Conclusion: “Many risk stratification scores are not validated or not sufficiently accurate for clinical use. The CSRS is an accurate validated prediction score for ED patients with unexplained syncope. Its impact on clinical decision making, admission rates, cost, or outcomes of care is not known.”
Of the 542 included patients, 46 (10%) required transfer to ICU within 24 hours of admission. The final composite model, adjusted for age and admission location, included history of heart failure and initial oxygen saturation of <93% plus either white blood cell count > 6.4 or glomerular filtration rate < 46. The odds ratio (OR) for decompensation within 24 hours was 5.17 (95% confidence interval [CI] = 2.17 to 12.31) when all criteria were present. For patients without the above criteria, the OR for ICU transfer was 0.20 (95% CI = 0.09 to 0.45).
Harm reduction for ED patients with injection drug use includes free dispensation of Naloxone (learn more about how EDs can get free naloxone to dispense here), and syringe services programs (find the SSP closest to you here).
2.6% of patients intubated patients recall an awareness of paralysis, with a two-fold risk among patients paralyzed with rocuronium (have your sedative ready to hang immediately after intubation).
Here’s the most important takeaway of the “HHS Practice Guidelines for the Administration of Buprenorphine for Treating Opioid Use Disorder”: All prescribers with a valid state license and DEA can register for an X wavier without mandatory training. It’s now a simple process. Get your X waiver TODAY!
PO Potassium Bicarbonate more palatable than KCl, dose is 50meq PO
Oral Magnesium Oxide 400-800mg tablet
Mag IV 4-8g if Mag<1, 2-4g if mag 1-1.4, 1-2g if Mag 1.5-1.9.
Calcium: 2g CaGluconate over 1 hour if sick.
Phosphate: typically replete if Phos<1, give Potassium Phos if K is low, give Sodium Phos if serum potassium is high, can give 15, 30 or 45 mmol depending on how low phosphate level is, typically 15 mmol/hr
Ask permission to share bad news: “I am afraid I have serious news. Would it be ok if I share?”
Align: “We need to work together quickly to make the best decisions for her care”.
Baseline function: “To decide which treatments might help her the most, I need to know more about her, what type of activities was she doing before her illness.”
“How much more would she be willing to go through for the possibility of more time?”
Preferred venous access is a 5f umbilical vein line, inserted in the little mouth of the umbilical stump face (umbilical arteries are the eyes, vein is the mouth). insert the 5f line 4-5cm until blood returns.
IO also an option but has a higher failure rate than in older kids.
Consider termination of CPR after 20 minutes with no detectable heart rate.
A total of 2,309 patients met criteria for inclusion in the study. Physician uptake of the HINTS exam was high, with 450 (19.5%) dizzy patients receiving all or part of the HINTS. A large majority of patients (96.9%) did not meet criteria for receiving the test as described in validation studies; most often this was because patients lacked documentation of nystagmus or described their symptoms as intermittent. In addition, many patients received both HINTS and Dix-Hallpike exams, which are intended for use in mutually exclusive patient populations. In no case was dizziness due to a central cause identified using the HINTS exam.
Sensitivity only 55% for gonorrhea with urine or endocervical swab so authors recommend empiric treatment rather than waiting for results. There is a counter-argument in the same issue but this one makes more sense to me. Probably should incorporate population characteristics and patient shared-decision making.
A 30-year-old man presented to the emergency department with throat pain and oral intolerance of fluids for several hours. Earlier that day, an outpatient operation was aborted after multiple unsuccessful intubation attempts in the operating room. The patient had unremarkable vital signs, noting only odynophagia. Computed tomography (CT) of the neck and an esophagram with water-soluble contrast were acquired.
This small trial found a trend toward benefit for the non-lytic group when comparing between patients treated with EVT alone versus EVT plus IVT for acute CVA.
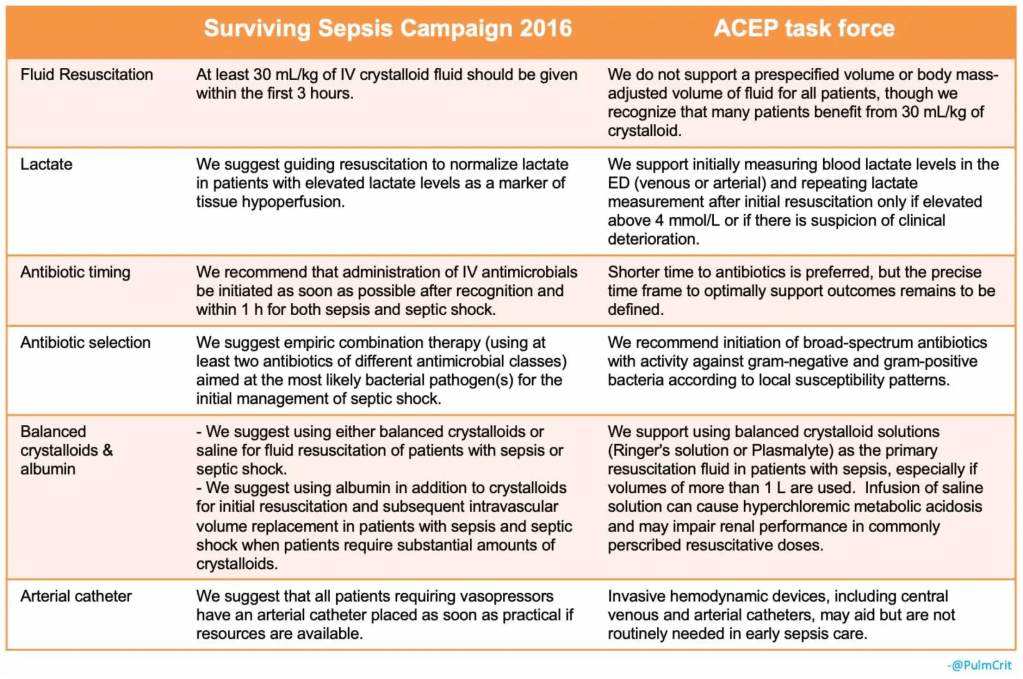
The ACEP consensus-based task force report was just published (see lead article in Annals of EM section above). Although spearheaded by ACEP, the report is also endorsed by the Society of Hospital Medicine (SHM) and the Society of Critical Care Medicine (SCCM).
