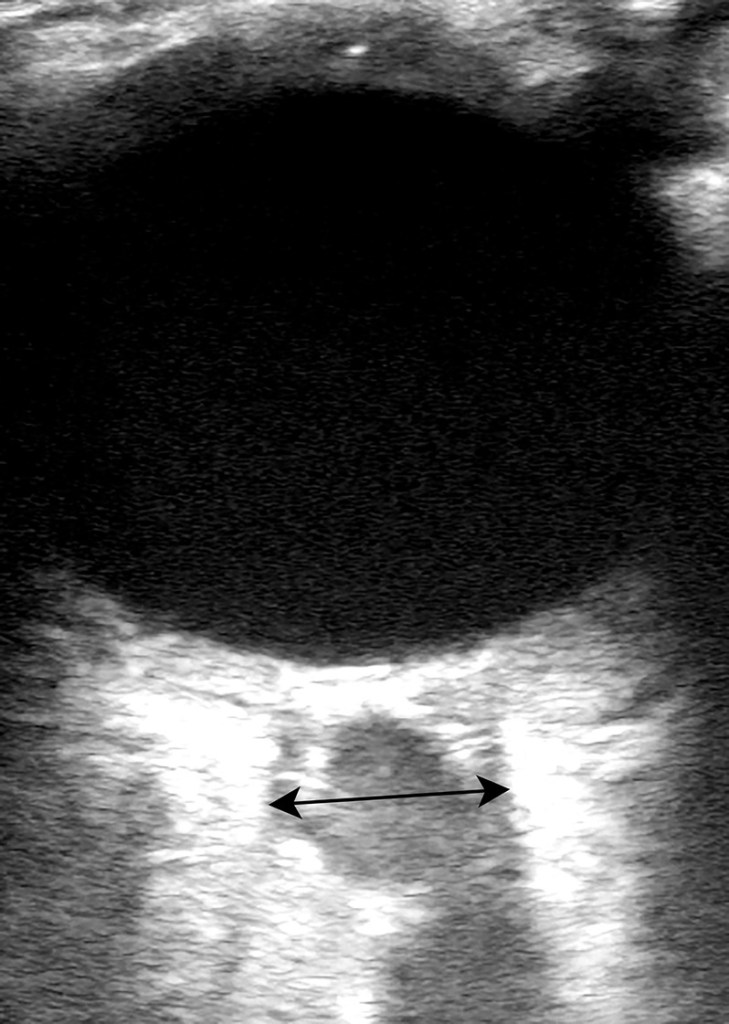
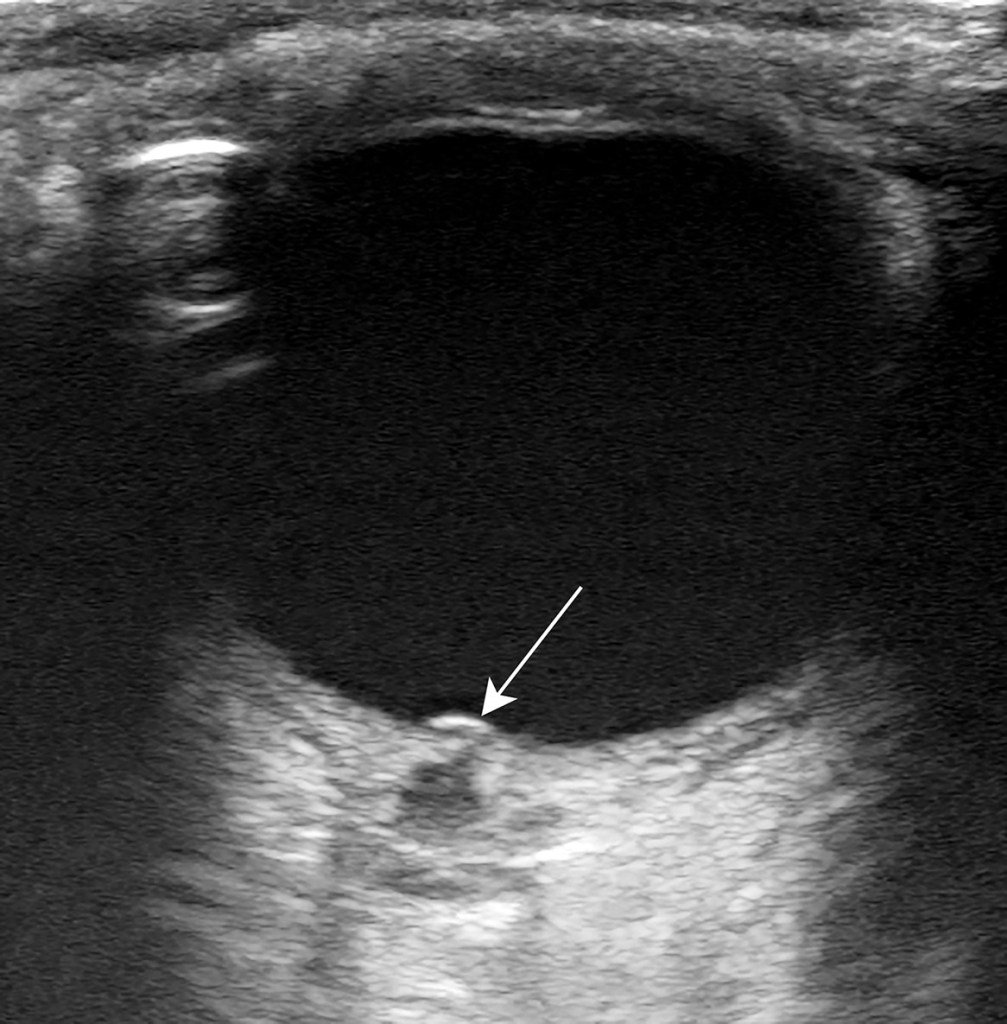
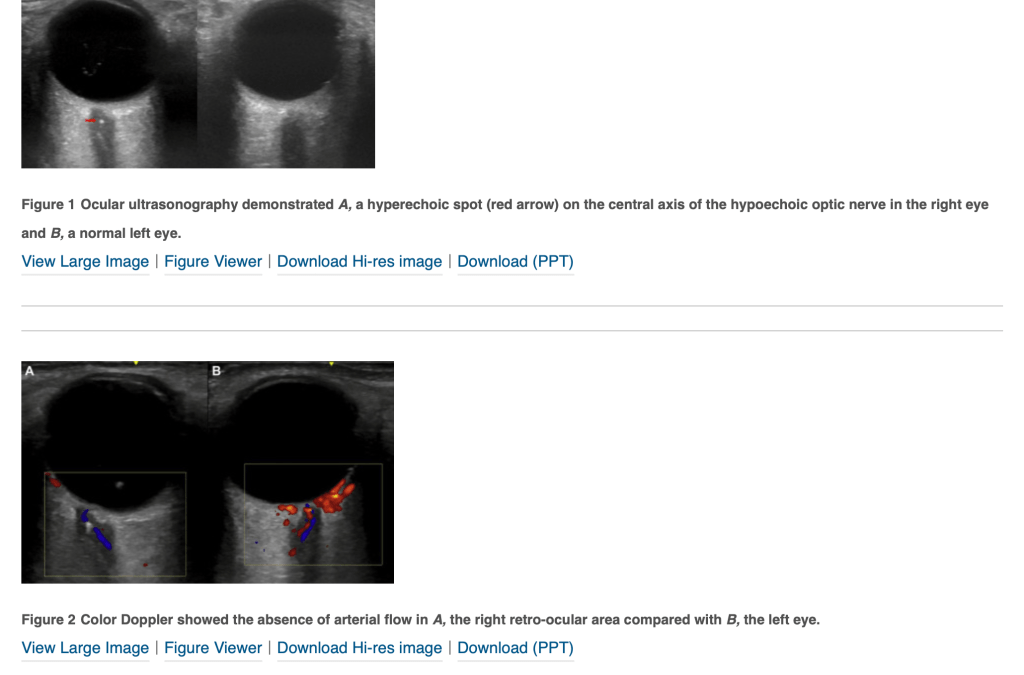
A healthy 39-year-old man presented to the emergency department with 2 days of nontraumatic severe left eye pain and progressive visual loss to the point of blindness. Upon physical examination, the patient reported only flashes of light in the left eye, with sluggish pupillary response and painful extraocular movements. The result of slit lamp examination was unremarkable, and ocular pressures were normal. The result of right eye examination was unremarkable. An emergency physician conducted point-of-care ocular ultrasound, demonstrating evidence of papilledema and optic nerve inflammation
6.5mm wide optic nerve, ill-defined borders suggest inflammationBulge of the optic disc
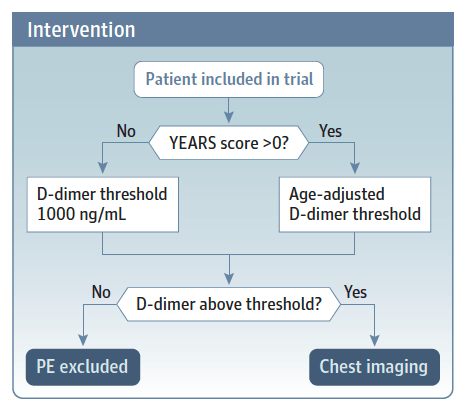
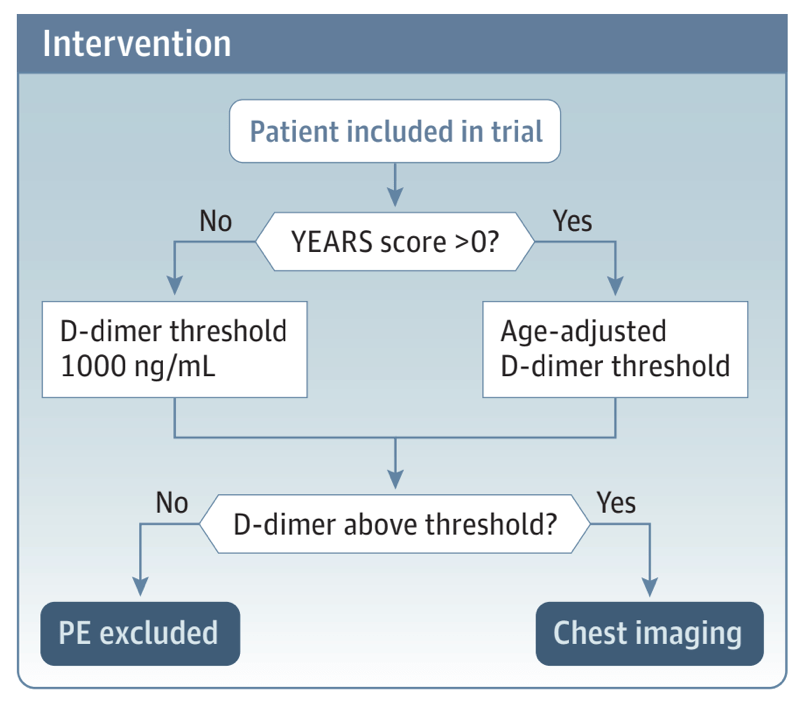
DVT was considered excluded without further testing by Wells low clinical pretest probability and D-dimer <1000 ng/mL or Wells moderate clinical pretest probability and D-dimer <500 ng/mL. All other patients had proximal ultrasound imaging. Repeat proximal ultrasonography was restricted to patients with initially negative ultrasonography, low or moderate clinical pretest probability, and D-dimer >3000 ng/mL or high clinical pretest probability and D-dimer >1500 ng/mL.
Of the 1275 patients with no proximal DVT on scheduled testing who did not receive anticoagulant treatment, eight (0.6%, 95% confidence interval 0.3% to 1.2%) were found to have venous thromboembolism during follow-up. Compared with a traditional DVT testing strategy, this diagnostic approach reduced the need for ultrasonography from a mean of 1.36 scans/patient to 0.72 scans/patient (difference −0.64, 95% confidence interval −0.68 to −0.60), corresponding to a relative reduction of 47%.
Konda SR et al. Computed tomography scan to detect traumatic arthrotomies and identify periarticular wounds not requiring surgical intervention: an improvement over the saline load test. J Orthop Trauma 2013; 27: 498-504.
