Anticoagulant/Antiplatelet Guidance
Highlights
- INR not recommended unless patient is on anticoagulants (per UpToDate) or requires admission for ongoing bleeding (my recommendation).
- Exam starts by having patient blow out all clots, spray of afrin, application of topical anesthetic in cotton ball, and firm squeezing x 10 minutes.
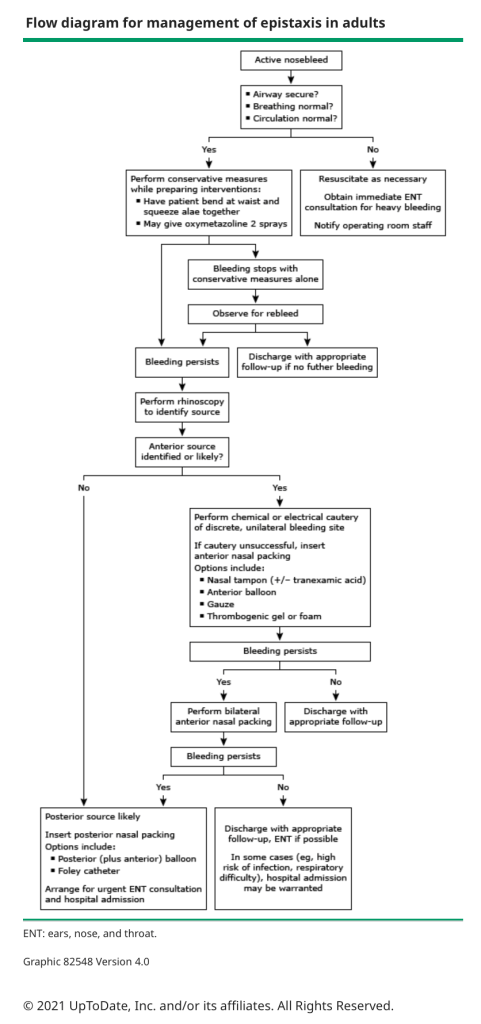
- If still bleeding, try cautery.
- If still bleeding, try anterior pack on one side.
- If still bleeding, try bilateral anterior packs (bilateral anterior packing controls 90-95% of bleeds, if patient still bleeding, posterior source more likely).
- If still bleeding, consult ENT and place anterior/posterior pack.
- If still bleeding, ENT decides between endoscopic ligation and IR embolization.
- Confirm your ED has a posterior balloon packing device: ideally a 9 cm Rhino Rocket (7.5cm Rhino Rocket can be used for posterior packing but it does not have a second balloon dedicated to the sphenopalatine artery bleeds), or the Epistat or T-3100 Storz.
- Most posterior bleeds need admission and cardiac monitoring (not because of the hypothetical nasopulmonary reflex which is no longer supported by best evidence), but because these patients are at higher risk for hemorrhage and aspiration.
Anatomy
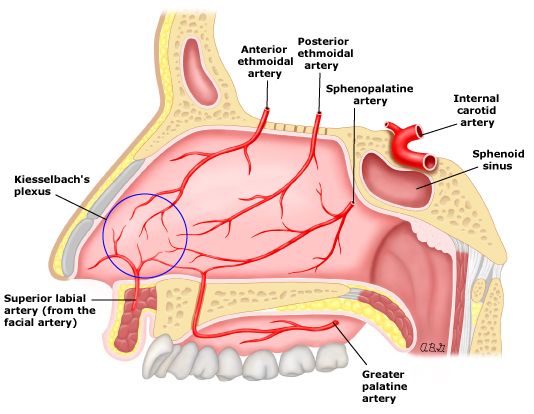
- Epistaxis divided into anterior (90-95%) and posterior (5-10%) bleeds.
- Anterior- 5 arteries converge in the anterior septum to form Kiesselbach’s plexus.
- Posterior- 2 arteries (sphenopalatine and internal carotid) can cause posterior bleeds.
Etiology
- Mucosal irritation and trauma most common
- Recreational cocaine use
- Nasal sprays
- Carotid aneurysm- especially after prior head and neck surgery or trauma
- Foreign body (consider when history of purulent drainage)
- Anticoagulation: anticoagulated patients commonly have epistaxis but need for reversal is rare according to UPTODATE (1.5 per 1000 patient-years).
- Hypertension- weak association, most likely due to it’s long term vasculopathic effects, may prolong bleeds rather than cause them.
- Bleeding disorders (epistaxis is the most common presenting symptom among patients with hereditary hemorrhagic telangiectasia (Osler-Weber-Rendu disease), also thrombocytopenia, von Willebrand’s disease, hemophilia, etc.