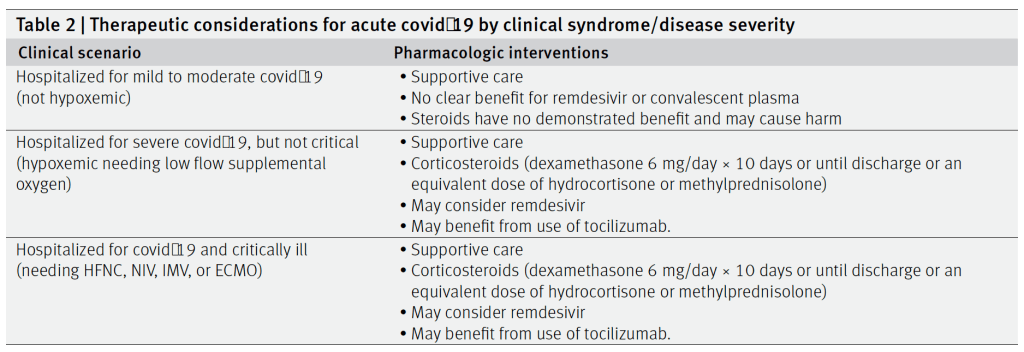
In critically ill patients with Covid-19 receiving organ support in ICUs, treatment with the interleukin-6 receptor antagonists tocilizumab and sarilumab improved outcomes, including survival, at 90 days.
All patients with an adrenal mass that is discovered during diagnostic testing for another condition (an “incidentaloma”) should undergo biochemical testing to detect pheochromocytoma and excess cortisol secretion, and those who also have high blood pressure should undergo biochemical testing to detect primary hyperaldosteronism.
Patients with pheochromocytoma should undergo adrenalectomy after adequate presurgical alpha- blockade and beta-blockade, if necessary.
Patients with mild autonomous cortisol excess and primary hyperaldosteronism may benefit from adrenalectomy, but treatment should be individualized.
Nonfunctioning adrenal tumors that have an attenuation of 10 Hounsfield units or less on computed tomographic (CT) evaluation and that are smaller than 4 cm in greatest diameter generally do not warrant intervention or long-term follow-up.
All other adrenal incidentalomas with indeterminate features on imaging may warrant additional imaging with contrast-enhanced CT, magnetic resonance imaging with chemical-shift analysis, positron-emission tomography–CT with 18F-fluorodeoxyglucose, or all of these tests. The management of these masses should be individualized and should involve a multidisciplinary team consisting of an endocrinologist, an endocrine surgeon, and a radiologist.
Authors recommend replacing red man syndrome with infusion reaction for all non-immune mediated reactions.
Uptodate uses the term vancomycin flushing syndrome or vancomycin infusion reaction.
The two can be distinguished if it is the first time a patient has been exposed to vancomycin it will not be an IgE reaction.
Otherwise they can be difficult to distinguish and may require allergy consult/testing to distinguish.
Typically the infusion reaction is characterized by upper body, neck an face greater than lower body flushing, erythema and itching. Pain and muscle spasms in the back and chest as well as dyspnea and hypotension may occur.
In this methodologically novel trial (Goulden R et al. Association of Intravenous Radiocontrast With Kidney Function: A Regression Discontinuity Analysis. JAMA Intern Med 2021. [Link is HERE]) there was no association between IV contrast from CTPA and worsening eGFR up to 6 months after index ED visit. Although a randomized clinical trial would be great, this may be the highest-level evidence we achieve. This trial plus other observational trials on this topic all point to a change in protocols to allow for IV contrast in patients regardless of kidney function.
In summary, the evidence for using a patient’s GCS score is mixed. Recent review articles have highlighted the paucity of strong evidence behind the classic adage of “GCS less than 8, intubate”. Orso D et al. Endotracheal intubation to reduce aspiration events in acutely comatose patients: a systematic review. Scand J Trauma Resusc Emerg Med. 2020.
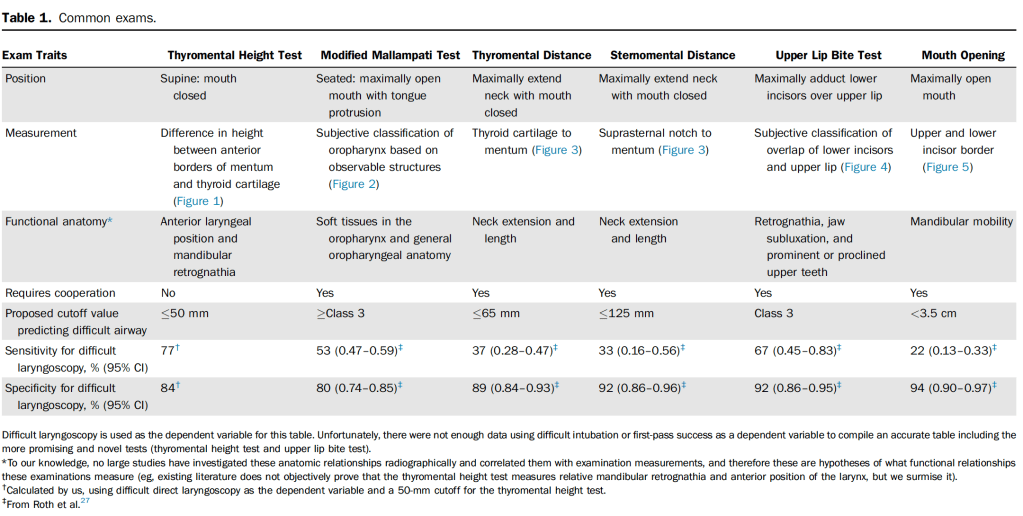
Several tools to assess airway difficulty but they require patient cooperation.
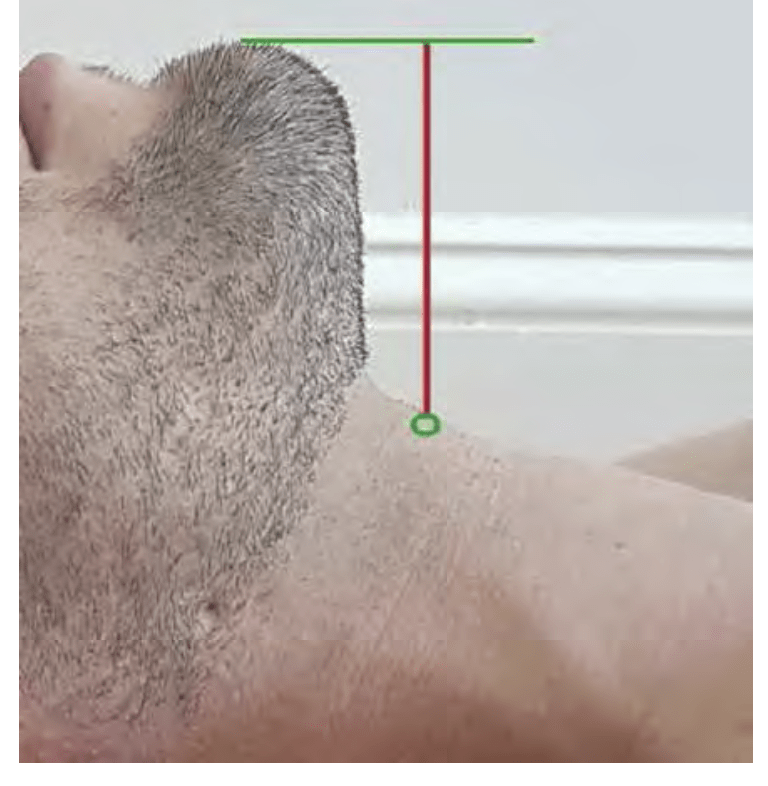
Thyromental height does not require patient cooperation and has both best sensitivity and moderate specificity.
