Academic Emergency Medicine
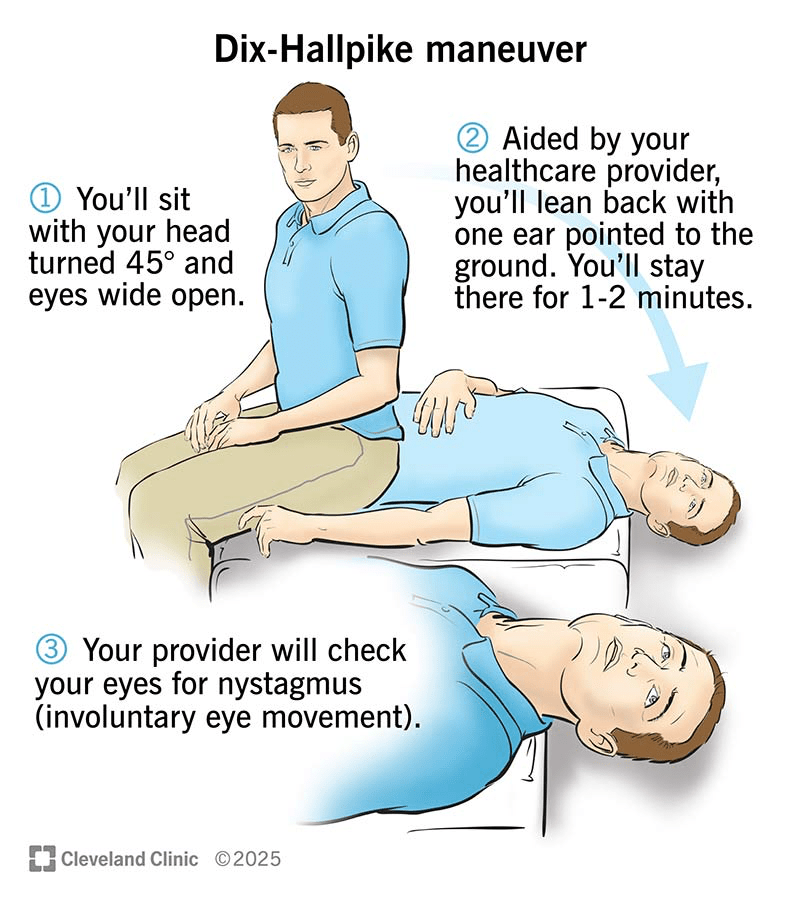
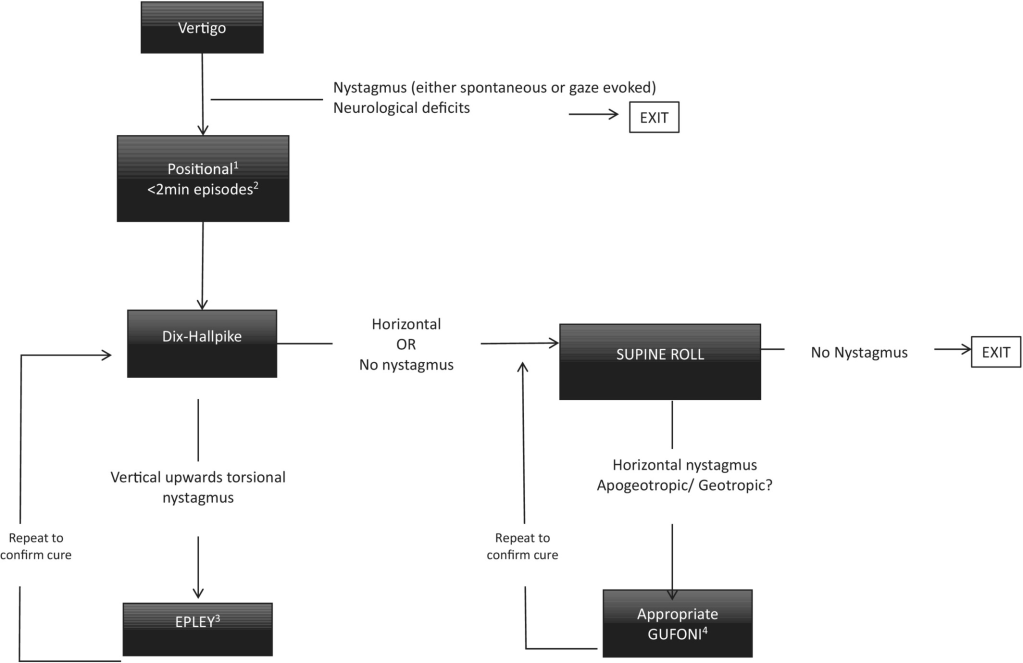
- If both tests (Supine Roll and Dix Hallpike) were negative (no nystagmus), no maneuver should be
performed. - If the Dix-Hallpike test was positive, the Epley maneuver
should be performed. - If the supine roll test was positive, the Gufoni maneuver
should be performed.
