Academic Emergency Medicine
No articles this month
Annals of Emergency Medicine
Predictors of Laryngospasm During 276,832 Episodes of Pediatric Procedural Sedation
- Laryngospasm occurs in 3.3/1000 cases of Ketamine
- Among patients with laryngospasm, the resulting outcomes included desaturation less than 70% for more than 30 seconds (19.7%), procedure not completed (10.6%), emergency airway intervention (10.0%), endotracheal intubation (5.3%), unplanned admission/increase in level of care (2.3%), aspiration (1.1%), and cardiac arrest (0.2%).
Pediatric Procedural Sedation and Laryngospasm: How Much Should I Worry?
- Laryngospasm is rare—approximately 3 in 1,000 sedations performed outside the operating room, and this number may even be lower in the ED setting.
- Serious outcomes are very rare but do occur.
- Risk factors to be aware of are as follows: young age (<1 year), patients with upper respiratory tract infections, patients categorized as ASA class III or higher, procedures involving the upper airway, and sedation with a combination of ketamine and propofol. It is uncertain whether these factors are directly translatable to ED sedations; however, knowing these patient- and medication- related risk factors can help inform emergency physicians in
- sedation planning.
- The findings of Cosgrove et al1 support continued confidence in ketamine as a single agent to provide safe and effective sedations for children.
- Laryngospasm associated with procedural sedation is a rare event regardless of the clinical setting, drug administered, or procedure performed—however, the risk is not zero—reinforcing that all sedation clinicians must be skilled in airway rescue.
- .48% incidence of invasive bacterial infection among 2-6 month olds with fever.
- Only 4 positive CSF cultures (1/5250).
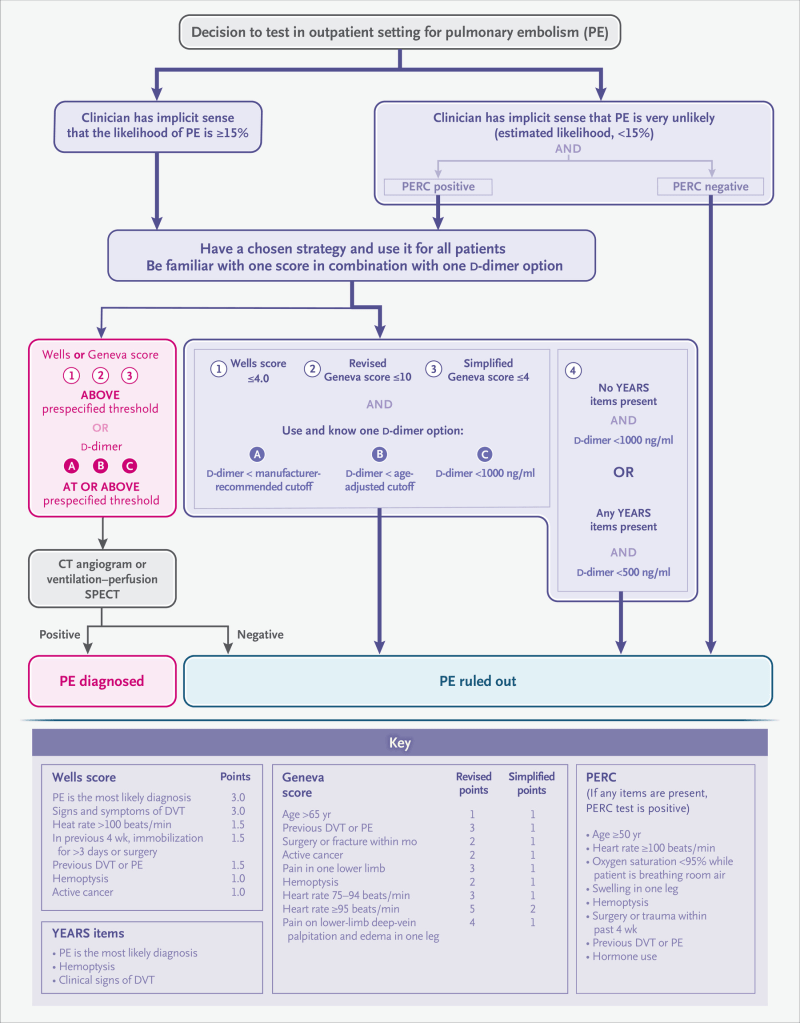
- Awaiting a validation study but suggests that d-dimer testing for DVT will go the way of PE testing where low pre-test probability allows for higher test threshold D-dimer levels.
BMJ
Circulation
CJEM
EMCRIT
EMCrit 338 – End of Year Question & Answer Session
Emergency Medicine Journal
EMRAP
Pigtail Catheter for Pneumothorax- Weingart
First10em
Laceration evidence part 7: Aftercare instructions
- Can wounds get wet?
- Very low level of evidence, but it is probably safe to get wounds wet early after repair, and keeping them clean with soap and water makes physiologic sense.
- Do dressings help?
- There does not seem to be any evidence that dressings improve healing after acute lacerations. It makes sense to use a dressing for comfort, and to absorb blood and exudate in the first 12-24 hours after repair. Obviously, patients can continue to use dressings for aesthetic or comfort reasons if they prefer.
For such a common problem in emergency medicine, there is a striking paucity of evidence to guide our care of lacerations. Nothing I found allowed for definitive conclusions, so clinical judgment and shared decision making are, like always, necessary.