Authors: “Early evidence on the thyromental height test is promising, given its higher sensitivity, reasonable specificity, and wider potential for application in the ED. However, to date no ED-, EMS-, or video laryngoscopy–based studies have been completed, to our knowledge.
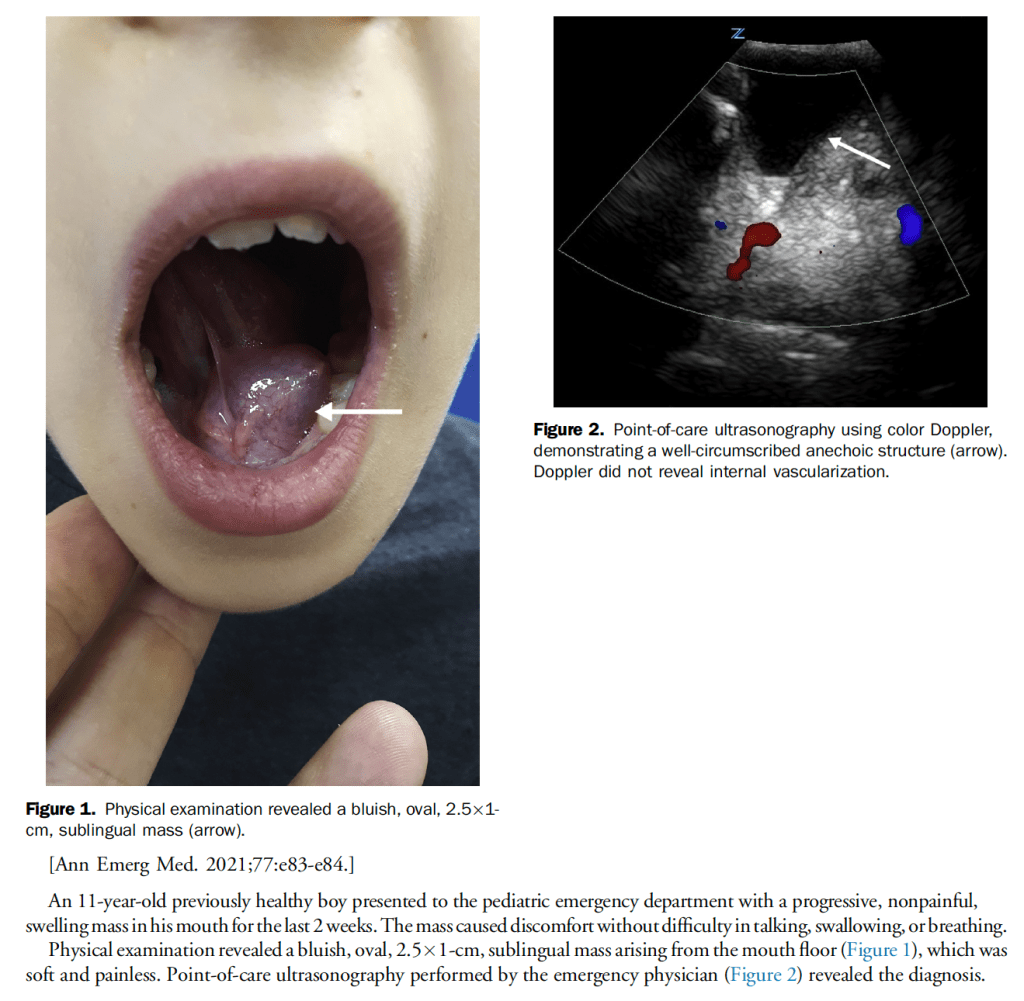
Sublingual ranula is a relatively common finding in the pediatric population, especially during the first and second decade of life, pseudocystic lesion, outpatient referral to ENT.
First and largest prospective multisite US cohort study to evaluate hs-cTnT strategies to date
NPV reached >99% with the combo 0 and 1 hour HS troponin plus a low heart score but using that approach only allowed 30.8% of patients to be discharged.
There was a high rate of MACE at 30 days (14.4%)
The study raises questions about whether HS-trop will improve efficiency if the discharge rate is 30.8%
Strawberry tongue seen in Strep but also in Kawasaki’s, this patient had 2 Kawasaki findings (tongue and lymphadenopathy) but needs fever for 5d and four additional findings (she had no rash, conjunctival injection or peripheral edema/erythema/desquamation).