Dix Hallpike
EMCrit 358 – Dizziness Makes Me Dizzy Still! – GRACE-3 and more with Peter Johns
Annals of Emergency Medicine
- Can trigger Cytokine Release Syndrome (CRS) which looks like sepsis and requires infusion of Tocilizumab for grades 2-4 CRS.
Clinical Toxicology
- This expert panel recommends Zyprexa if Droperidol not available, onset time is nearly identical to droperidol (17 minutes).
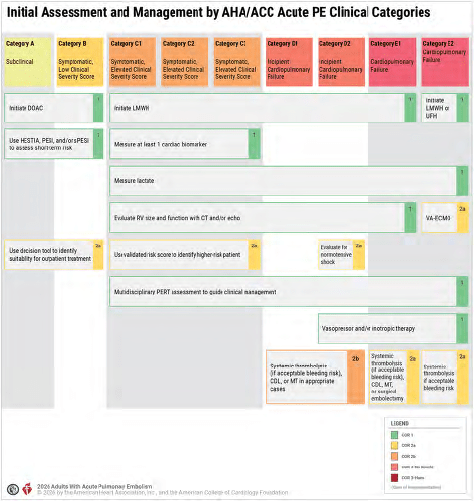
Circulation
- Thrombolytics for Category D
EMCRIT
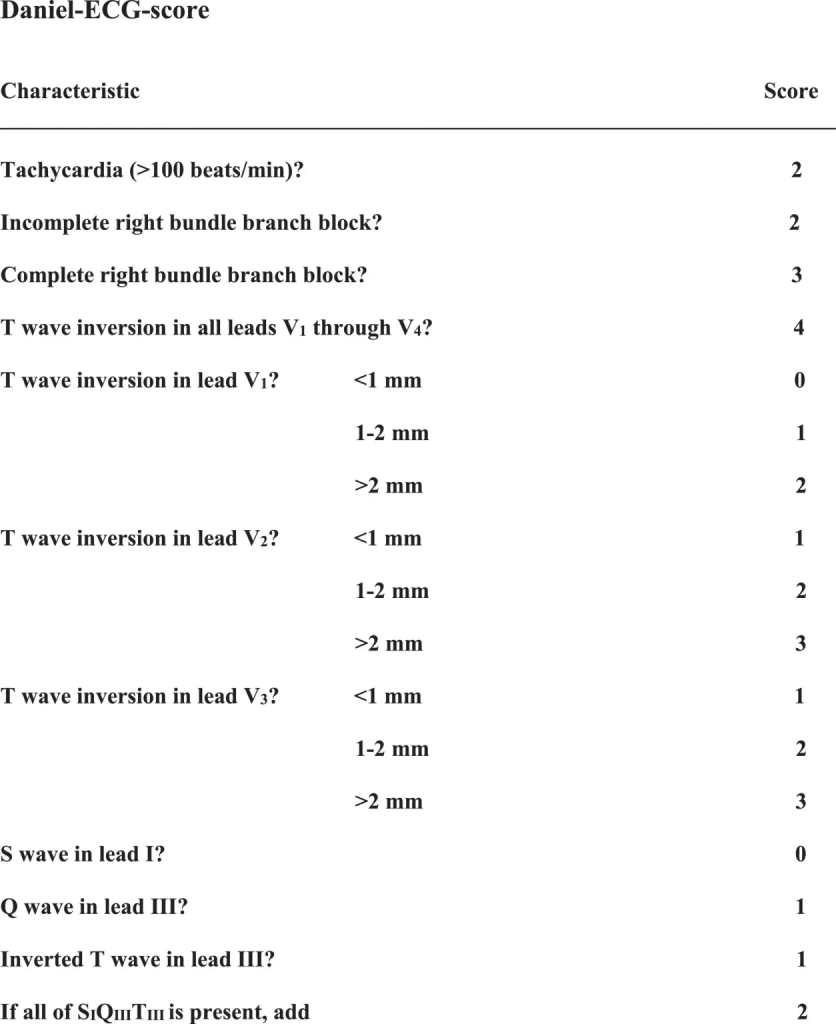
EMCrit Wee – ECGs in Acute Pulmonary Embolism – Death Threats in Little Squiggly Lines
- Deep dive on ECG findings for PE inspired by the scary malpractice case from 2025 where a young patient who was PERC negative died and physician lost lawsuit due to classic ecg findings for acute PE (twi in inferior and anterior leads).