The requirement for tracheal intubation or mortality within 30 days was significantly lower with CPAP (36.3%; 137 of 377 participants) vs conventional oxygen therapy (44.4%; 158 of 356 participants) (absolute difference, −8% [95% CI, −15% to −1%], P = .03), but was not significantly different with HFNO (44.3%; 184 of 415 participants) vs conventional oxygen therapy (45.1%; 166 of 368 participants) (absolute difference, −1% [95% CI, −8% to 6%], P = .83).
Proning not studied but probably more important than oxygen delivery system
This limited study found no statistically significant difference in stability of oral FXi related ICH after the administration of AA or 4F-PCC. However, the inherent potential bias and small participant numbers limit generalizability and therefore larger prospective studies are needed. 4F-PCC is cheaper and more widely available than AA ($5670/patient, compared to $22,120-$49,500/patient);
The 90-day incidence of venous thromboembolism among patients discharged from the ED with ankle fractures requiring immobilization was 1.3%. These patients had a 5.7- to 6.3-fold increased hazard compared to matched controls. Certain patients immobilized for ankle fractures are at higher risk of venous thromboembolism, and this should be recognized by emergency physicians.
Among preschool-aged children with gastroenteritis seeking ED care, oral ondansetron administration was associated with a reduction in index ED visit intravenous fluid administration; it was not associated with intravenous fluids administered within 72 hours, hospitalization, or vomiting and diarrhea in the 24 hours following discharge.
The findings suggest that SSRIs provide high rates of remission with low risk of adverse events for the treatment of panic disorder. Among SSRIs, sertraline and escitalopram were associated with high remission and low risk of adverse events. The findings were, however, based on studies of moderate to very low certainty levels of evidence, mostly as a result of within study bias, inconsistency, and imprecision of the findings reported.