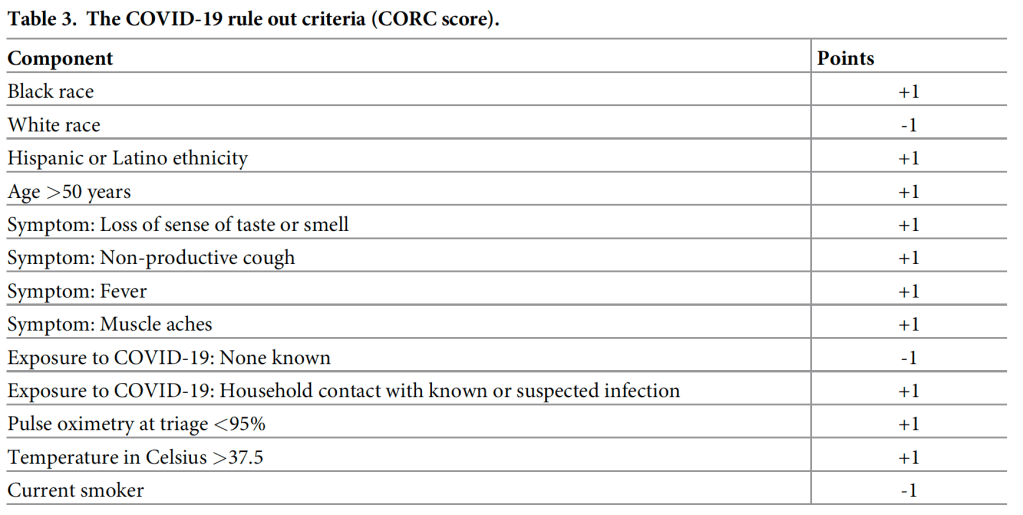
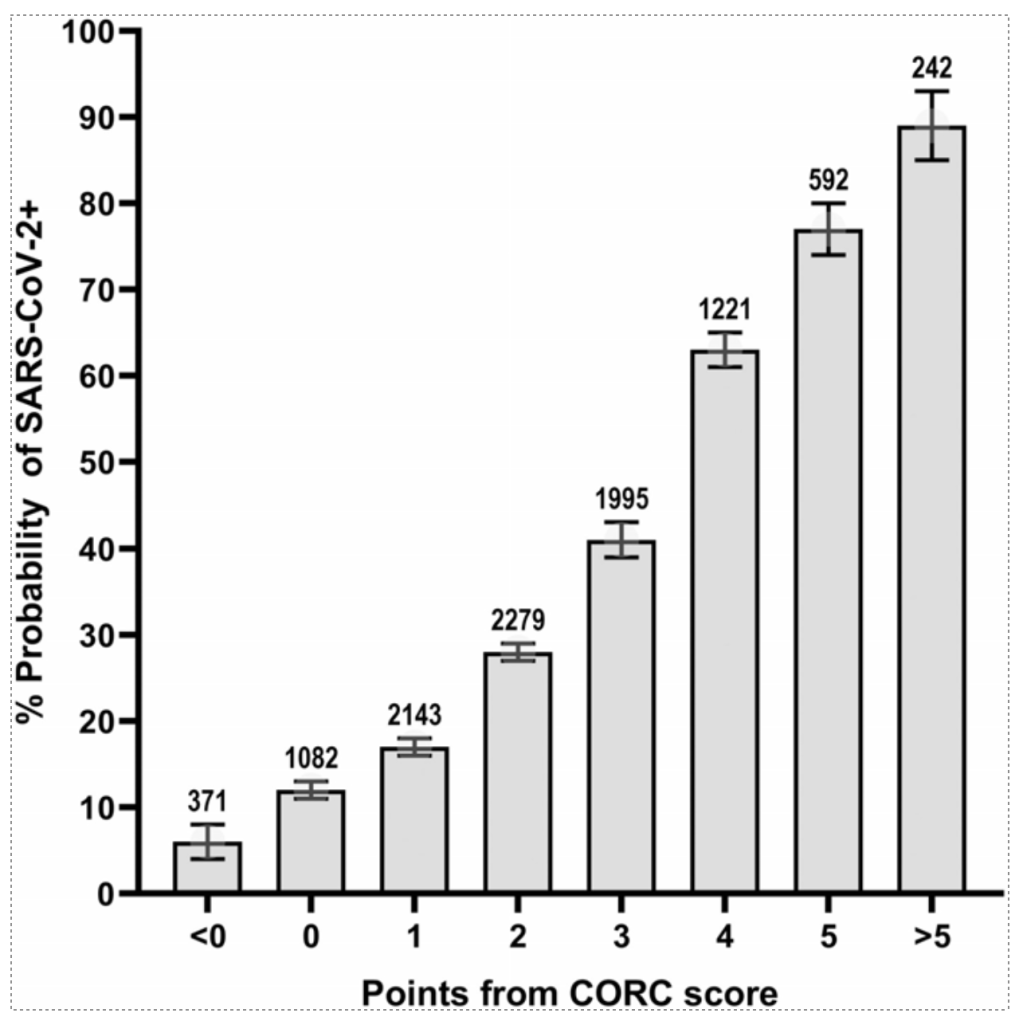
In the simplified score, a score of zero produced a sensitivity of 95.6% (94.8–96.3%), specificity of 20.0% (19.0–21.0%), negative likelihood ratio of 0.22 (0.19–0.26). Increasing points on the simplified score predicted higher probability of infection (e.g., >75%probability with +5 or more points).
We now have three randomized controlled trials (DIRECT-MT, DEVT, SKIP) as well as retrospective, non-randomized data (Phan 2017, Rai 2018) looking at this question.
In all three RCTs, the endovascular arm performed numerically better than the combination arm. This would appear to support a move towards endovascular therapy alone.
Addition of the HEART score to an initial hs-TnT below the limit of quantification improves sensitivity and NPV for cardiac events increasing patient safety, but this strategy does rule-out fewer patients (30.8%).
Clinical Take Home Point: Discharging patients presenting to the ED with chest pain after a single negative conventional troponin and proper risk stratification with the HEART score can be considered to be as safe as serial troponin testing while being less time consuming, less costly and therefore more patient oriented.
Paper: Wassie et al. Single versus serial measurements of cardiac troponin in the evaluation of emergency department patients with suspected acute myocardial infarction. JAMA Network Open 2021.