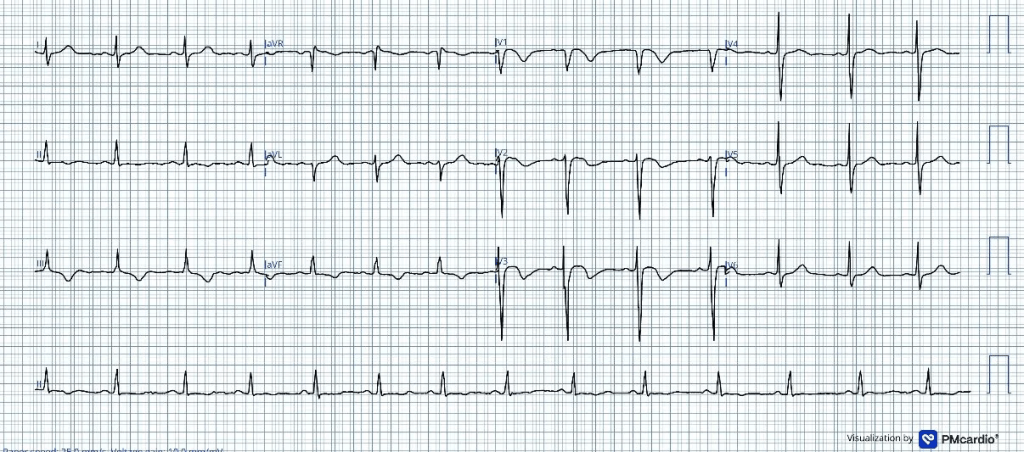
- 4 key findings to document on your ecg
- no rbbb or incomplete rbbb
- TWI in V1-V4 (In the anterior leads, the TWI are accompanied by a recognizable QRS and ST pattern: little R, big S, coved st-segment, then big TWI)
- no S1Q3T3 (tiny r with deep S is considered a Q3)
- sinus tach
- If patient has one of the 4 then acknowledge and either argue why your suspicion for PE is still too low to test or proceed to D-Dimer.
EMRAP
Risk Management Series: Abdominal Pain
Mike Weinstock, MD, and Colin Kaide, MD
Dr. Weinstock and Dr. Kaide review a case presentation of abdominal pain that resulted in an adverse outcome. They review the top 10 ways to keep patients safe and avoid medicolegal encounters, specifically in those who present with abdominal pain.
Case Presentation:
- An elderly woman presents to an ED in the northeastern United States.
- She complains of minimal abdominal pain with constipation.
- Previous diagnosis of constipation
- Lab testing is unremarkable.
- The patient is discharged.
- The patient dies shortly after from a ruptured abdominal aortic aneurysm (AAA).
Case Litigation:
- The facts are in dispute:
- The family said she had severe pain to the point that she couldn’t even walk.
- The emergency physician said the pain was minimal.
- There was a significant disparity in pain severity.
