American J of Emerg Med
- No difference
COVID-19 in pregnancy and the puerperium: A review
for emergency physicians
Annals of Emergency Medicine
Management and Outcomes of Children With Nursemaid’s Elbow
- Radial head subluxation in 1-3 year olds is a clinical diagnosis that does not require radiographic confirmation unless a fracture is suspected.
- X-rays were done is 28.5% of patients.
- 0.3% of patients had fractures.
- Avoid unnecessary x-rays in this population.
- Distal radius buckle (torus) fractures are the most common fractures of childhood and carry an excellent prognosis.
- Removable wrist splint for 2-4 weeks without sports.
- May return to sports after 2-4 weeks as long as they wear the splint.
- Splint removal after 4-6 weeks as long as no pain with good range of motion.
- Home management just as good as PCP referral.
- No ortho referral needed.
Risk of Leukemia in Children With Peripheral Facial Palsy
- Among 644 patients age 5 months to 17 years with acute onset palsy, 5 had leukemia identified as the cause, all demonstrated blasts on their CBC.
- Steroids can decrease the blast count, delaying the diagnosis, also increases risk of tumor lysis syndrome.
- Authors suggest a screening CBC for all kids with facial palsy before initiating steroids.
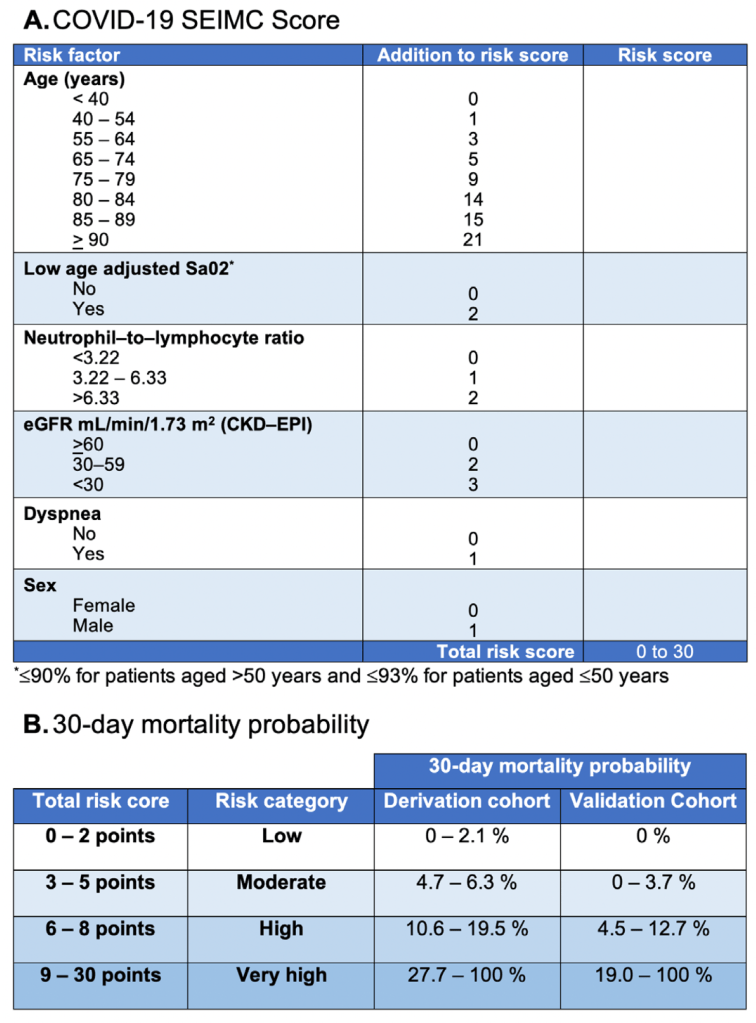
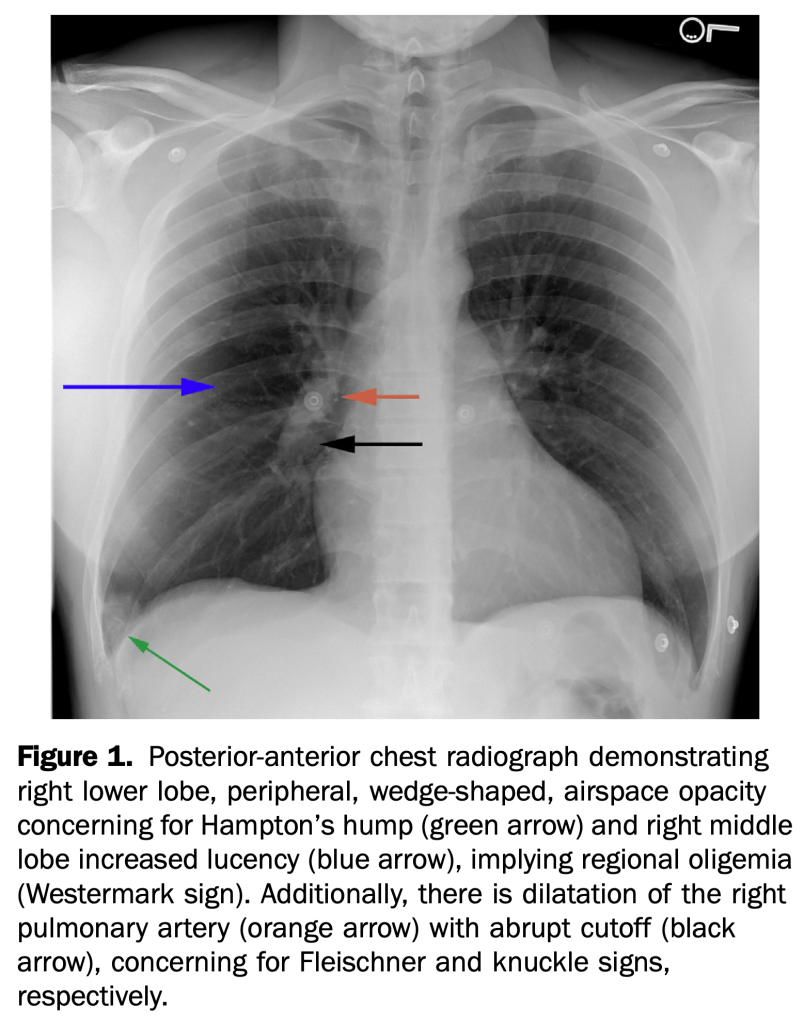
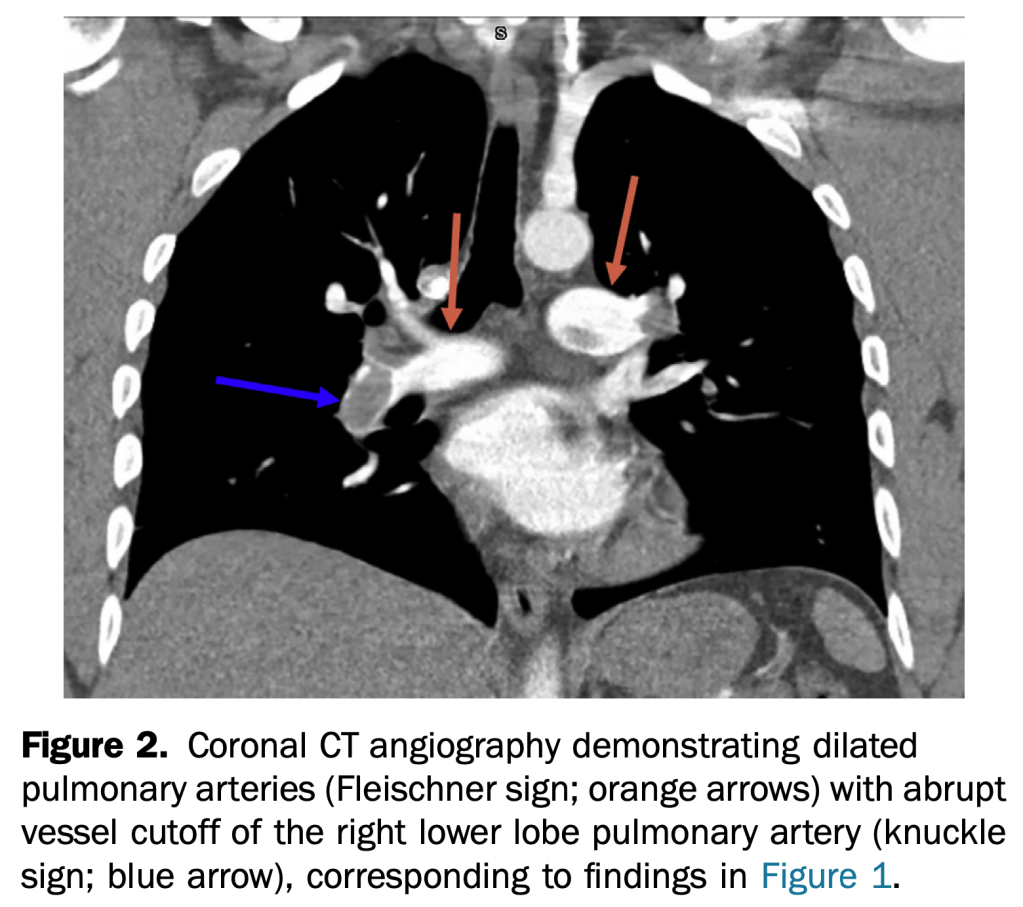
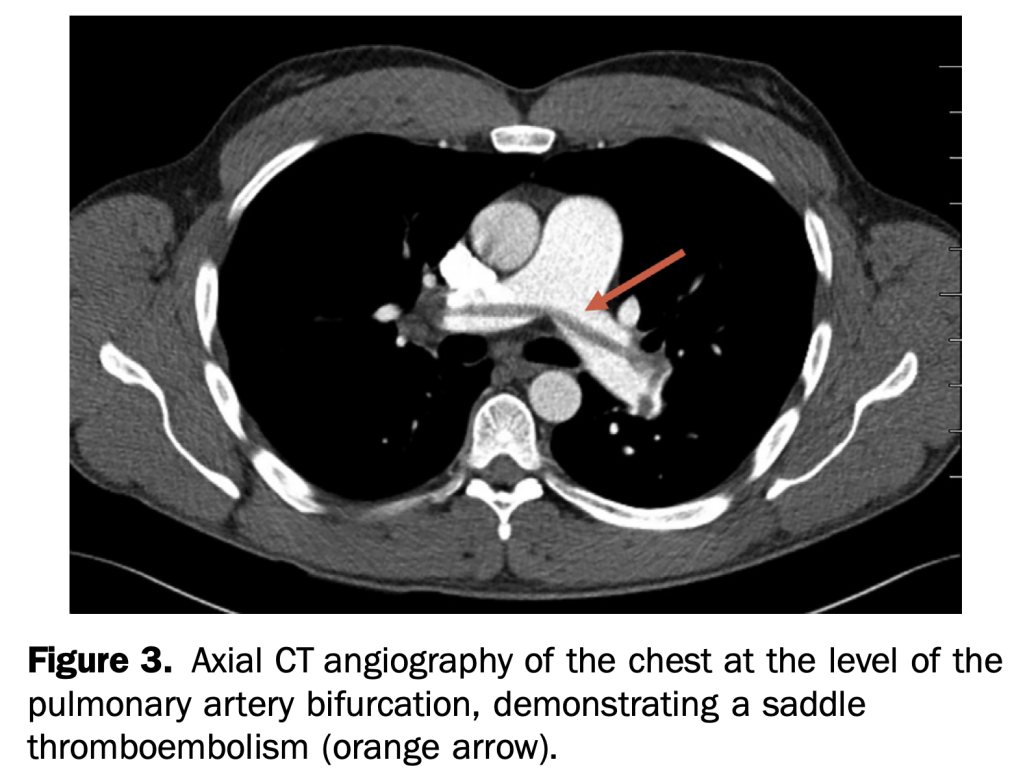
- An otherwise healthy 35-year-old active duty military infantryman presented to the emergency department, complaining of intermittent dyspnea over one-week duration, which was worsened by exertion. He recalled some unusual left leg cramping three weeks before and reported an uncomplicated tooth extraction one week before, but denied any invasive surgeries.