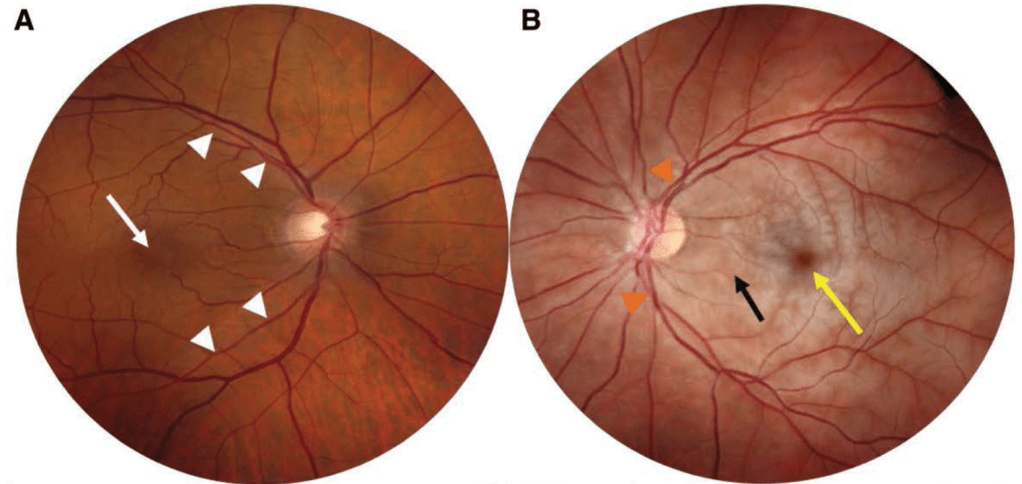
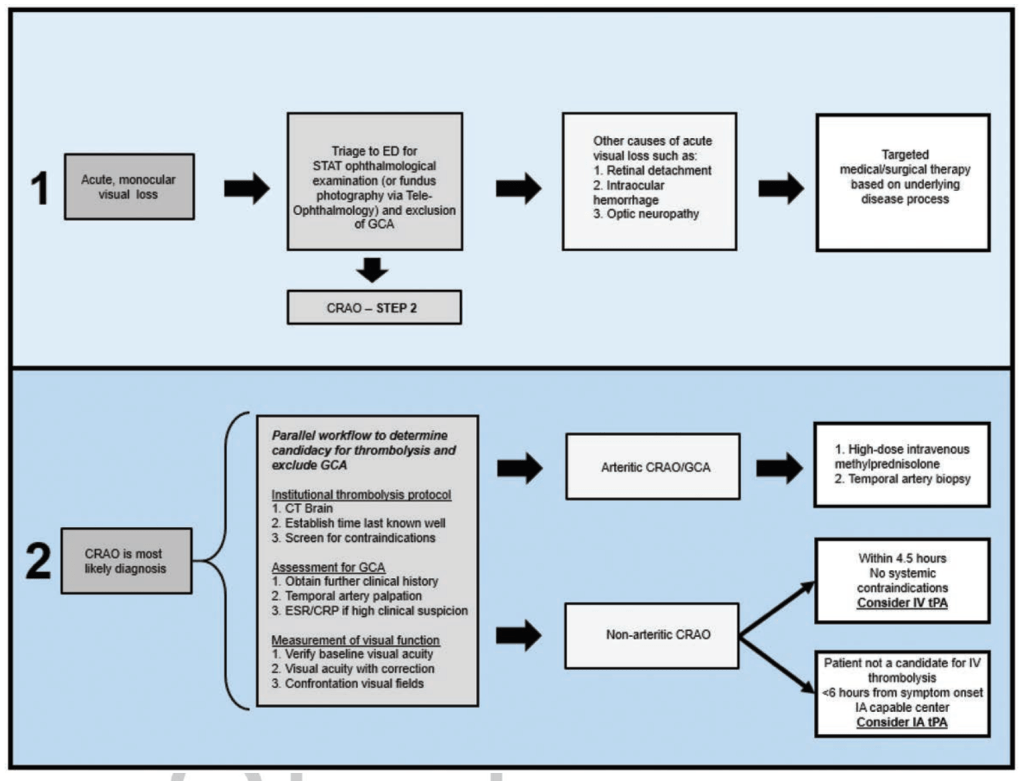
A, Fundus photograph of the normal right eye. Note the normal fovea (white arrow) and the normal retinal arteries (white arrowheads). B, Fundus photograph of a left CRAO showing diffuse retinal whitening (black arrow) with a cherry red spot (yellow arrow), attenuated arteries (orange arrowheads). Note the difference in color of the edematous retina compared with the normal right eye.
The success rates of the first attempt and the procedure time were statistically significant between the IO group and the CVC group (91.7% vs. 50.0%, P<0.001; 52.0 seconds vs. 900.0 seconds, P<0.001).
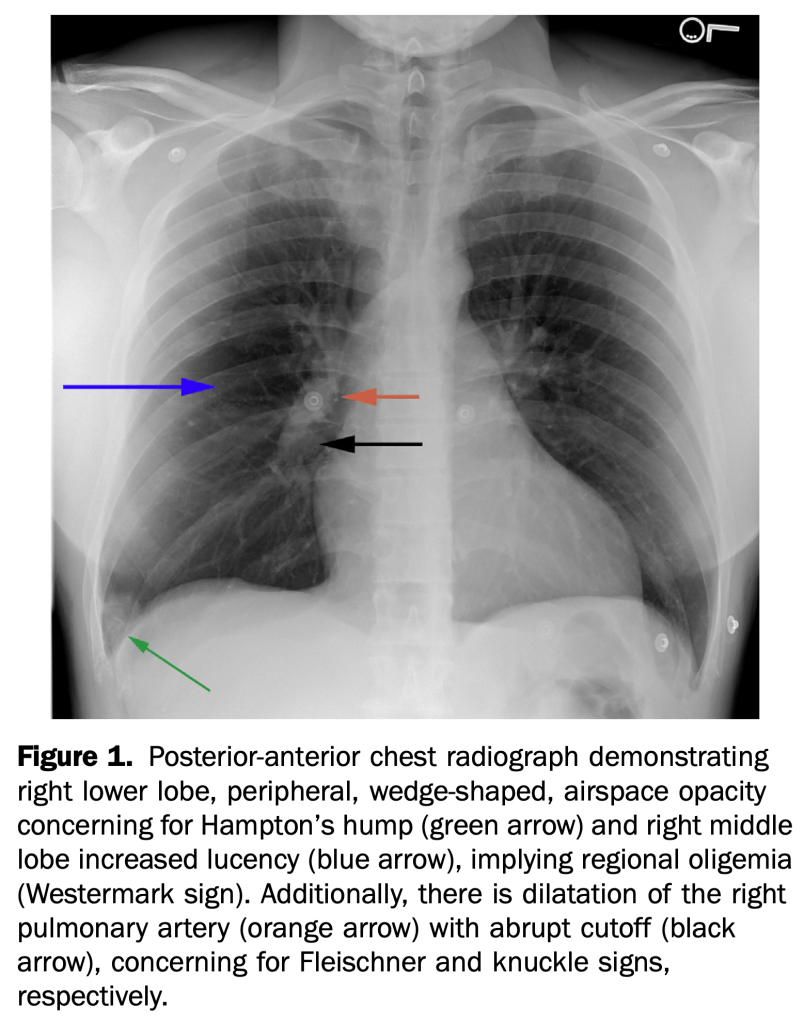
An otherwise healthy 35-year-old active duty military infantryman presented to the emergency department, complaining of intermittent dyspnea over one-week duration, which was worsened by exertion. He recalled some unusual left leg cramping three weeks before and reported an uncomplicated tooth extraction one week before, but denied any invasive surgeries.