- Plaintiff’s emergency medicine expert testimony:
- It is incumbent upon the examining physician to rule out all potential serious and or life-threatening causes of the abdominal pain/symptoms before making a definitive diagnosis.
- The defendant admitted that she did not suspect an AAA.
- This was based on the decedent’s complaints of pain that was not that severe.
- The clinical picture was not suspicious for AAA.
- The jury found for the defendant.
Abdominal Pain:
- Can be very complicated
- Lots of different structures in abdomen
- Lots of different patterns of innervation
- Pain occurring in abdomen can be felt in other parts of the body
Top 10 Ways to Keep Patients Safe
(and also to avoid a medicolegal encounter)
10. Thorough Documentation
- Be specific and use descriptive terms and relevant information!
- Your documentation should accurately reflect what it is that you are seeing.
- Example:
- GOOD: “abdomen soft, non-tender”
- BETTER: “abdomen soft, non-tender, no rebound or guarding, patient is able to ambulate”
9. Imaging Tests Can Lie to You
- Dr. Kaide’s Article
- “The donut of half-truths”
- “Never order a test you don’t understand”
- If you don’t understand the sensitivity and specificity of the test for the specific thing you’re looking for, it can be problematic.
- Cochrane Review for Appendicitis
- If you have a moderate to high pretest probability of ~40% for somebody having appendicitis, a negative CT still gives you about a 5% chance of having appendicitis.
- CT angiogram looking for mesenteric ischemia:
- 90% sensitive
- 10% of the time, it’s going to miss the diagnosis
- Depending upon the situation you run into:
- You have to be willing to either accept that risk or be able to explain why you didn’t pursue this diagnosis further.
- You have to mix your understanding of this with the pretest probability for the disease in question.
8. Bounceback Rates for Abdominal Pain Are Higher Than Average
- Bouncebacks can be a good safety net.
- We want patients to come back if their disease progresses, changes, or does not resolve.
- The bounceback rate for abdominal pain is higher than average.
- Pain or symptoms are worse
- Planned return for re-examination
- Before the patient leaves the ED, imagine that the patient is going to bounce back with something worse.
- Try to address that consideration before the patient leaves the ED.
- Misdiagnosis does not equate to medical malpractice.
7. Missed Appendicitis = Biggest Medical Legal Risks
- The problem isn’t that you didn’t think about appendicitis BUT that the CT was negative and the patient ended up with a complication.
- Atypical presentation:
- Non-localized pain, diarrhea (which is not a common symptom in appendicitis)
- Failure to consider the diagnosis of appendicitis
- Medical malpractice cases: misdiagnosis of gastroenteritis and anchoring it
- Big caution for lone vomiting with no diarrhea
6. Mesenteric Ischemia
- Can be tricky!
- Consider in patients who have POOP and POOP+
- POOP = pain out of proportion
- POOP+ = pain out of proportion + clotting issue (atrial fibrillation [Afib], hypercoagulable state, vascular disease)
5. Ectopic Pregnancy +/- Rupture
- Do a pregnancy test!
- Low-hanging fruit
- Indicated in everyone of childbearing age
- If a patient’s pain doesn’t make sense, it is very easy to order the ultrasound and take a look.
4. Get an ECG for Abdominal Pain (especially in elderly patients)
- Low-hanging fruit to rule out cardiac pathology
- Dr. Weinstock shares a patient encounter of an elderly patient with epigastric pain
- Negative abdominal workup but inferior ST-elevation myocardial infarction (STEMI) on ECG
- Abdominal pain or back pain + weird story = CONCERNING
- Consider retroperitoneal pathology
3. Pediatric Testicular Torsion
- Study by Gaither (Journal of Pediatric Urology)
- Legal cases that originated out of missed testicular torsion:
- 31% of these patients presented with abdominal pain, not with testicular pain
- 40% of patients who have testicular torsion have had a previous torsion and detorsion event
- Ask if previous event like this has occurred
- Be aware that the patient who looks great in the ED:
- May have detorsed that testicle
- May have partial torsion or partial reversal of a torsion
- Biggest problems:
- Failure to examine testicles
- Failure to obtain ultrasound or obtain in timely manner
- Failure to get surgical intervention in timely fashion
2. Bariatric Surgery Patients
- Find out what kind of surgery they have had:
- Most common currently is Roux-en-Y gastric bypass
- Sleeve gastrectomy
- Adjustable gastric band (older procedure)
- Biliopancreatic diversion, duodenal switch, or vertical banded gastrofundoplasty (much older procedures)
- Complications
- Obstructions
- Marginal ulcers (at anastomotic site)
- Perforations
- Internal hernias
- MUST KNOW THIS!