- A bleeding diathesis should be considered in the patient with recurrent spontaneous epistaxis.
- Neoplasm
- Aspirin has a weak association with epistaxis, NSAIDS have no increased risk.
Evaluation
- History:
- ask about risk factors above
- Labs
- INR not recommended unless patient is on anticoagulants (per UpToDate) or being admitted (per me)
- CBC not recommended unless patient has massive or prolonged hemorrhage or physician concern for thrombocytopenia (e.g. history of ITP, petechiae on exam) or being admitted.
- Exam Preparation
- Have patient blow nose to remove clots
- 1 of spray of oxymetazoline (afrin) to affected nares
- Place cotton ball/gauze soaked with 3 cc of 1-2% lidocaine with epinephrine or 4% cocaine in affected nares
- Have patient squeeze nares with soaked cotton ball x 10 minutes, while leaning head forward to avoid pooling of blood in throat

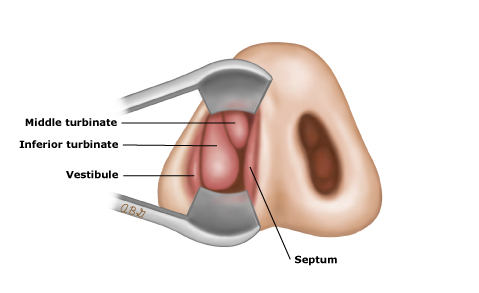
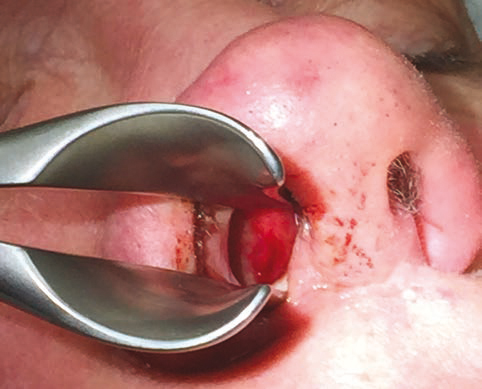
- Speculum Exam
- Remove cotton ball
- Use a nasal speculum to evaluate turbinates and septum for source of bleeding
Treatment
- Cautery
- Either chemical (silver nitrate) or electrical (never tried but per UpToDate works equally well), is first line if anterior bleeding confirmed.
- Though silver nitrate requires moisture to act, it will work only on a relatively bloodless surface; the bleeding point itself cannot be cauterized until hemostasis is achieved either through proximal cautery, vasoconstrictive agents such as afrin drops or tamponade from manual pressure.
- Confirm patient is anesthetized, otherwise too painful
- Area should be cauterized from proximal periphery then move to center of bleeding.
- Only cauterize for a few seconds to avoid necrosis (also avoid cautery to both sides of the septum).
- Nasal packing
- May require reapplication of local anesthesia
- May require opiates (fentanyl) and/or anxiolytics (versed)- patient preference.
- 3 options: Rhino Rocket, Merocel Tampon, Balloon
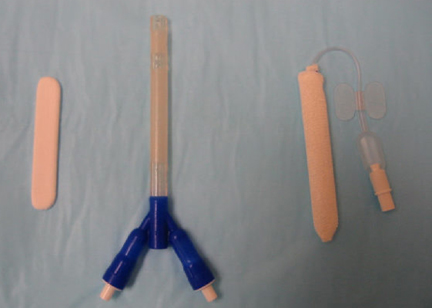
- Rhino Rocket (RR)
- 5 cm size is for anterior bleeds, 7.5 and 9 cm are for posterior bleeds (but 7.5 cm RR does not have a designated posterior balloon for the posterior sphenopalatine artery, unclear if this limits its efficacy, I couldn’t find any head to head comparisons).
- Should be soaked in sterile water x 30 seconds but not saline or lubricants or topical antibiotics because it degrades the mesh.
- Inflate balloon with air using a 20ml syringe, inflate until cuff is round and firm (after 10-15 min reassess to see if more air is required).
- Two trials found RR and Nasal tampons are equally effective but RR cause less discomfort and are easier to insert.
- Nasal Tampon (Merocel)
- Coat with antibiotic ointment to facilitate insertion into the nares.
- Rhino Rocket (RR)
- TXA
- Due to the pain of nasal packing, a 2013 small trial of possible benefit from cotton balls or gauze soaked in 5 ml of TXA (100mg/ml IV preparation) was received with enthusiasm.
- Recent studies have been less promising.
- a 2018 Cochrane meta-analysis by Joseph concluded “we are uncertain whether or not topical tranexamic acid is effective in stopping bleeding in the 10-day period after a single application”.