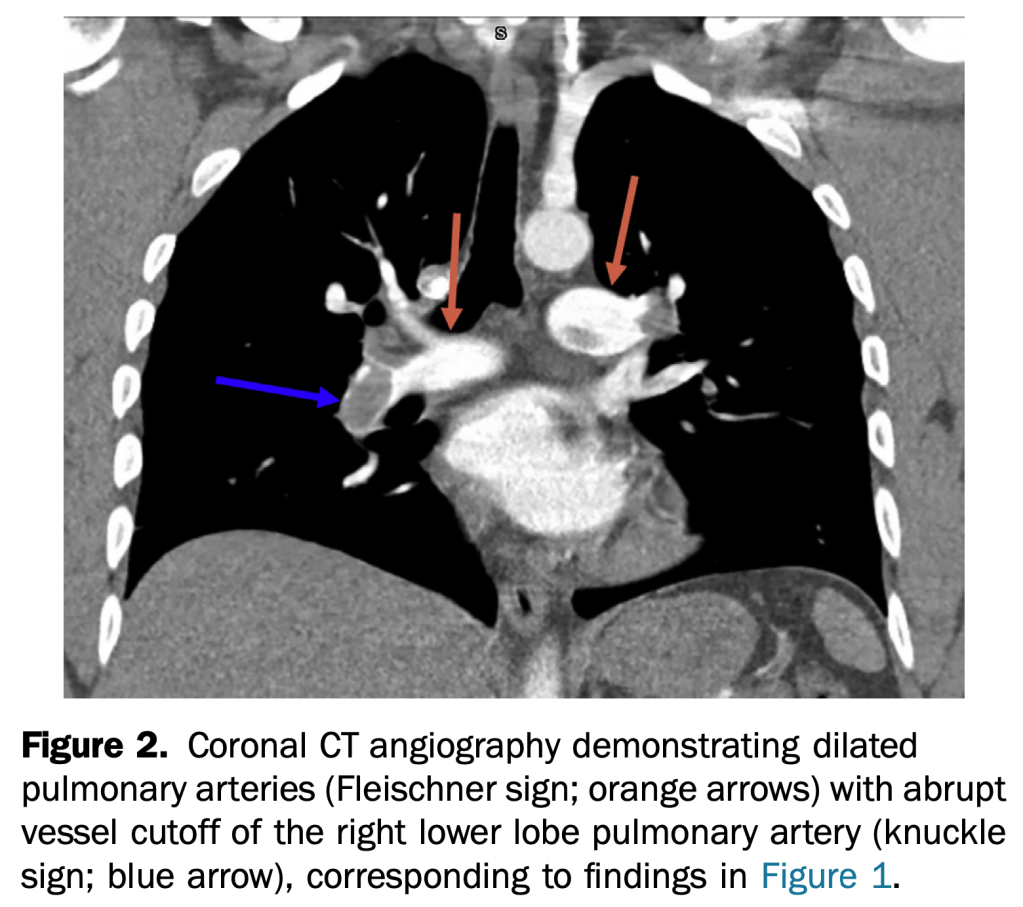
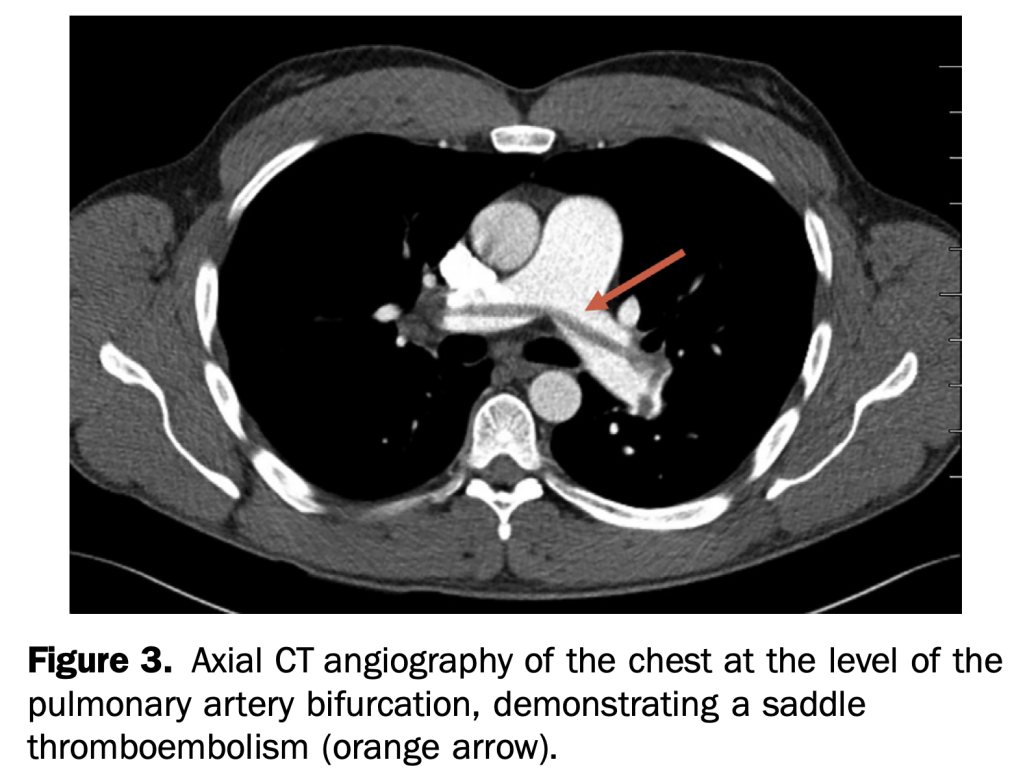
This case demonstrates multiple rare but specific radiographic findings of pulmonary embolism. These include the Westermark, knuckle, and Fleischner signs, in addition to Hampton’s hump.
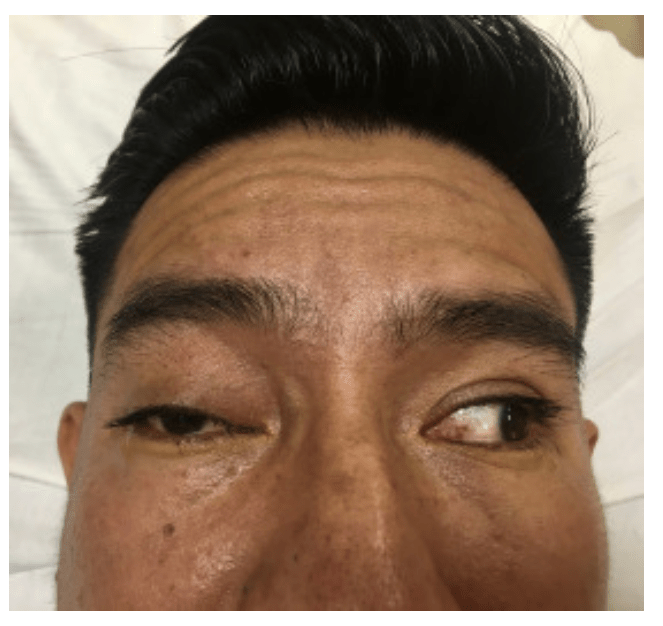
A 36-year-old man presented to the emergency department with double vision. Four weeks before, he had been struck in the face and he underwent open reduction and internal fixation of a mandibular fracture. He had intact cranial nerves in the immediate postoperative period. On examination, he displayed preserved visual acuity, a right-sided cranial nerve III palsy with an inferiorly abducted right eye, loss of medial and upward gaze, significant right-sided ptosis, and asymmetric mydriasis (Figure 1 and Video E1 [available online at http://www.annemergmed.com]). A bruit was auscultated over the affected eye.