- Pocket in which parts of the intestine can herniate into and create an internal obstruction and/or internal hernia
- Most common presentation is intermittent symptoms
- “Waxing and waning”
- Created by the surgery itself
- CorePendium: Post-Bariatric Surgery Complications
- EM:RAP 2020 January: Complications after Bariatric Surgery
- Discharge Instructions
- Explain the decision-making process to the patient.
- Engage in shared decision-making.
- “We don’t have a firm diagnosis for you. I want you to come back if it gets worse. We have ruled out a lot of the possibilities, but there are still some things that we haven’t settled yet completely. I want you to have a low threshold to come back and get rechecked because we’re not 100% sure you don’t have something more emergent.”
- Document this conversation in the chart.
- If someone reviews this, they can understand your decision-making process.
PEARL: If it’s not in the differential, it won’t be in the diagnosis. Differential diagnosis is a dynamic process. More specific documentation wins. Review the top 10 ways to keep patients safe and avoid medicolegal encounters.
Obstructive Uropathy
Chris Reilly, MD, and Megan Cooper, DO
Dr. Chris Reilly gets an expert opinion from urologist Dr. Megan Cooper on all things obstructive uropathy. Their discussion covers a general approach to urinary retention, pearls for difficult foley placement, and evaluating for post-obstructive diuresis.
- Approach to Obstructive Uropathy
- Obtain a careful history to determine underlying cause:
- Differentiate between complete obstruction vs reduced stream
- New or changed medications or substance abuse
- Consider neurologic causes including cauda equina
- Recent urologic procedures, history of similar prior or recent trauma
- If hematuria is present, place a 22 Fr or larger, ideally a three-way foley, which allows for flushing and irrigation.
- If patients have >1 L retention, recommend maintaining foley to allow bladder to recover from distention.
- Advanced imaging is not routinely required but may be indicated in the post-procedure setting.
- Obtain a careful history to determine underlying cause:
- Post-Obstructive Diuresis
- This is concerning if >200 mL/hour for ≥2 hours, or >3-4 L/day.
- Look out for hypotension, tachycardia, dizziness, syncope, or electrolyte abnormalities (ie, hyponatremia, hypokalemia, hypomagnesemia).
- Clamping of the foley is not routinely recommended.
- The focus of management is monitoring and fluid replacement.
- Tips for Foley Insertion
- Male Patients
- For a patient without hematuria or prior instrumentation, an 18 Fr coudé is a good starting point.
- Use ample lubricant and hold penis taut.
- In cases of narrowing or stricture, attempt a 14 Fr silicone foley for more rigidity.
- If coudé and silicone are both unsuccessful, it is reasonable to consult urology for assistance.
- Female Patients
- Sometimes more difficult because anatomy can be obscured.
- Consider using a bed pan to elevate the pelvis for better visualization.
- In postmenopausal women, the urethra can retract behind the pubic bone; inserting a digit in the vagina may help guide the trajectory of the foley.
- When to Consult Urology
- Several failed attempts
- Signs of trauma
- Suspected urethral injury
- Ongoing obstruction despite foley
- Hematuria not being cleared by irrigation
- Recent urologic surgery
- If necessary, a spinal needle, central line kit, or thora/para kit can be used in conjunction with ultrasound guidance for suprapubic drainage.
- Male Patients
- Troubleshooting a Non-Draining Foley
- Ensure there are no kinks and that tubing is correctly connected.
- Attempt flushing/irrigating.
- Use point-of-care ultrasound to confirm the balloon is in the bladder.