Results Of the 1150 patients included in this study, 820 (71.3%) had no history of CAD, 97 (8.4%) had index AMI and 123 (10.7%) had 30-day MACE. In patients with no prior history of CAD, HEAR ≤ 1 identifi ed 202 (24.6%) of patients as very low risk for 30-day MACE with 98.4% (95% CI 91.6ñ 99.9%) sensitivity. Among all patients, HEAR ≤ 1 identifi ed 202 (17.6%) patients as very low risk for 30-day MACE with 99.2% (95% CI 95.6ñ 99.9%) sensitivity. Conclusions A HEAR score ≤ 1 can identify more than 17% of all patients as very low risk for index AMI and 30-day MACE and unlikely to benefi t from troponin testing. Broad implementation of this strategy could lead to signifi cant resource savin
A “Best BETs” in 2014 concluded, “There is no scientific evidence for the routine use of nasogastric tubes in adults with small bowel occlusion.”
They are routinely rated as the most painful procedure performed in the ED.
Bottom line: Nasogastric tubes clearly do harm in terms of patient discomfort and there is no evidentiary basis for their role in the modern management of SBO. This doesn’t mean that nasogastric tubes play no role. They may be useful in patients with vomiting refractory to antiemetics or patients with distended stomachs. We simply do not know who benefits from them and instead of being a routine part of care, selective use makes more sense.
Rib fractures that are not seen on a chest radiograph are generally not clinically significant (2/3 of rib fxs seen on CT are missed on plain film)
Fractures of the first and second ribs place patients at high risk for vascular injuries. If seen on a chest radiograph, CT angiography of the neck should be performed.
When read by a radiologist, rib series are not more sensitive than a standard two-view chest x-ray, and result in twice the amount of ionizing radiation to the patient.
Among nonhospitalized patients who were at high risk for Covid-19 progression, a 3-day course of remdesivir had an acceptable safety profile and resulted in an 87% lower risk of hospitalization or death than placebo.
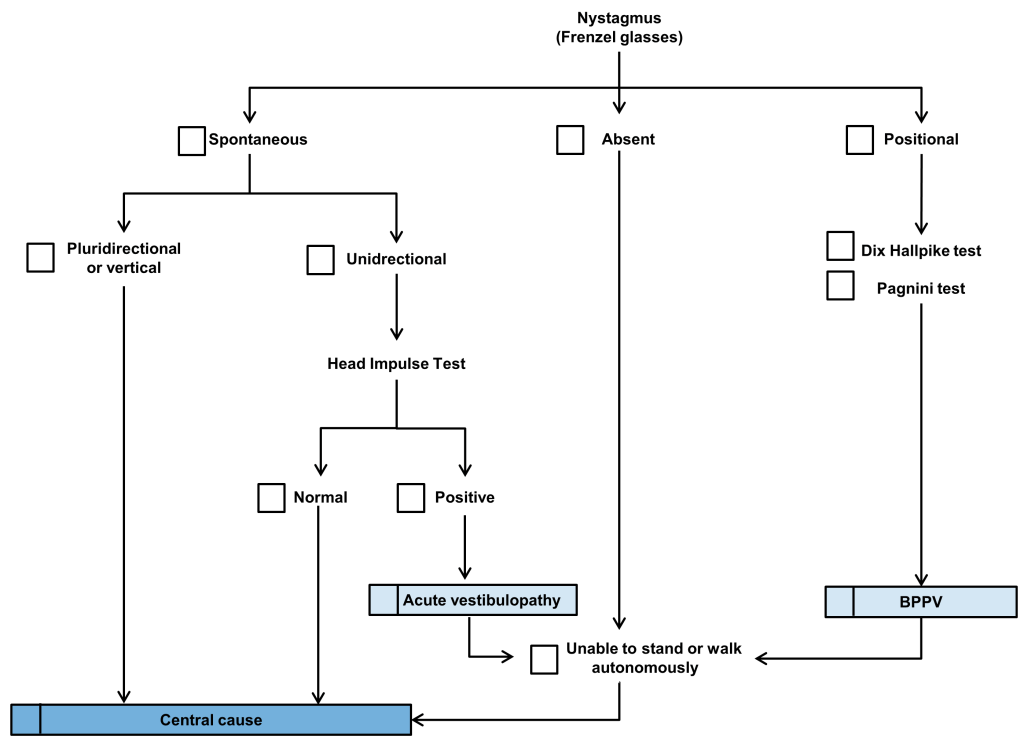
HINTS and STANDING tests reached high sensitivities at 97% and 94% and NPVs at 99% and 98%, respectively. The ABCD2 score failed to predict half of central vertigo cases and had a sensitivity of 55% and a NPV of 87%. The STANDING test was more specific and had a better positive predictive value (PPV; 75% and 49%, respectively; positive likelihood ratio [LR+] = 3.71, negative likelihood ratio [LR–] = 0.09) than the HINTS test (67% and 44%, respectively; LR+= 2.96, LR– = 0.04).
Conclusions: In the hands of EPs, HINTS and STANDING tests outperformed ABCD2 in identifying central causes of vertigo.
Standing Test
Hot off the press: Self-obtained vaginal swabs for sexually transmitted infection testing
For the primary outcome, self-swabs had a sensitivity of 95% (95% CI= 88% to 99%) for the detection of NG/CT when com-pared to provider performed swabs. Secondary outcomes revealed an excellent kappa of 93%, and self-swab sensitivities for NG and CT were 97% and 94%, respectively
2% annual graduate medical education growth, 3% annual emergency physician attrition, 20% encounters seen by a nurse practitioner or physician assistant, and 11% increase in emergency department visits relative to 2018. This scenario would result in a surplus of 7,845 emergency physicians in 2030.
Clinical protocol for ED patients with moderate to severe alcohol use disorder using oral naltrexone and extended-release intramuscular naltrexone together with substance use navigation. Identification of alcohol use disorder, a brief intervention, and initiation of naltrexone resulted in a 15% follow-up rate in formal addiction treatment. Future work should prospectively examine the effectiveness of naltrexone as well as the effect of substance use navigation for ED patients with alcohol use disorder.
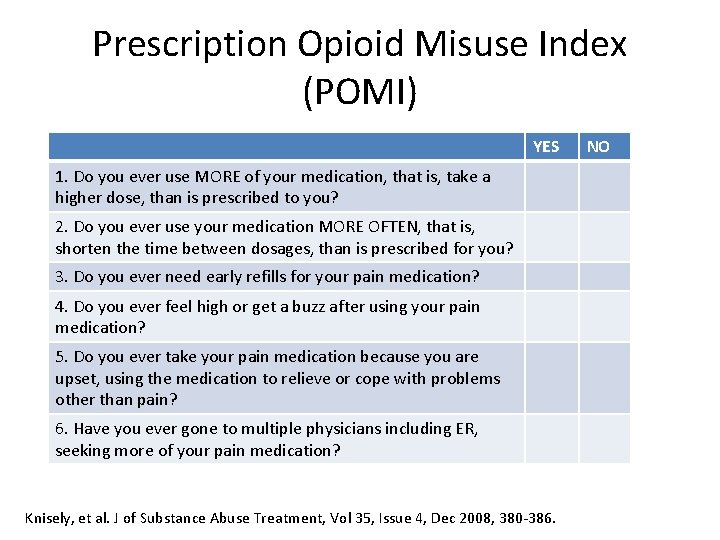
Low-threshold ED buprenorphine treatment implemented with a harm reduction approach and active navigation to outpatient addiction treatment was successful in achieving buprenorphine treatment for opioid use disorder in diverse California communities.