- A 2019 meta-analysis of three small trials (two of which used oral TXA) involving 408 patients found no difference in short term bleeding.
- The largest and most recent multicenter study, NoPAC, published in the June 2021 issue of Annals of EM found no benefit from topical TXA.
- UpToDate has TXA in their treatment algorithm as a +/- option in combination with nasal tampons (despite their acknowledgement that this has never been studied).
- Many centers use rhino rockets with a mesh covering that degrades when saline or lubricants are applied, so unclear if TXA is acceptable to apply to a rhino rocket.
- Bottom-line: TXA still used at many centers as an initial measure with cotton balls or gauze or Merocel tampons, certainly reasonable to try if you have found success with TXA or if recommended at your institution, but the pendulum of evidence may be swinging away from significant benefit.
- Persistent Bleeding
- Pack the other nares, bilateral pack works in 90-95% of cases.
- If still bleeding, need ENT consult and posterior packing.
- Posterior Packing
- 7.5cm Rhino Rocket is advertised as a posterior packing device, but it only has a single balloon for the entire nares so unclear if it adequately tamponades the posterior nasal cavity.
- 9cm Rhino Rocket now available, designed for posterior bleeds with two balloons, but may not yet be in your ED, so ask for it to be ordered.
- Other posterior balloon options include the Epistat and T-3100 Storz.
- Inflate the posterior balloon first (for Rhino Rocket the posterior cuff is marked by a green line on the swallow guard as shown below, inflate with air)
- Retract the catheter gently until it lodges against the posterior choana in the nasopharynx.
- Once the posterior balloon is seated, inflate the anterior balloon.
- Admit, cardiac monitor, see below under disposition.
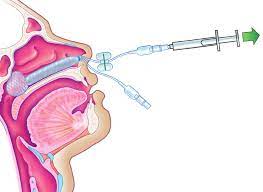
Using a 20 cc syringe, slowly inflate the posterior balloon with air only inside the patient’s nose. The balloon will conform to the anatomy of the posterior nasal cavity.
- Embolization or Ligation
- If bleeding persists despite posterior packing, ENT consult necessary to determine if patient should get IR embolization (4% risk of CVA) or endoscopic ligation of the sphenopalatine or anterior ethmoidal artery (similar efficacy 90%).
- Anticoagulation reversal
- Per NEJM 2021 article, consider actions below if posterior bleed, hemodynamic instability or >2g drop in hemoglobin or transfusion of 2 units of PRBCs.
- Consult specialist in anticoagulation or cardiovascular medicine
- Consider temporary discontinuation of anticoagulant or antiplatelet medication
- Consider treatment with reversal agent
- Consider platelet transfusion
- Per NEJM 2021 article, consider actions below if posterior bleed, hemodynamic instability or >2g drop in hemoglobin or transfusion of 2 units of PRBCs.
Disposition
- Admission Criteria
- Most patients with posterior bleeds need hospitalization and cardiac monitoring (not because of the hypothetical nasopulmonary reflex which is no longer supported by best evidence), but because these patients are at higher risk for hemorrhage and aspiration.
- Anterior bleeds who cannot be relied on to return or follow-up or who have significant comorbidities.
- Discharged Patient Follow-up
- If vital signs and respiratory function remain normal after anterior packing, the patient may be safely referred for specialist follow-up in 24 to 48 hours, with advice to present to an emergency department sooner if bleeding recurs.
- If specialist follow-up cannot be achieved in 24-48 hours, the packing should be removed in the ED in 1-2 days.
- Rhino Rockets are easy to remove by deflating the balloons but Merocel tampons should be rehydrated with saline drops prior to removal for patient comfort.
- Antibiotic Prophylaxis
- No evidence that they reduce the risk of toxic shock (1.6/10000 packings) or sinusitis.
- UpToDate does not recommend, although they say it can be considered if DM, immunocompromised or advanced age.
- Many ENTs recommend antibiotic prophylaxis, consider institutional norms and patient preference in your decision.
- Anticoagulant and Antiplatelet Guidance
- UpToDate says folks who are therapeutic on their anticoagulant and in whom hemostasis is achieved can continue on their regimen.
- If patient has recurrent visits to ED for bleeding the temporary cessation of the AC or antiplatelet agent should ideally be a shared decision between the patient and the prescribing physician.
- Preventive Therapy
- Anterior bleeds should be advised to sleep in a humidified environment.
- For patients without packing, topical antibacterial (eg, mupirocin) or bacteriostatic (eg, bacitracin) ointment may be gently applied to the nasal mucosa with a cotton-tipped swab TID in an attempt to prevent recurrence.
- Directing nasal medication sprays away from the septum may decrease the risk of epistaxis.