- Discomfort after relieving obstruction may be from bladder spasm; this can be treated with anticholinergics or toradol.
- Disposition
- Start tamsulosin on patients being discharged.
- Consider trial of void within 1 to 3 days for simple reversible causes, but wait at least 1 week in severe cases.
- Could attempt trial of void in the ED for patients willing to learn clean intermittent catheterization so they are able to self-catheterize if they have recurrence at home.
- Counsel regarding daily hygiene of the catheter, checking for kinks, and return precautions.
PEARL: For patients with recent urologic surgery or procedure within the last 3 months, involve urology early for assistance with appropriate management.
Rural Medicine: Not Your Average Fever
Vanessa Cardy, MD, and Lily Muldoon, MD
Dr. Lily Muldoon, an emergency medicine clinician practicing at San Francisco General Hospital, and with the Commonwealth Health Care Corporation in the Northern Mariana Islands, a U.S. territory in the western Pacific, joins EM:RAP to discuss a rare but high-impact case of arthritis.
- Case Summary
- History
- A 17-year-old Pacific Islander male in Saipan with no previous medical history
- Presents during respiratory virus season with 6 days of intermittent fever and progressive difficulty walking
- Pain localized to left knee and right foot/ankle
- Initially attributed to weightlifting and ankle roll
- No recent illness or sexual activity
- Family history of gout (gout is common locally)
- Vitals and Exam
- Temperature 101.3°F, heart rate 100 beats/minute, respiratory rate 19 breaths/minute, BP 137/82 mm Hg, oxygen saturation (SpO2) 98% on room air
- Cardiovascular: tachycardia; no murmur
- Oropharynx: clear, no lesions or swelling
- Abdomen: benign
- Musculoskeletal: left knee mildly swollen
- History
- Initial Differential
- Septic arthritis
- Disseminated gonococcal infection/sexually transmitted infection (STI)-related arthritis
- Crystal arthropathy/gout
- Reactive arthritis
- ARF
- Workup
- X-ray: unremarkable except small knee effusion
- Urinalysis: no infection
- Labs: white blood cell (WBC) count 17,000, C-reactive protein 25 mg/dL, lactate 2.5 mmol/L
- Rapid streptococcus and viral swabs: negative
- Bedside ultrasound-guided arthrocentesis:
- Straw-colored fluid
- Synovial WBC count 36,000 (mostly polymorphonuclear leukocytes [PMNs])
- No crystals
- ECG: Normal sinus rhythm with mildly prolonged PR (~200 ms)
- Re-evaluation
- Reframed evaluation using local epidemiology (high rheumatic fever prevalence)
- Repeat exam targeting ARF findings:
- Erythema marginatum (absent)
- Subcutaneous nodules (absent)
- Advocated to keep ARF on the differential:
- Added throat culture, antistreptolysin O (ASO) titers, and anti–DNase B (send-out tests)
- Patient met 1 major and 3 minor modified Jones criteria
- Hospital Course
- Pediatrics and orthopedics consulted; OR washout initially considered
- Decision: admit and monitor prior to surgical intervention
- Hospital Day 2:
- Blood and synovial cultures negative
- Throat culture positive for group A strep
- PR interval progressed to 280 to 300 ms with Mobitz I AV block
- Echocardiogram normal
- Suspected diagnosis: Acute rheumatic fever
- Management:
- Broad-spectrum antibiotics discontinued
- Intramuscular (IM) penicillin G for eradication of group A Streptococcus
- Naproxen for inflammation
- Long-term monthly IM penicillin G for suppression and biennial echocardiograms to monitor for valvular disease
- Discussion
- ARF remains common in endemic and resource-limited regions (Pacific Islands, sub-Saharan Africa).
- ARF frequently mimics septic arthritis.
- Synovial WBC counts matter; inflammatory range does not equal “septic” by default.
- ARF may occur without classic pharyngitis symptoms.
- Missed or delayed diagnosis leads to rheumatic heart disease and potential need for valve replacements in young adults.
- Key Points
- In endemic settings, septic arthritis vs ARF is a critical diagnostic distinction.