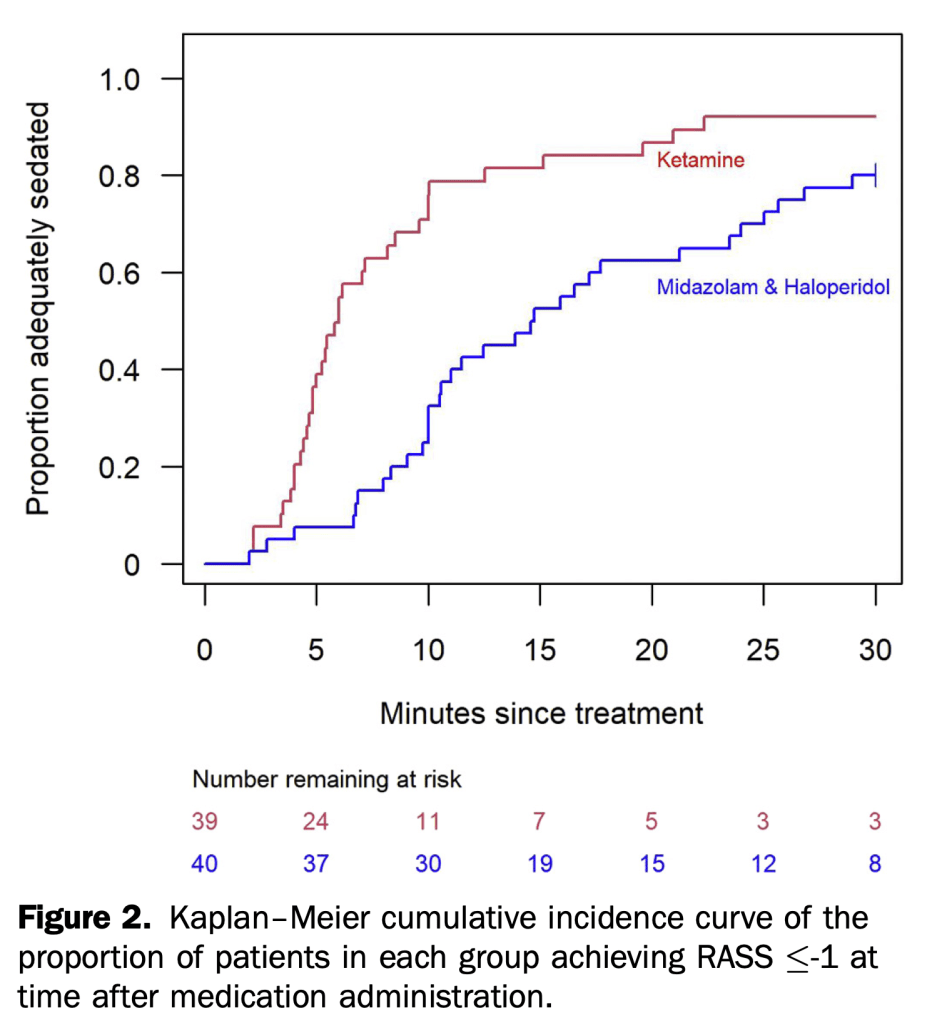
In this randomized controlled trial of 80 adults, the median time to adequate sedation was significantly faster for ketamine 5mg/kg IM versus Midazolam 5mg IM/haloperidol 5mg IM (6 versus 15 minutes, respectively).
Intubation occurred in 34 (34.3%) randomized to high-flow oxygen therapy and in 51 (51.0%) randomized to conventional oxygen therapy (hazard ratio, 0.62; 95% CI, 0.39-0.96; P = .03). The median time to clinical recovery within 28 days was 11 (IQR, 9-14) days in patients randomized to high-flow oxygen therapy vs 14 (IQR, 11-19) days in those randomized to conventional oxygen therapy (hazard ratio, 1.39; 95% CI, 1.00-1.92; P = .047).
Among Medicare beneficiaries 65 years or older with atrial fibrillation, treatment with rivaroxaban compared with apixaban was associated with a significantly increased risk of major ischemic or hemorrhagic events.
Janapala RN, et al. Efficacy of Topical Tranexamic Acid in Epistaxis: A Systematic Review and Meta-Analysis. Am J Emerg Med. Nov 2021.
This meta-analysis highlights the importance of a head-to-head comparison of first line agents in the treatment of epistaxis. Knowing the efficacy of topical TXA compared to other first line vasoconstrictors from this study, it’s not an unreasonable approach to use it as a first line agent. The use of TXA in epistaxis should be left to the discretion of the emergency physician. Although, the NoPAC trial showed no difference in the use of topical TXA, that study was different in that direct pressure plus phenylephrine was used and only after failure were patients randomized to TXA vs placebo. Maybe a better strategy would be direct pressure PLUS TXA as a 1st line approach to epistaxis as it appears from this study that it does a better job in bleeding cessation when compared to other vasoconstrictors.
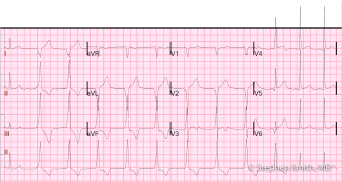
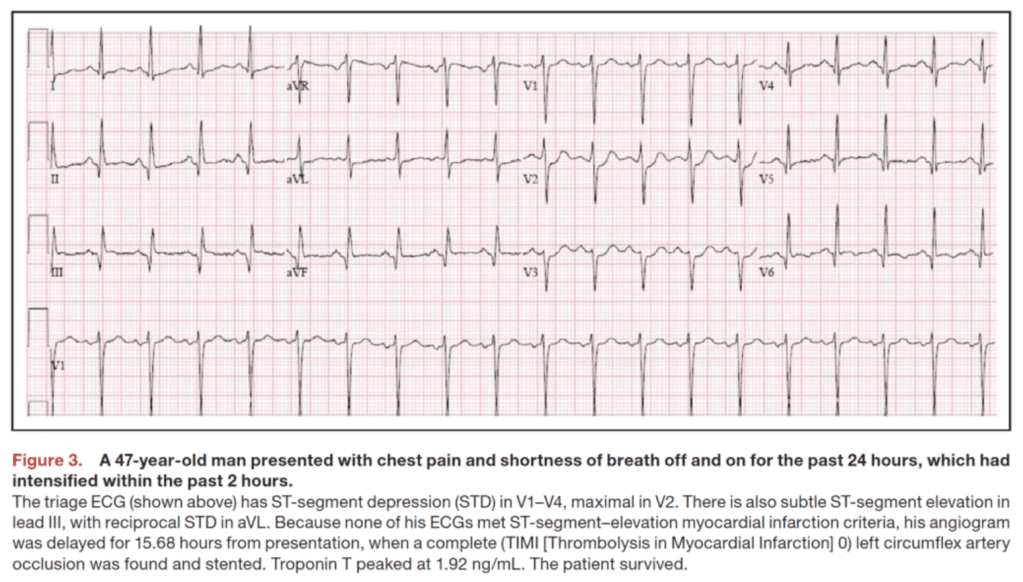
Not all occlusion myocardial infarctions (OMIs) present with classic ST-segment elevation (We have covered this on REBEL EM Before HERE, HERE, and HERE). OMIs of the “posterior” and “lateral” walls are the most commonly missed, with >50% of left circumflex occlusions (Posterior and lateral walls suppled by the circumflex artery)not receiving emergent reperfusion. These misses occur because isolated posterior OMIs do not result in classic ST-elevation ECG changes. Instead, posterior OMI results in ST depression which is maximal in V1 to V4 (alternatively, ST-depression of subendocardial ischemia is maximal in V5 to V6).