Personally, I tell patients:
- A dressing isn’t required, but you probably want one for the first 24 hours, as some bleeding may still occur. After that point, I would suggest applying a dressing if you are in an environment where the wound might become contaminated, or if you prefer one for cosmetic sake, but I want you to remove the dressing every day to check for signs of infection.
- It is fine to get the wound wet, and in fact I like the idea of keeping the area clean with soap and water. However, I would avoid obviously contaminated water sources, like lakes and public pools until the wound is completely healed.
- Topical antibiotics probably aren’t necessary. They might prevent small pimple-like infections, but there is a risk of an allergic reaction. You can use an over-the-counter preparation if you like.
- I don’t think there is any evidence that vitamin E or expensive scar creams help. Applying a very light layer of vaseline during the first week, to keep the wound moist as it heals, might make sense.
JAMA
- Among US primary care physicians in 2019, MIPS scores were inconsistently associated with performance on process and outcome measures. These findings suggest that the MIPS program may be ineffective at measuring and incentivizing quality improvement among US physicians.
Journal of Emergency Medicine
None
Lancet
None
NEJM
Prescribing Opioids for Pain — The New CDC Clinical Practice Guideline
PEDIATRICS
None
REBELEM
Pigtail Catheter vs Large Bore Chest Tube for Pneumothorax
- We agree with the author’s conclusion. PC performed as well as LBCT in terms of successful drainage and was associated with fewer complications, decreased drainage duration, and decreased length of hospital stay, driven by data on spontaneous pneumothorax.
REBEL Core Cast 92.0 – Perichondritis
- Most common organism is pseudomonas so must treat with fluoroquinolones.
- Inpatient treatment is required if an abscess is suspected.
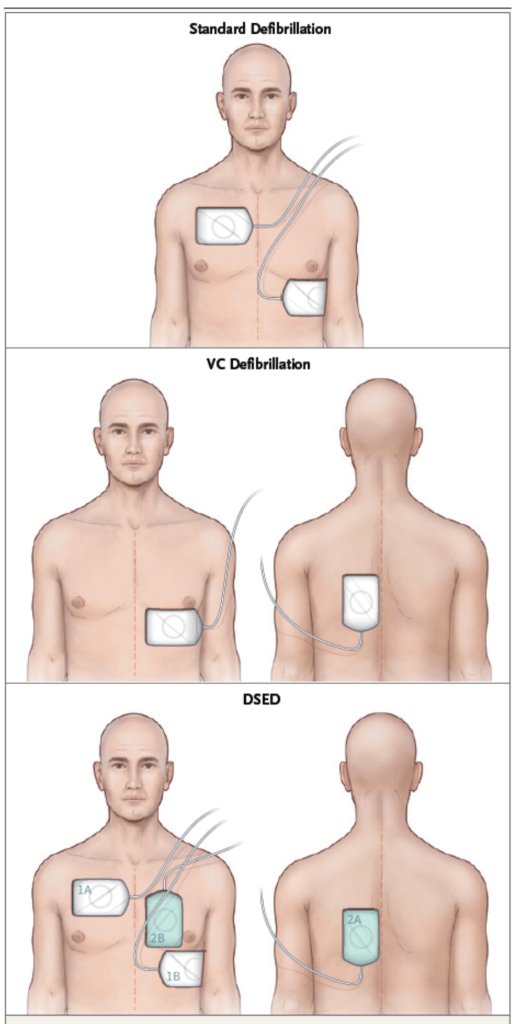
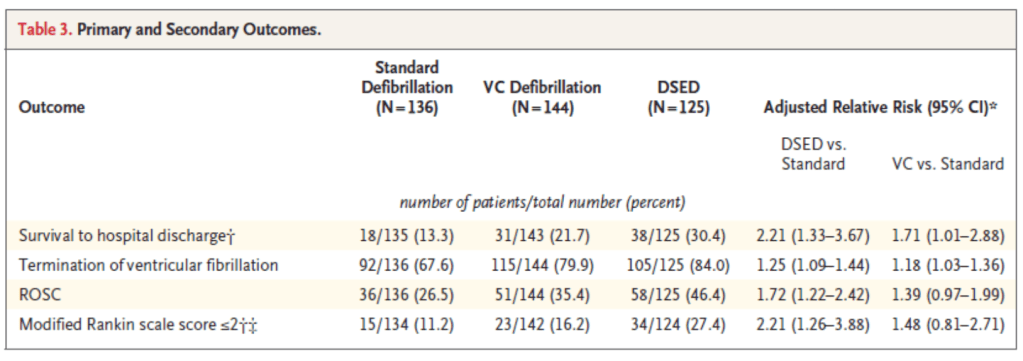
REBEL Cast Ep113: Defibrillation Strategies for Refractory Ventricular Fibrillation
- Double sequential defibrillation and vector change defibrillation are both feasible treatments for refractory ventricular fibrillation with the later being more practical and cost effective in the prehospital setting. . However, until additional evidence presents itself, the use of double defibrillation on a case-by-case basis should be considered based on operational feasibility such as institution/agency policies, and availability of resources.
7d vs 14d of Antibiotics in Afebrile Men with UTI
- 7d of abx for stable afebrile males with UTI
Resuscitation