- Prolonged PR interval is an important clue; consider ECG in patients with febrile arthritis.
- Apply the modified Jones criteria systematically.
- Consider strep testing, even without sore throat, in high-risk populations.
- Know your population—what’s rare on the mainland may be common elsewhere.
PEARL: Maintain a broad differential for febrile arthritis and consider acute rheumatic fever when practicing in endemic settings.
Extremity CTA in Trauma
Jessie Werner, MD, and Dennis Kim, MD
Dr. Dennis Kim, Trauma Medical Director at the Victoria General Hospital in Canada, joins Dr. Jessie Werner to discuss when CTA meaningfully changes management in trauma patients with extremity or pelvic fractures. They review hard vs soft signs, the role of ankle-brachial index/arterial pressure index (ABI/API) and Doppler, when pelvic CTA is indicated, and how to approach CTA results in clinical decision-making.
- Introduction / Listener Question
- A listener asked whether routine CTA is necessary for trauma patients with orthopedic extremity or pelvic fractures.
- Orthopedics at their institution felt that hematomas are expected and CTA rarely changes management.
- Trauma surgery felt imaging may still be useful.
- Dr. Kim walks us through this question through a practical, exam-first approach.
- Extremity Vascular Injuries: Hard vs Soft Signs
- Hard signs (historically “straight to the OR,” but in stable patients CTA is now often appropriate first):
- Shock or hypotension
- Rapidly expanding or pulsatile hematoma
- Pulseless or frankly ischemic limb
- Palpable thrill/audible bruit (traumatic arteriovenous [AV] fistula)
- Soft signs (suggest need for further workup: ABI/API, Doppler, serial exams, or CTA):
- Reported large-volume blood loss at the scene
- Hematoma around the fracture (common and expected)
- Pulse discrepancy between extremities
- Hard signs (historically “straight to the OR,” but in stable patients CTA is now often appropriate first):
- Role of ABI/API and Doppler (see CorePendium spotlight for how to perform):
- ABI/API ≥0.9 → major arterial injury essentially ruled out
- ABI/API <0.9 → obtain CTA
- Doppler ultrasound can help identify abnormal flow or traumatic AV fistula.
- ABIs remain an essential bedside skill; Doppler availability is a common challenge.
- CTA in Pelvic Trauma
- Pelvic bleeding is difficult to assess clinically; the exam can be misleading, especially with pelvic binders already in place.
- Early pelvic X-ray is important for fracture detection.
- High-mechanism trauma patients frequently already undergo pan-CT including CTA abdomen/pelvis.
- Only ~10% to 15% of pelvic fractures have arterial bleeding requiring angioembolization (higher when the patient is hypotensive).
- No arterial blush on CTA can reliably exclude major arterial hemorrhage.
- CTA in Extremity Trauma
- CTA is reasonable in stable patients with
- Soft signs (especially pulse discrepancy)
- Mangled extremity or concern for distal ischemia
- High-mechanism polytrauma already getting pan-CT
- Routine CTA for all extremity fractures is not supported.
- CTA is reasonable in stable patients with
- Interpreting CTA Result
- If CTA is positive:
- Involve vascular surgery early (or interventional radiology depending on institutional resources)
- Endovascular options are increasingly used
- Unstable or worsening patients → OR for damage control
- If CTA is negative:
- Very low likelihood of significant vascular injury
- If suspicion persists, reasonable to admit for vascular checks
- If CTA is positive:
PEARL: Routine CTA is not needed for every pelvic or extremity fracture. Start with a good exam, look for hard and soft signs, use ABI/API to screen stable patients, and reserve CTA for patients with abnormal findings or high-risk mechanisms.
Critical Care Mailbag: Stroke Airway
Anand Swaminathan, MD, and Scott Weingart, MD
Swami and Scott discuss when to intubate a critical stroke patient prior to interfacility transfer.
To Intubate or Not?
- In critical stroke patients, interfacility transfer is often required for endovascular clot retrieval.
- Common dilemma: whether or not to intubate the patient for airway protection.
- Glasgow Coma Scale score can be a poor guide (motor scores are often preserved).