- This case demonstrates multiple rare but specific radiographic findings of pulmonary embolism. These include the Westermark, knuckle, and Fleischner signs, in addition to Hampton’s hump.
A 36-year-old man presented to the emergency department with double vision. Four weeks before, he had been struck in the face and he underwent open reduction and internal fixation of a mandibular fracture. He had intact cranial nerves in the immediate postoperative period. On examination, he displayed preserved visual acuity, a right-sided cranial nerve III palsy with an inferiorly abducted right eye, loss of medial and upward gaze, significant right-sided ptosis, and asymmetric mydriasis (Figure 1 and Video E1 [available online at http://www.annemergmed.com]). A bruit was auscultated over the affected eye.
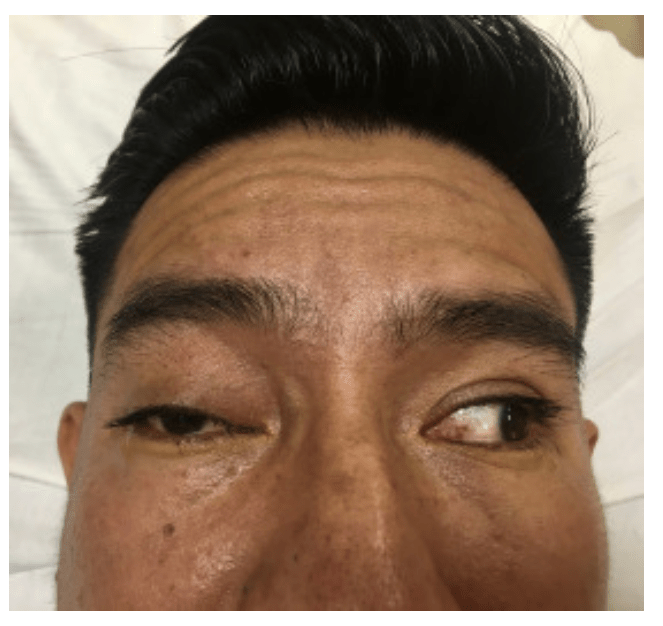
Computed tomographic angiography of the brain revealed arterial filling of the cavernous sinus, consistent with a right-sided carotid-cavernous fistula and a dilated right ophthalmic vein.
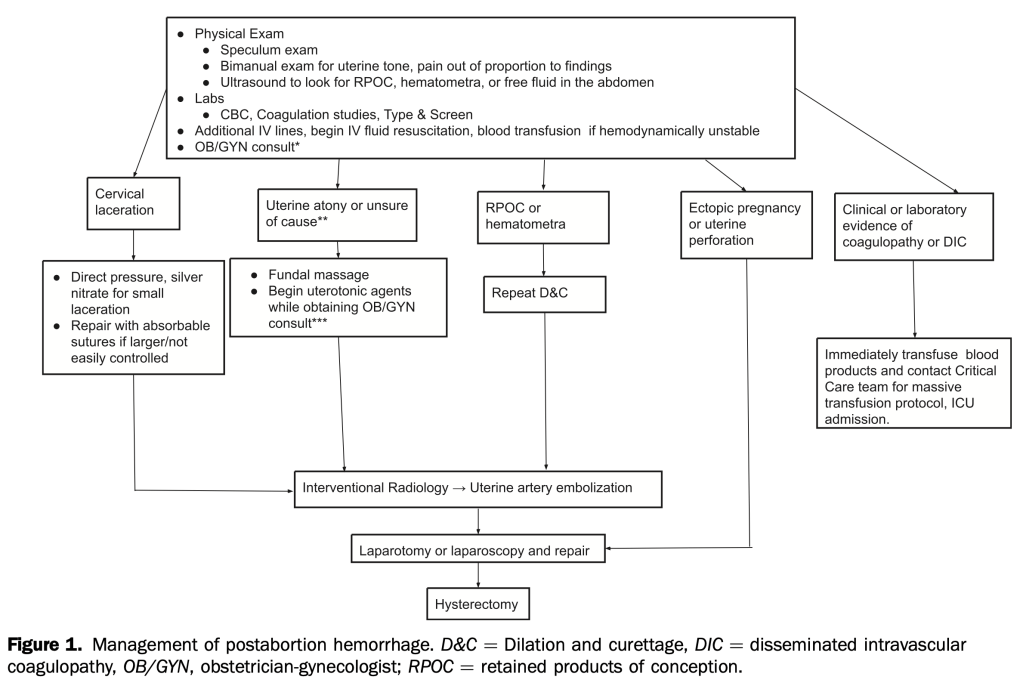
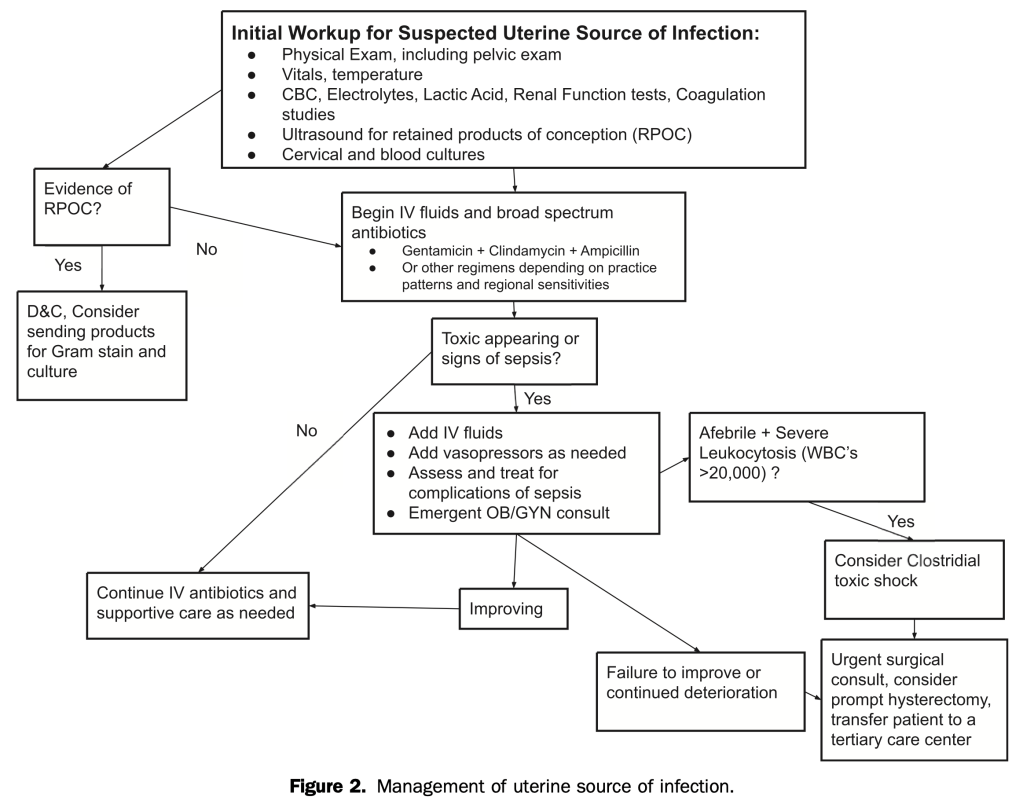
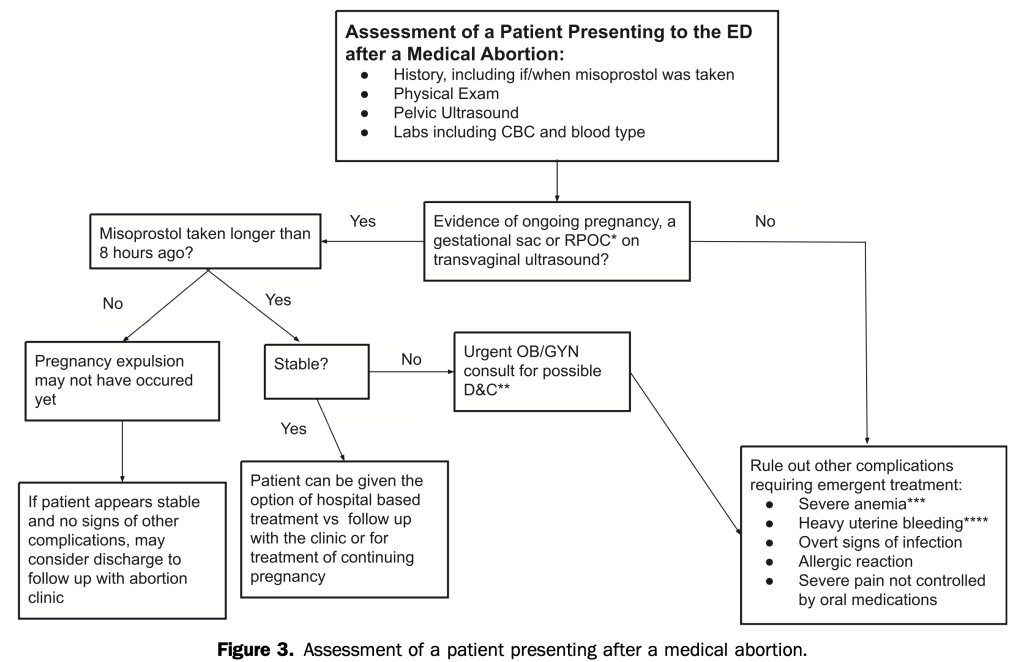
Management of Postabortion Complications for the Emergency Medicine Clinician
- Good review and algorithms to identify and manage the rare serious complication of bleeding and infection.