In patients with symptoms suggestive of ACS in the ED, the specificity of STDmaxV1-4 was 97% for the diagnosis of posterior OMI and 96% for posterior OMI requiring PCI. This finding of STDmaxV1-4 is both highly accurate and sufficient without the need for routine posterior leads.
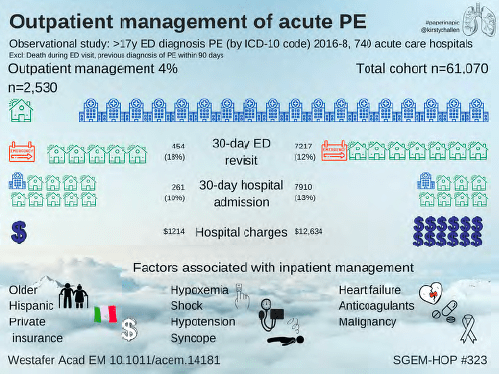
@RozhenalMD : In my experience the limiting factor is often the fact that some insurance plans cover rivaroxaban and others cover apixaban, apparently none cover both. So it’s practically impossible to figure this out and send them home on a doac unless it’s 2 pm on a Tuesday. Hence, obs.
Reply by author @LWestafer: We get around this with initial coupons. https://eliquis.com/eliquis/hcp/resources#panel- element-2… either 30d free or 10$ copay regardless of insurance- I tell patients they may get switched but this will get them started
Current dosing recommendations of topiramate for migraine prophylaxis approved by the FDA is to start at 25 mg a night for week 1, 25 mg twice a day for week 2, 25 mg in the morning and 50 mg in the evening on week 3, and finally 50 mg both morning and evening starting week 4.12 In patients with significant side effects, rapid discontinuation without tapering is favored.
As of November 2020, a one-month supply of topiramate (50 mg twice daily) costs $9.00 to $11.81.
Side effects: drowsy, dizzy, fatigue, also associated with long term and short cognitive dysfunction
Of the 256 children, 58 (22.7%) had clinically important intussusception. POCUS identified 60 (23.4%) children with clinically important intussusception. The diagnostic accuracy of POCUS was 97.7% (95% confidence interval [CI] 94.9% to 99.0%), compared to 99.3% (95% CI 96.8% to 99.9%) for RADUS.
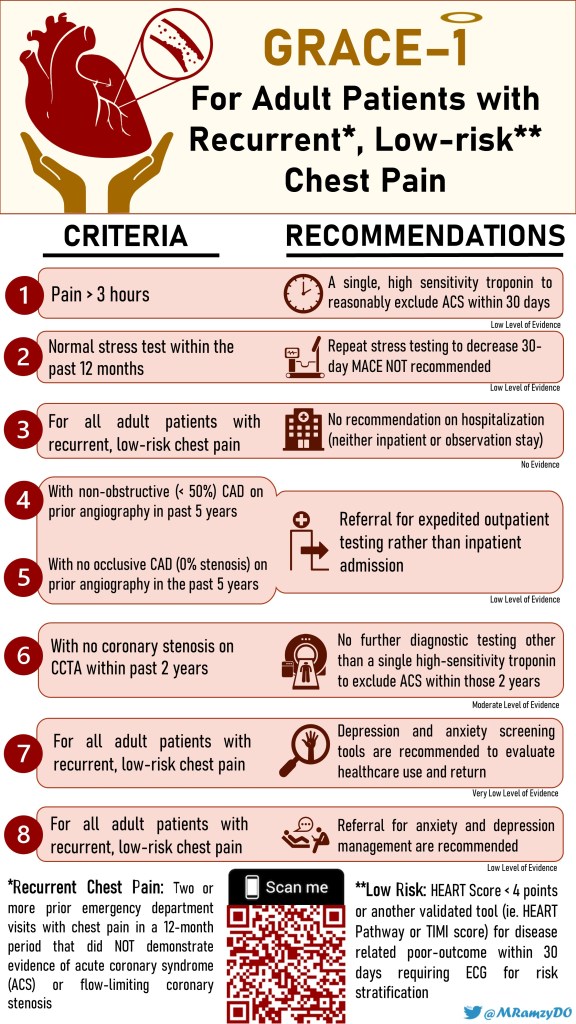
In patients with acute chest pain and suspected ACS who are deemed low-risk (<1% 30-day risk of death or MACE), it is reasonable to discharge home without admission or urgent cardiac testing.
Introducer Sheath is in (If the patient NEEDS a pacemaker–an experienced person should put in the introducer)
Position the Patient so you can see the monitor
Put the damn sterile sheath on the wire
Test the balloon (Special Syringe only allows 1.5 ml of air)
Attach to wire extender to the box, the pacemaker pins and tighten!!!! (Write Negative=Distal on your Pacemaker Drawer)
Have your partner set the box. Rate 2x intrinsic and V Output 20 mA
attribution neededOrient the curve
Advance to 15 cm
Call for balloon up (Note be GENTLE with balloon inflation/and only passive deflation. Down until 1.3 cc)
Advance somewhat rapidly until you see electrical capture (monitor shows big electrical spikes with lbbb morphology) then confirm mechanical capture by looking at rate of pulse ox or having someone check pulses or looking at ultrasound arterial pulse.
Do the turn down dance
Deflate Balloon/lock stopcock
Secure by first clamping down on the wire then attaching down distal and clamping proximal portions of sheath and suture the introducer to the patient
Hang box on IV pole
Check Sensitivity Settings
Get an Xray (RV placement will show the wire cross the midline)
In contrast to spontaneous bacterial peritonitis in patients with cirrhosis, which is diagnosed when the neutrophil count is 250 per μl or higher, peritoneal dialysis–related peritonitis is diagnosed with a white-cell count as low as 100 per μl if there are 50% or more neutrophils.
Retrospective study: Of the 2259 patients with RPAs and PPAs, 1677 (74.2%) were in the noncorticosteroid group and 582 (25.8%) were in the corticosteroid group. There were no significant differences in age, sex, or insurance status. There was a lower rate of drainage in the corticosteroid cohort (odds ratio: 0.28; confidence interval: 0.22–0.36). Patients in this group were more likely to have repeat computed tomography imaging performed, had lower hospital costs, and were less likely to have opioid medications administered. The corticosteroid cohort had a higher 7-day emergency department revisit rate, but there was no difference in length of stay (rate ratio 0.97; confidence interval: 0.92–1.02).