- Weigh the risk of deterioration during transfer.
When to Intubate:
- Aspiration risk
- Decreased level of consciousness
- High National Institutes of Health Stroke Score (NIHSS)
- More likely to convert to hemorrhage → decompensation
- Posterior stroke
- Will most likely be intubated before neurointerventional procedure
- Prior to interfacility transfer
- If interfacility transfer hospital is going to intubate patient, then consider intubating before transport
- Benefit of resuscitating patient after intubation and before transport to ensure “stable” transport
- Prevention of decompensation en route
How to Intubate?
- Rapid sequence intubation (RSI) = most likely first-pass airway.
- Consider intubating with the head of the bed at 30°.
- Use the position that will lead to best first-pass intubation,
- The key is to not let patients get hypoxemic, hypercarbic/hypocarbic, or hypotensive!
- Maintain tight BP control:
- SBP 140-180 mm Hg, MAP 70-90 mm Hg
- Augment to 160 mm Hg with vasopressors (norepinephrine) before intubation.
- Don’t use intravenous (IV) fluids as these patients are not usually fluid down.
- Most patients are hypertensive:
- >180 mm Hg = danger zone for hemorrhagic conversion
- 180 mm Hg is the magic number for ischemic stroke for either thrombolytics or large vessel occlusion (LVO)
- SBP 140-180 mm Hg, MAP 70-90 mm Hg
- Do NOT overventilate patient:
- End-tidal CO2 should be 35-45
- Low CO2 = vasoconstriction = worse outcome
- Consider 1:1 ketamine/propofol sedation.
- Etomidate also an option
- Paralytic = rocuronium (1.2-1.5 mg/kg)
- The patient remains paralyzed during transport.
- Avoid high doses.
- Can consider succinylcholine if neurointerventionalists care about neuro exam
- Institution specific
- Post-intubation Sedation/Analgesia
- Propofol/fentanyl
- Have norepinephrine hanging in the room in case BP drops
- Consider remifentanil or dexmedetomidine as alternatives if available
- Propofol/fentanyl
- Post-intubation Care
- Place a nasogastric tube.
- Hyperoxia is dangerous; aim for 95% to 98%.
PEARL: Have a low threshold to intubate critical stroke patients to protect the airway before transport; then stabilize them prior to transport. The key is to avoid hypoxemia, hypercarbia/hypocarbia, and hypotension!
NEJM
REBELEM
REBEL Core Cast 149: Review of Corticosteroids in Community-Acquired Pneumonia
- 💉 Hydrocortisone Saves Lives:
The 2023 Cape Cod Trial (NEJM) showed a clear mortality benefit and reduced need for intubation in severe CAP patients treated with hydrocortisone. - 📊 Guidelines Are Catching Up:
The SCCM (2024) and ERS now recommend steroids for severe CAP, while ATS/IDSA updates are still pending. - 🔥 Redefining “Severe”:
Patients requiring high FiO₂ (>50%), noninvasive or mechanical ventilation, or PSI >130 meet criteria for steroid therapy — even outside the ICU. - 🍬 Main Risk = Hyperglycemia:
Elevated glucose was the most consistent adverse effect, but rates of GI bleed and secondary infection were not increased. - 🧭 Early, Targeted Use Matters:
Start hydrocortisone within 24 hours of identifying severity — especially in patients with high CRP (>150) or strong inflammatory response. - Dose: Hydrocortisone Continuous Infusion 200mg/d or 50mg q6h if continuous infusion not possible
- Hey, this is Swami, one of the ED attendings. I’m calling for an ortho consult.
- I’m calling about a patient with a suspected septic knee. I need you to evaluate for operative management.
- When there is push back:
- Help me understand your concern about seeing this patient
- To be clear, I’m concerned this is septic arthritis and needs ortho evaluation. If you don’t feel you’re the right service, who should be—rheum, medicine, or another surgical team
- I’m worried we’re missing something time-sensitive. If this were your family member, what would you want us to do next
- We’re at an impasse and the patient needs a decision. I’m escalating to clarify ownership and ensure timely care