Retrospective Review of Pregnant Patients Presenting for Evaluation of Acute Neurologic Complaints
- Between January 1, 2010, and May 31, 2017, 205 pregnant patients presented to the ED with a neurologic chief complaint. The majority of patients had a normal neurologic examination result. Patients with an abnormal examination result were not more likely to have clinically significant imaging findings.
- Within our population, 28% underwent imaging, and noncontrast magnetic resonance imaging was the most common modality. Five patients had clinically significant imaging findings. Specifically, 3.3% of patients with abnormal examination result had significant findings and 2.3% of those with a normal examination result had significant findings.
- A normal examination result does not adequately exclude serious intracranial pathology, and diagnostic vigilance is justified.
- In patients presenting to an ED with atraumatic epistaxis that is uncontrolled with simple first aid measures, topical tranexamic acid applied in the bleeding nostril on a cotton wool dental roll is no more effective than placebo at controlling bleeding and reducing the need for anterior nasal packing.
BMJ
- The Canadian TIA Score stratifies patients seven day risk for stroke, with or without carotid endarterectomy/carotid artery stenting, and is now ready for clinical use.
- Incorporating this validated risk estimate into management plans should improve early decision making at the index emergency visit regarding benefits of hospital admission, timing of investigations, and prioritization of specialist referral.
- Excluded: had neurological deficits for more than 24 hours (that is, a stroke according to the World Health Organizationí s definition), had a decreased level of consciousness from their baseline (that is, Glasgow Coma Scale <15 in previously cognitively normal patients), had an alternative diagnosis (for example, hypoglycemia, seizure, electrolyte imbalance, or migraine), presented more than seven days after onset of the neurological symptoms, or were treated with tissue plasminogen activator or embolectomy for an acute stroke.
- 7607 consecutively enrolled adult patients (80.6% of all potentially eligible patients)108 (1.4%) had a subsequent stroke within 7d
- 83 (1.1%) had carotid endarterectomy/carotid artery stenting within 7d
- 9 patients had both within 7d leaving 182 with outcomes
- Low risk: 16.3% of patients, 7d risk of CVA or carotid procedure ≤0.5%;
- Medium risk: 72.1% of patients, 7d risk of CVA or carotid procedure 2.3%;
- High Risk: 11.6% of patients, 7d risk of CVA or carotid procedure: 5.9%;

- Authors recommend Head CT and routine follow-up for low risk patients, CTA head/neck for medium risk and with rapid follow-up.