For patients with advanced inflammation, prophylactic intubation may be necessary. Involve consultants early for a possible awake intubation in the OR, and with preparations to convert to a surgical airway, if necessary.
Clinical Take Home Point: The combination of vasopressin and methylprednisolone compared to placebo during in-hospital cardiac arrest resulted in more ROSC but had no statistically significant difference in the more patient oriented outcomes of survival and survival with favorable neurologic status at 30 and 90d. In fact, survival at 30 days appeared to be worse in the VAM group. At this time, we cannot recommend the addition of vasopressin and methylprednisolone in the management of IHCA.
The American Academy of Orthopedic Surgeons recommends regional analgesia for preoperative pain control in patients with hip fracture (strong evidence).11 Based on the available evidence, the review summarized here found that PNB reduced pain on movement, shortened time to first mobilization, and resulted in lower rates of delirium and chest infections. Thus, we have assigned a color recommendation of green (benefit > harm) for PNB for hip fracture. Further study is needed to evaluate PNB in periods and settings other than the perioperative period and the potential benefit of continuous infusion versus single injection. However, current data support that this would be a valuable intervention for hip fractures that could be utilized in the ED.
In summary, the existing data indicate that NAIs reduce the duration of symptoms by less than 1 day in patients with confirmed or suspected influenza. The use of NAIs to treat influenza does not prevent hospitalization and is associated with adverse events. Therefore, we have assigned a color recommendation of yellow (unclear if it provides benefit, more data needed) to this treatment.
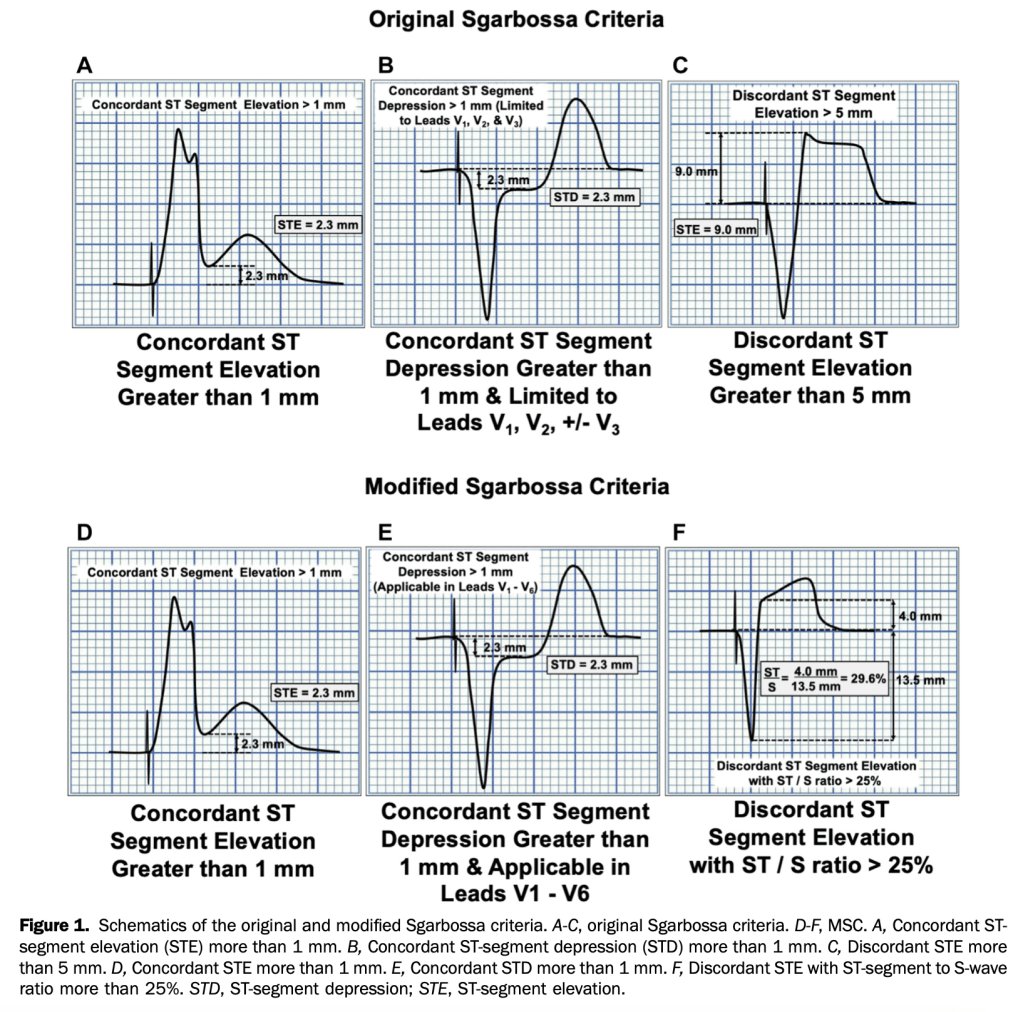
Modified Sgarbossa Criteria in LBBB- sensitivity was significantly higher than that of the original Sgarbossa criteria (91% versus 52% and 80% versus 49%, respectively; P<.001 for all) and high specificity was maintained (90% versus 98% and 99% versus 100%, respectively).
This study showed MSC were more sensitive than the original Sgarbossa criteria; specificity was high for both rules. The MSC may contribute to clinical decisionmaking for patients with ventricular paced rhythm. [Ann Emerg Med. 2021;78:517-529.]
Etoricoxib 60 mg/day and diclofenac 150 mg/day seem to be the most effective oral NSAIDs for pain and function in patients with osteoarthritis. However, these treatments are probably not appropriate for patients with comorbidities or for long term use because of the slight increase in the risk of adverse events. Additionally, an increased risk of dropping out due to adverse events was found for diclofenac 150 mg/day. Topical diclofenac 70-81 mg/day seems to be effective and generally safer because of reduced systemic exposure and lower dose, and should be considered as first line pharmacological treatmentfor knee osteoarthritis. The clinical benefit of opioid treatment, regardless of preparation or dose, does not outweigh the harm it might cause in patients with osteoarthritis.
CONCLUSIONS: Acute urinary retention might be a clinical marker for occult urogenital, colorectal, and neurological cancers. Occult cancer should possibly be considered in patients aged 50 years or older presenting with acute urinary retention and no obvious underlying cause.
The absolute risk of prostate cancer after a first diagnosis of acute urinary retention was 5.1% (n=3198) at three months, 6.7% (n=4233) at one year, and 8.5% (n=5217) at five years. Within three months of follow-up, 218 excess cases of prostate cancer per 1000 person years were detected. An additional 21 excess cases per 1000 person years were detected during three to less than 12 months of follow-up, but beyond 12 months the excess risk was negligible.