Computed tomographic angiography of the brain revealed arterial filling of the cavernous sinus, consistent with a right-sided carotid-cavernous fistula and a dilated right ophthalmic vein.
Between January 1, 2010, and May 31, 2017, 205 pregnant patients presented to the ED with a neurologic chief complaint. The majority of patients had a normal neurologic examination result. Patients with an abnormal examination result were not more likely to have clinically significant imaging findings.
Within our population, 28% underwent imaging, and noncontrast magnetic resonance imaging was the most common modality. Five patients had clinically significant imaging findings. Specifically, 3.3% of patients with abnormal examination result had significant findings and 2.3% of those with a normal examination result had significant findings.
A normal examination result does not adequately exclude serious intracranial pathology, and diagnostic vigilance is justified.
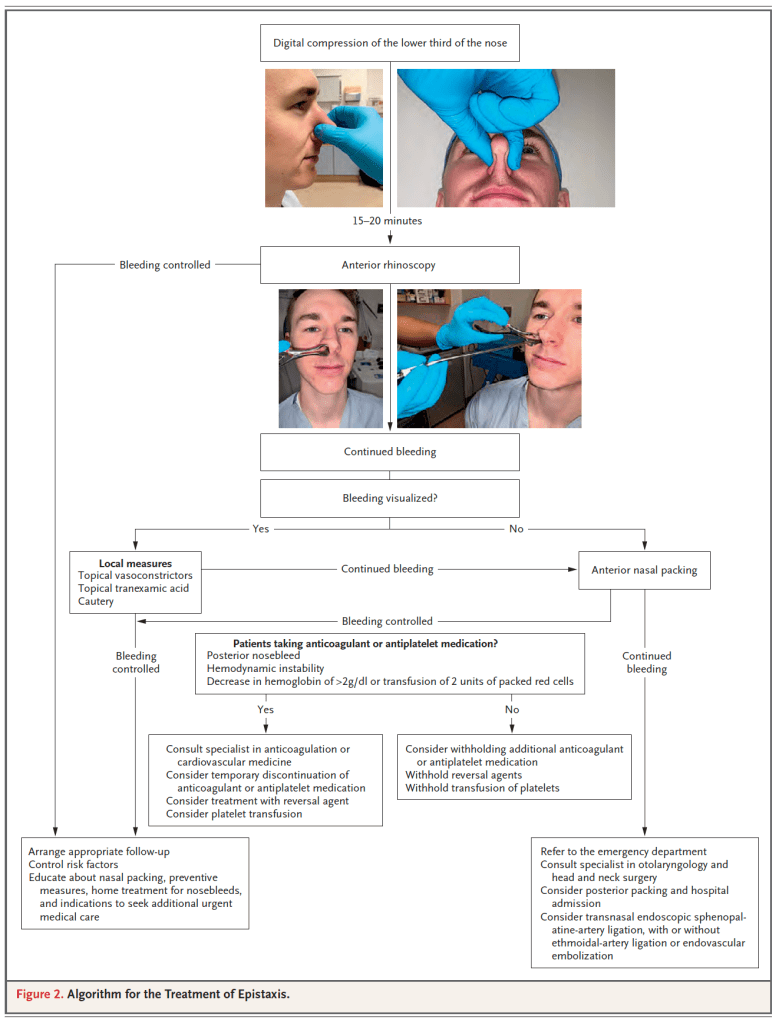
In patients presenting to an ED with atraumatic epistaxis that is uncontrolled with simple first aid measures, topical tranexamic acid applied in the bleeding nostril on a cotton wool dental roll is no more effective than placebo at controlling bleeding and reducing the need for anterior nasal packing.
The Canadian TIA Score stratifies patients seven day risk for stroke, with or without carotid endarterectomy/carotid artery stenting, and is now ready for clinical use.
Incorporating this validated risk estimate into management plans should improve early decision making at the index emergency visit regarding benefits of hospital admission, timing of investigations, and prioritization of specialist referral.
Excluded: had neurological deficits for more than 24 hours (that is, a stroke according to the World Health Organizationí s definition), had a decreased level of consciousness from their baseline (that is, Glasgow Coma Scale <15 in previously cognitively normal patients), had an alternative diagnosis (for example, hypoglycemia, seizure, electrolyte imbalance, or migraine), presented more than seven days after onset of the neurological symptoms, or were treated with tissue plasminogen activator or embolectomy for an acute stroke.
7607 consecutively enrolled adult patients (80.6% of all potentially eligible patients)108 (1.4%) had a subsequent stroke within 7d
83 (1.1%) had carotid endarterectomy/carotid artery stenting within 7d
9 patients had both within 7d leaving 182 with outcomes
Low risk: 16.3% of patients, 7d risk of CVA or carotid procedure ≤0.5%;
Medium risk: 72.1% of patients, 7drisk of CVA or carotid procedure 2.3%;
High Risk: 11.6% of patients, 7drisk of CVA or carotid procedure: 5.9%;
Authors recommend Head CT and routine follow-up for low risk patients, CTA head/neck for medium risk and with rapid follow-up.
BIG PEARL: avoid intubation in severe metabolic acidosis patients, if possible, allow them to continue their compensatory breathing until you can correct underlying problem (especially true for easily fixable problems like DKA, less so for severe sepsis).
Smaller pearl: cause of acidosis as important as the actual number in determining prognosis, low pH from COPD, DKA or even salicylate poisoning easier to resuscitate and better prognosis than septic shock.
Scant evidence for bicarb boluses but Weingart doesn’t use because if patient is already maxed out on respiratory compensation, the added bicarb simply gets converted to CO2 that can no longer be blown off.
Weingart does use 3 amps of NaBicarb in D5W drip for salicylate poisoning, but not for DKA
Place on Vent with NIV mask with pressure support to augment respiratory drive before intubation to determine the minute ventilation that needs to be matched after intubation.
Once patient is induced but before paralysis occurs, patient should be switch to vent settings RR 12, TV 8cc/kg, this lower RR should reduce risk of gastric dissension and vomiting.
Once patient is intubated, empiric settings RR 30, TV 8cc/kg.
Ask RT to confirm patient is exhaling whatever they are inhaling and not air stacking due to the high RR.
If patient is air stacking, switch to the square breathing curve with a high inspiratory flow rate.