Emerg Med J
None
EMRAP
Critical Care Mailbag: Intubating with Severe Acidosis- Weingart
- BIG PEARL: avoid intubation in severe metabolic acidosis patients, if possible, allow them to continue their compensatory breathing until you can correct underlying problem (especially true for easily fixable problems like DKA, less so for severe sepsis).
- Smaller pearl: cause of acidosis as important as the actual number in determining prognosis, low pH from COPD, DKA or even salicylate poisoning easier to resuscitate and better prognosis than septic shock.
- Scant evidence for bicarb boluses but Weingart doesn’t use because if patient is already maxed out on respiratory compensation, the added bicarb simply gets converted to CO2 that can no longer be blown off.
- Weingart does use 3 amps of NaBicarb in D5W drip for salicylate poisoning, but not for DKA
- Place on Vent with NIV mask with pressure support to augment respiratory drive before intubation to determine the minute ventilation that needs to be matched after intubation.
- Once patient is induced but before paralysis occurs, patient should be switch to vent settings RR 12, TV 8cc/kg, this lower RR should reduce risk of gastric dissension and vomiting.
- Once patient is intubated, empiric settings RR 30, TV 8cc/kg.
- Ask RT to confirm patient is exhaling whatever they are inhaling and not air stacking due to the high RR.
- If patient is air stacking, switch to the square breathing curve with a high inspiratory flow rate.
Chest Pain in Pregnancy: Part 3 Pulmonary Embolism- Bavolek
- Endorses the Years adjusted d-dimer approach based on the 2019 van der Pol NEJM study.
- See my post on shared decision-making for PE work-up in pregnancy.
- Consider in patients with headache and hypercoagulable states: pregnancy, ocps, malignancy…
- CT venogram or MR venogram
Community Acquired Pneumonia II
- IDSA recommends only 5 days of antibiotics, not 7-14.
- Discourage azithromycin alone due to high resistance from Strep Pneumo.
- Amoxicillin plus Doxy or Macrolide for atypicals if healthy,<65 and no recent antibiotics
- Augmentin plus Doxy or Macrolide if comorbidities or >/=65 or recent antibiotics
- UPTODATE has good recommendations.
JAMA
- Retrospective cohort study
- 27 918 patient encounters (16 212 women [58.1%]; mean [SD] age, 58.7 [15.2] years) were included in the study.
- Of patients with an initial troponin measurement below the level of detection, 14 459 (51.8%) were discharged after a single troponin measurement, and 13 459 (48.2%) underwent serial troponin tests.
- After adjustment for cardiac risk factors and comorbidities, there was no statistically significant difference in the primary outcome of acute myocardial infarction or cardiac mortality within 30 days between the 2 groups (single troponin, 56 [0.4%] vs serial troponin, 52 [0.4%]; adjusted odds ratio, 1.41 [95% CI, 0.96-2.07]).
- Patients discharged after a single troponin test had lower rates of coronary artery bypass graft (adjusted odds ratio, 0.24 [95% CI, 0.11-0.48]) and invasive coronary angiography (adjusted odds ratio, 0.46 [95% CI, 0.38-0.56]).
- This study suggests that patients are routinely discharged from the ED after a single negative troponin test result, and when compared with serial troponin testing, a single troponin test appears safe based on current physician decision-making, with no difference in rates of 30-day cardiac mortality and acute myocardial infarction, which are low in both groups.
NEJM
Management of Antithrombotic Therapy after Acute Coronary Syndromes
- Primarily for hospitalists and cardiologists.
- Didn’t realize that addition of anticoagulant therapy to anti platelet therapy has been shown to improve outcomes after ACS but is not routinely done due to increased risk of bleeding.
Circadian Mechanisms in Medicine
Thorax
- Highly recommended by Evidence Alerts