Avoid first antihistamines, second generation ok (loratadine)
Nitrofurantoin (on the list bc not effective if cr cl<30, otherwise ok for short term)
NSAIDS: incr cv and go complications, naproxen safest, safer than ibuprofen
Antipsychotics: increased risk from prolonged use
Neutropenic Fever
Fever: Temperature greater than 101ºF (38.3ºC) or sustained of 100.4ºF (38ºC) for at least an hour.
Neutropenia: Absolute neutrophil count (ANC) < 1000 with an expected decrease to 500, or an ANC of < 500.
The most common (and deadly) bacterial sources of infection are gram negative bac-teria. There is also a higher rate of resistant organisms and opportunistic infections.
If there is no obvious source of infection, the work-up should include 2 blood cultures (1 from indwelling line, if present), liver function tests, bilirubin, chest x-ray (if upper or lower respiratory infectious symptoms), and respiratory viral panel.
Administer empiric antibiotics as quickly as possible:
Provide gram negative coverage with antipseudomonal activity: cefepime or a carbapenem if concern for ESBL.
Piperacillin-tazobactam is another common choice.
Vancomycin can be considered if an indwelling line is suspected to be the source of infection, or if they are hypotensive or toxic-appearing.
Some patients may need fungal or viral coverage.
Which patients can go home?
Use MASCC calculator on MDCALC.
This should only be done in consultation with oncology.
Watchman Procedure
A cardiology procedure that eliminates the left atrial appendage, thus reducing the risk of clot formation in patients with atrial fibrillation (paroxysmal or chronic).
Performed via percutaneous access through the femoral artery.
Over approximately 45 days, the myocardium grows over the device that is placed in the appendage.
Patients require anticoagulation for the first 45 days due to increased risk of thrombo-embolic disease, but do not require chronic anticoagulation.
Watchman device versus systemic anticoagulation:
Lower hemorrhagic stroke rate with the device. Lower cardiovascular mortality with the device. No difference in ischemic stroke rate.
Overall complication rate: approximately 1-8% (most occurring immediately post-procedure). Cardiac perforation leading to tamponade.
For pain freedom or pain relief at 2 hours after the dose, lasmiditan, rimegepant, and ubrogepant were associated with higher ORs compared with placebo but lower ORs compared with most triptans. However, the lack of cardiovascular risks for these new classes of migraine-specific treatments may offer an alternative to triptans.
Association of Tramadol vs Codeine Prescription Dispensation With Mortality and Other Adverse Clinical Outcomes (no open access)
Compared with codeine, tramadol dispensation was significantly associated with a higher risk of all-cause mortality (incidence, 13.00 vs 5.61 per 1000 person-years; HR, 2.31 [95% CI, 2.08-2.56]; ARD, 7.37 [95% CI, 6.09-8.78] per 1000 person-years), cardiovascular events (incidence, 10.03 vs 8.67 per 1000 person-years; HR, 1.15 [95% CI, 1.05-1.27]; ARD, 1.36 [95% CI, 0.45-2.36] per 1000 person-years), and fractures (incidence, 12.26 vs 8.13 per 1000 person-years; HR, 1.50 [95% CI, 1.37-1.65]; ARD, 4.10 [95% CI, 3.02-5.29] per 1000 person-years). No significant difference was observed for the risk of falls, delirium, constipation, opioid abuse/dependence, or sleep disorders.
J Am Geriatr Soc.
Effect of age on treatment outcomes in benign paroxysmal positional vertigo: A systematic review (no open access)
Although more CRPs (Canalith Repositioning Procedures- Epley’s maneuvers) are needed, the rate of complete recovery in older adults is similar to that observed in younger adults.
Once you figure out the neonate that presented to your ED is sick, run through a differential of why then can be sick so you don’t anchor. I like to use TIMOT (Trauma, Infection, Metabolic, Organs, Tox) but use whatever works for you.
Use your detailed history looking for risk factors to help you narrow the differential down. Do a good hands-on physical exam. Work them up more than you would a standard baby and do things like you would to an adult such as a bedside US. These will all lead you to the diagnosis of a congenital cardiac disease
You have two options now: they either have a cyanotic lesion that requires prostaglandins and a dose of 0.05-0.2 mg/kg/min and will need to be intubated. Or they are in full blown heart failure and require lasix at 1 mg/kg and pressors, typically a combination of dobutamine and norepinephrine.
Don’t be a hero but don’t have imposter syndrome. You can manage these kids, but do so with support from your PICU, cardiac surgeon or transferring institution. What you are doing in the ED is temporizing to keep them alive to definitive therapy which is usually a combination of ECMO and/or surgery. Get them out of your department ASAP.
Clinical Take Home Point: In hemodynamic and electrically stable patients with OHCA and no STEMI after ROSC, an immediate-angiography strategy does not appear to improve 30-day mortality. It appears that an approach of intensive care first followed by delayed angiography if clinically indicated is preferred.
Clinical Take Home Point: Although earlier trials showed a signal of benefit for remdesivir improving time to recovery, no trials have shown an improvement in mortality, a more important clinical outcome. Additionally, this is now the third trial showing no clinical benefit of remdesivir. The current evidence does not support the use of remdesivir in hospitalized patients with symptoms for more than 7 days and requiring oxygen support. This story sounds much like another antiviral medication used for another viral illness (i.e. Tamiflu for influenza), except this medication is much more expensive ($3k – 5k for a 5 day course).
Of the 514/1081 (47.5%) infants who met the PECARN low-risk criteria, 1/514 (0.2%, 95% confidence interval [CI] 0.005% to 1.1%), had clinically important traumatic brain injuries1/514 (0.2%, 95% confidence interval [CI] 0.005% to 1.1%)
CONCLUSIONS: Moderate to high certainty evidence shows that non-inhaled medical cannabis or cannabinoids results in a small to very small improvement in pain relief, physical functioning, and sleep quality among patients with chronic pain, along with several transient adverse side effects, compared with placebo. The accompanying BMJ Rapid Recommendation provides contextualised guidance based on this body of evidence.
Use a body bag (the same ones used to transport patients to the morgue) to cool patient rapidly in 20-30 minutes. Put patient in the bag and fill with ice and water.
Pulse ox waveform depends on perfusion index (ratio of pulsatile blood over non-pulsatile blood), <0.5 has a poor waveform.
Low cardiac output (cardiogenic shock) or vasoconstriction (hemorrhagic shock) cause lower perfusion index and poor waveform, while septic shock tends to be warm and hypotensive due to poor vasoconstriction.
For patients with COVID-19 pneumonia and acute hypoxemic respiratory failure, CPAP reduced the need for intubation compared to conventional oxygen therapy. However, HFNO did not reduce the need for intubation compared to conventional oxygen therapy. Neither intervention showed a statistically significant mortality benefit compared to conventional oxygen therapy, however, the study was not powered for this outcome. Although the conclusion of the trial is CPAP > HFNO > COT, there may be some scenarios where HFNO > CPAP to reduce adverse events (i.e awake prone positioning, patient nutrition, etc).
This is the highest-level evidence we have to date on awake prone positioning. In this trial of patients with hypoxemic respiratory failure due to COVID-19, awake prone positioning reduced the incidence of treatment failure (intubation and death), which was primarily driven by decreased intubation compared to standard care. Not only was there no signal of harm from awake prone positioning, but even longer durations of awake prone positioning (>8hrs/day) were associated with a lower risk of treatment failure.
