threshold to admit these high-risk patients who are presenting with Afib and even a minimally elevated troponin.
Delta Troponin
- There are no guidelines to direct us on what the delta/second troponin should be in a newly diagnosed Afib patient who has elevated initial troponin.
- The algorithms we have in place are for chest pain and ACS.
PEARL: History and underlying comorbidities in the Afib patient will help determine if troponin is necessary.
EMA 2025 February Abstract 9: Complications of US-Guided Nerve Blocks in the Emergency Department
- EMA EDITOR’S COMMENTARY: This study is the first report from the NURVE Block Registry describing the use of UGNBs from 11 EDs in the U.S. Among almost 3,000 blocks, most were fascia iliaca/femoral nerve blocks and erector spinae plane blocks performed by residents. The authors report extremely low complication rates coupled with good efficacy estimates. If the data had been collected prospectively, this study would be a serious game changer, but we can’t ignore the potential reporting bias, selection bias, and threats to generalizability in the registry. However, I still feel that the large sample size and excellent attention to detail in the methods mean that this article will move the needle, and we should all be learning about these blocks. I have now performed several (with help!) for hip/femur fractures and was thoroughly impressed with the results in most cases. This is patient-focused care. At minimum, this article should encourage you to read about these blocks and maybe even try one.
Neurocritical Care Mailbag: TBI Management
Anand Swaminathan, MD, and Evie Marcolini, MD
Dr. Marcolini and Dr. Swaminathan discuss the Brain Injury Guidelines (BIG), which provide a structured approach to managing blunt traumatic brain injuries (TBIs).
- Background
- BIG was developed in 2013 by Drs. Bilal Joseph, Peter Rhee, and colleagues from a retrospective study of 3,800 patients with blunt TBI.
- Factors such as age, medications, injury mechanism, neurologic exam findings, and imaging results were assessed.
- The goal of the guidelines was to reduce unnecessary transfers, neurosurgical consults, and repeat computed tomography (CT) scans for patients unlikely to require surgery.
- The guidelines categorize patients into 3 categories:
- BIG 1:
- Mild injuries with normal serial neurologic exams, no intoxication, and no major risk factors
- No anticoagulation/antiplatelet use
- Types of injuries:
- Small hemorrhages:
- Subdural hematoma (SDH) or epidural hematoma (EDH): ≤4 mm
- Single intraparenchymal hemorrhage (IPH): ≤4 mm
- Trace subarachnoid hemorrhage (SAH)
- No intraventricular hemorrhage (IVH)
- No skull fractures
- Small hemorrhages:
- Management: 6-hour ED observation, no repeat head CT, no neurosurgical consult
- Disposition:
- Safe for discharge if stable
- Possibly saves hospital admission (no patients required upgrades in the original study)
- BIG 2:
- Moderate injuries with mild risk factors (eg, intoxication, non-displaced fracture, slightly larger hemorrhages)
- No anticoagulation/antiplatelet use
- Types of injuries:
- SDH or EDH: 5 to 7 mm thick
- Single IPH: 5 to 7 mm or IPH in ≤2 locations
- Localized SAH
- No IVH
- Non-displaced skull fractures permitted, nodepressed skull fractures
- No midline shift, mass effect, or herniation
- Disposition:
- Hospital admission, but no repeat CT or neurosurgical consult unless condition worsens
- Possibly saves transfer
- In the study, 9 out of 313 patients (2.9%) required upgrades:
- 7 for worsening head CT
- 2 for worsening exam
- None required neurosurgical intervention
- BIG 3:
- Severe injuries requiring close monitoring, repeat CT scans, and neurosurgical evaluation
- Patients on antiplatelets or anticoagulants were included in BIG 3 for original study
- Management: Admission to a higher level of care, full neurosurgical evaluation
- BIG 1:
- Validation of BIG:
- BIG was validated in a 2022 multicenter study of 2,300 patients, showing that no BIG 1 patients clinically worsened, and only 2 out of 295 BIG 2 patients experienced clinical deterioration.
- In this external validation study, BIG guidelines would have reduced
- CT scans by 29% overall
- 100% reduction for BIG 1 patients
- 98% reduction for BIG 2 patients
- Significant reduction in admissions and neurosurgical consults
- CT scans by 29% overall
- Limitations and considerations:
- Emergency physicians may be hesitant to discharge patients with visible bleeding on CT scans.
- Direct-acting oral anticoagulants(DOACs) are more common today but were not included in the original study.
- Neurosurgeons are already informally following these guidelines in many hospitals.
- Hospitals without in-house neurosurgery can avoid unnecessary patient transfers by using BIG for risk stratification.
- Encouraging collaboration among emergency medicine, neurosurgery, and critical care teams is essential to integrating BIG into hospital protocols.
PEARL: The BIG guidelines provide an evidence-based framework that can safely reduce unnecessary imaging, hospital admissions, and neurosurgical consultations while ensuring excellent care for TBI patients. Emergency medicine providers should be familiar with the guidelines, and hospitals should consider a multispecialty collaborative approach in implementing them.
REFERENCES:
The BIG (brain injury guidelines) project: defining the management of traumatic brain injury by acute care surgeons
Joseph B, Friese RS, Sadoun M, et al. J Trauma Acute Care Surg. 2014;76(4):965-9. doi: 10.1097/TA.0000000000000161. PMID: 24662858.
Validating the Brain Injury Guidelines: Results of an American Association for the Surgery of Trauma prospective multi-institutional trial
Joseph B, Dubose J, Dugan A, et al. J Trauma Acute Care Surg. 2022;93(2):157-165. doi: 10.1097/TA.0000000000003554. PMID: 35343931
EM Updates
How To See Emergency Department Patients
- Ask PMH/Meds/SocHx/ADLs before asking why they are there, presumably because you will forget to do it later.
First10EM
Rethinking Acute Pancreatitis in the ED
- Order a triglyceride in all cases
- Order a biliary ultrasound in all cases
- If patient can tolerate oral nutrition, feed them (unless surgical or triglycerides)
- Discharge only if symptoms well controlled and patient can tolerate a solid oral diet.
JAMA
- Conclusions and Relevance Compared with NIV, HFNO met prespecified criteria for noninferiority for the primary outcome of endotracheal intubation or death within 7 days in 4 of the 5 patient groups with ARF. However, the small sample sizes in some patient groups and the sensitivity of the findings to the choice of analysis model suggests the need for further study in patients with COPD, immunocompromised patients, and patients with ACPE.
NEJM
Tirzepatide for Obesity Treatment and Diabetes Prevention
Bacterial Vaginosis — Time to Treat Male Partners
Unexplained or Refractory Chronic Cough in Adults
REBELEM
None