Abx reduce complications in culture positive asymptomatic bacteriuria, which is a subset of asymptomatic bacteriuria before culture performed.
Uptodate makes no mention of checking UA in pregnant patients with abnormal vaginal bleeding. I was taught in residency to do this to rule out occult UTI as a cause of threatened miscarriage, then the UA always comes back with a few wbcs or bacteria and I feel obliged to treat. I’m gonna stop!
ED clinicians had only moderate agreement with research HEART scores. Combined with uncertainties regarding accuracy in predicting major adverse cardiac events, we urge caution in the widespread use of the HEART score as the sole determinant of ED disposition.
Showed a benefit to therapeutic anticoagulation in non-critically ill but this benefit was small per Uptodate and other studies have not shown a benefit and the incidence of thromboembolic events in hospitalized patients are lower now than earlier in the pandemic, possibly related to the use of steroids and tocilizumab.
In CRITICALLY ILL patients with COVID-19, an initial strategy of therapeutic-dose anticoagulation is not associated with a greater probability of survival to hospital discharge or a greater number of days free of cardiovascular or respiratory organ support vs usual-care pharmacologic thromboprophylaxis
In NON-CRITICALLY ILL patients with COVID-19, an initial strategy of therapeutic-dose anticoagulation is associated with a greater probability of survival to hospital discharge or a greater number of days free of cardiovascular or respiratory organ support vs usual-care pharmacologic thromboprophylaxis
In NON-CRITICALLY ILL patients with COVID-19, there is a clear signal of benefit, however with all the protocol violations and variable treatment arms it would still be reasonable to discuss with the inpatient team to help guide the decision (Although, in my practice and at my institution most patients who are not critically ill and don’t have contraindications, we have changed our protocols to full dose anticoagulation).
In this retrospective study of patients receiving blood cultures at a hospital in The Netherlands, we found that 6.3% of patients with SARS- CoV-2 had positive blood cultures and all were considered contaminated. Overall bacterial coinfection using other diagnostics was 1.4%. This suggests that in patients known to have SARS- CoV-2, blood cultures are unlikely to be of use.
Procalcitonin and the Pneumonia Severity Index seem most promising to recognise patients at risk for severe outcome of COVID-19 when presenting to the ED.
A traumatic arthrotomy is a laceration that extends into the joint capsule exposing the intra-articular surface to the environment. It is important to identify, as operative washout, debridement and proper closure of the joint capsule is required.
Instill saline into the joint and see if it leaks out through the laceration. Leakage of saline means you have an arthrotomy.
For the knee, a load of 194 mL achieves 95% sensitivity.
Keese GR, Boody AR, Wongworawat MD, Jobe CM. The Accuracy of the Saline Load Test in the Diagnosis of Traumatic Knee Arthrotomies. Journal of Orthopaedic Trauma. 2007;21(7):442-443. doi: 10.1097/BOT.0b013e31812e5186.
Sensitivity of anterior nares is lower (82-88%) than nasopharyngeal (98%) but in a population with 10% positivity, the negative predictive value is still greater than 98%.
Evolving definition of the previously termed conversion disorder, now called functional neurological disorder (FND) in which there is loss of motor or sensory or presence of seizure activity without any evidence of structural pathology.
Can be thought of as a software problem rather than a hardware problem
Two useful tests are hip abductor sign (hip abduction felt on one side while and hoover’s sign
FI GURE 2 Hip abductor and Hoover’s sign of functional leg weakness. Top left: Hip abductor sign – weak left hip abduction. Top right: Hip abductor sign – strength in left hip returns to normal with abduction of right hip. Bottom left: Hoover’s sign – weak left hip extension. Bottom right: Hoover’s sign – strength in left hip extension returns to normal with right hip flexion.
Management errors were varied and remarkable for the frequency of patients with elevated troponin levels which were not repeated, and there was no indication that the elevated value was appreciated in the health record.
For patients with atrial fibrillation, unappreciated dual diagnoses (eg, acute heart failure, community-acquired pneumonia, exacerbation of chronic obstructive pulmonary disease), clinical severity, and missing the underlying cause contributed to diagnostic errors (eg, pulmonary embolism, community-acquired pneumonia).
3 cases of patients experiencing adverse drug effects related to warfarin and 3 related to direct oral anticoagulants.
Two patients with recent-onset atrial fibrillation and elevated Congestive Heart Failure, Hypertension, Age, Diabetes, previous Stroke scores were discharged without anticoagulation and returned with severe strokes.
Although patients discharged with syncope had fewer adverse events, the majority of events (10) were diagnostic errors, and 2 key contributing factor themes were failure to seek an underlying cause (eg, end-stage heart failure, community-acquired pneumonia, gastrointestinal bleeding) and lack of recognition of injuries related to the fall from syncope (eg, missed fractures)
Although intravascular temperature management does not improve survival compared with surface-cooling methods in post–cardiac arrest patients, it may improve neurologic outcomes.
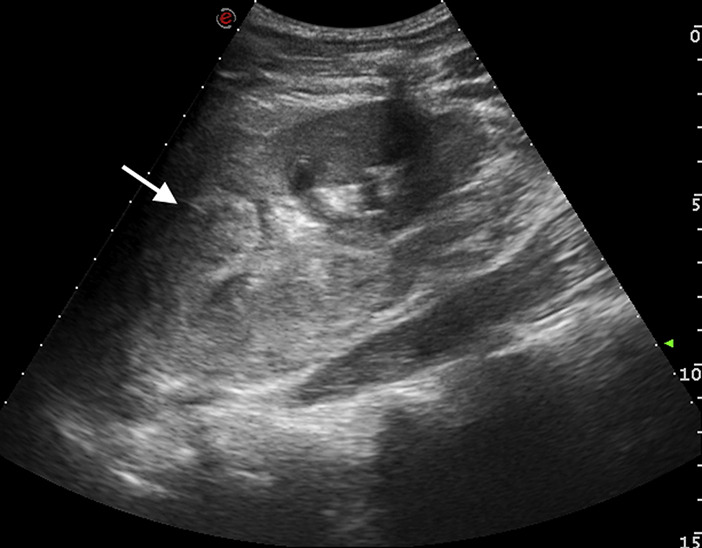
A 15-year-old previously healthy boy was admitted for a blunt abdominal trauma owing to a cycling crash. On admission he was alert; blood pressure and pulse rate were 145/95 mm Hg and 75 beats/min, respectively. Physical examination result was remarkable for severe left-sided flank pain with guarding. No others injuries were found. His urine was like blood and laboratory tests showed a normal hemoglobin level, at 13.5 g/dL, with hematocrit level 40.9%.
An abdominal ultrasonographic scan showed major left kidney trauma (Figure 1). A computed tomographic (CT) scan confirmed a grade IV renal laceration, according to the American Association for the Surgery of Trauma classification (Figure 2).
In patients with coma after out-of-hospital cardiac arrest, targeted hypothermia did not lead to a lower incidence of death by 6 months than targeted normothermia.


{kind=link}