27 918 patient encounters (16 212 women [58.1%]; mean [SD] age, 58.7 [15.2] years) were included in the study.
Of patients with an initial troponin measurement below the level of detection, 14 459 (51.8%) were discharged after a single troponin measurement, and 13 459 (48.2%) underwent serial troponin tests.
After adjustment for cardiac risk factors and comorbidities, there was no statistically significant difference in the primary outcome of acute myocardial infarction or cardiac mortality within 30 days between the 2 groups (single troponin, 56 [0.4%] vs serial troponin, 52 [0.4%]; adjusted odds ratio, 1.41 [95% CI, 0.96-2.07]).
Patients discharged after a single troponin test had lower rates of coronary artery bypass graft (adjusted odds ratio, 0.24 [95% CI, 0.11-0.48]) and invasive coronary angiography (adjusted odds ratio, 0.46 [95% CI, 0.38-0.56]).
This study suggests that patients are routinely discharged from the ED after a single negative troponin test result, and when compared with serial troponin testing, a single troponin test appears safe based on current physician decision-making, with no difference in rates of 30-day cardiac mortality and acute myocardial infarction, which are low in both groups.
Didn’t realize that addition of anticoagulant therapy to anti platelet therapy has been shown to improve outcomes after ACS but is not routinely done due to increased risk of bleeding.
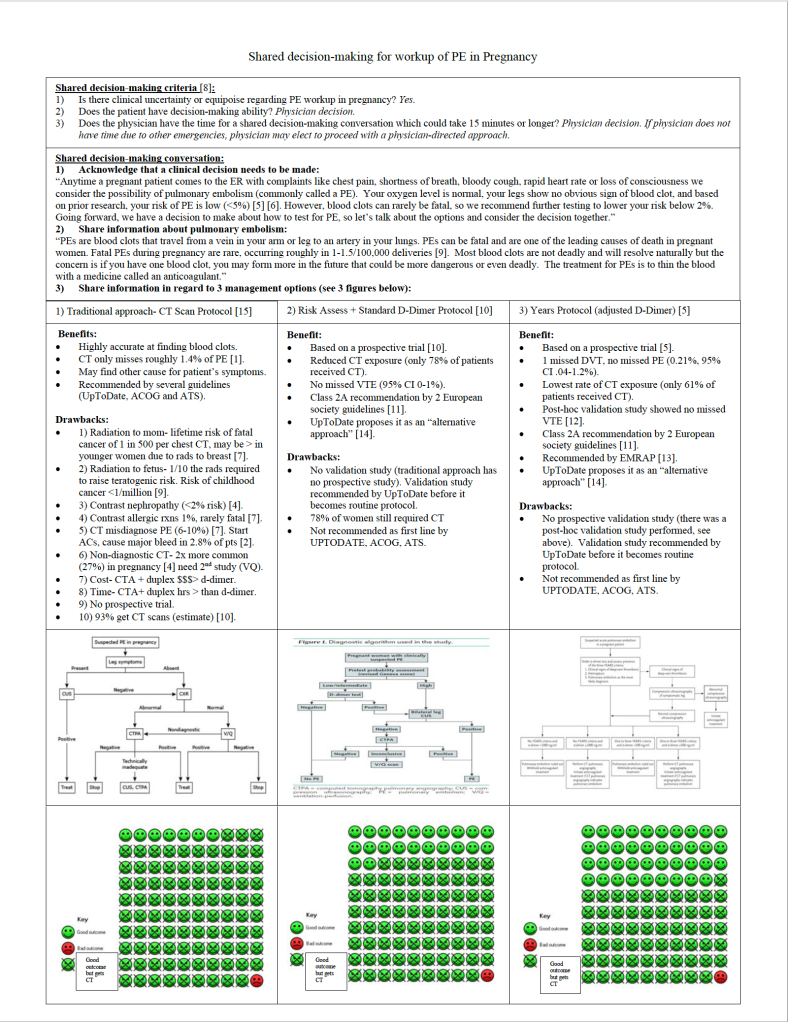
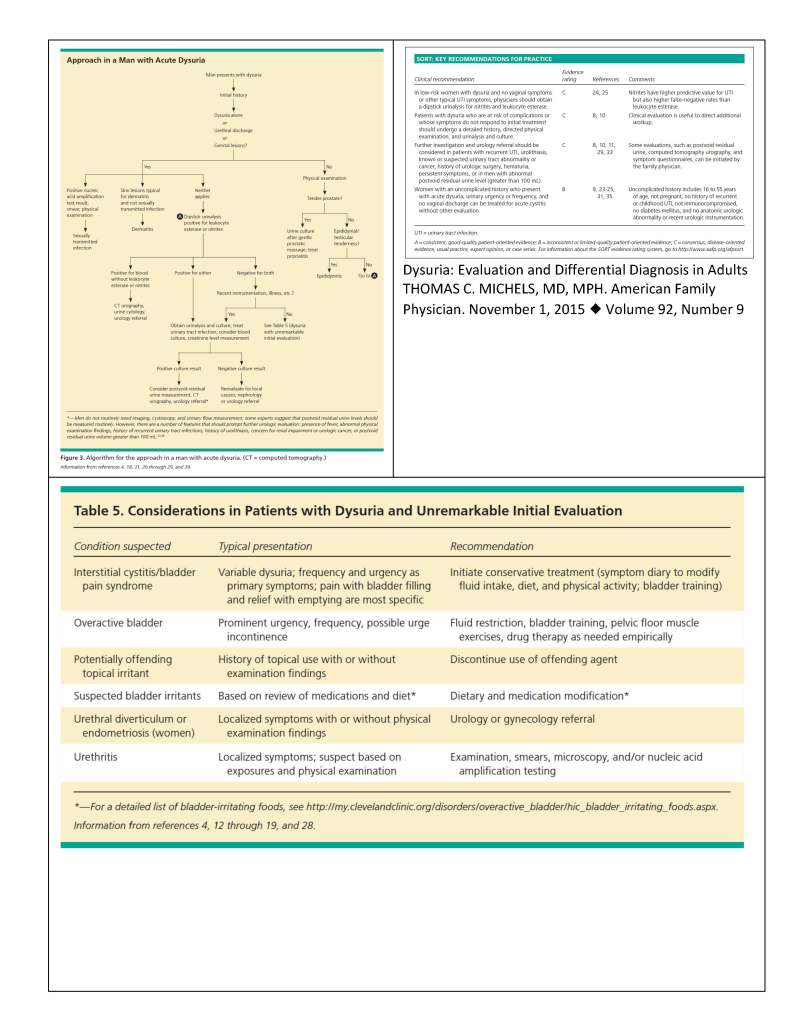
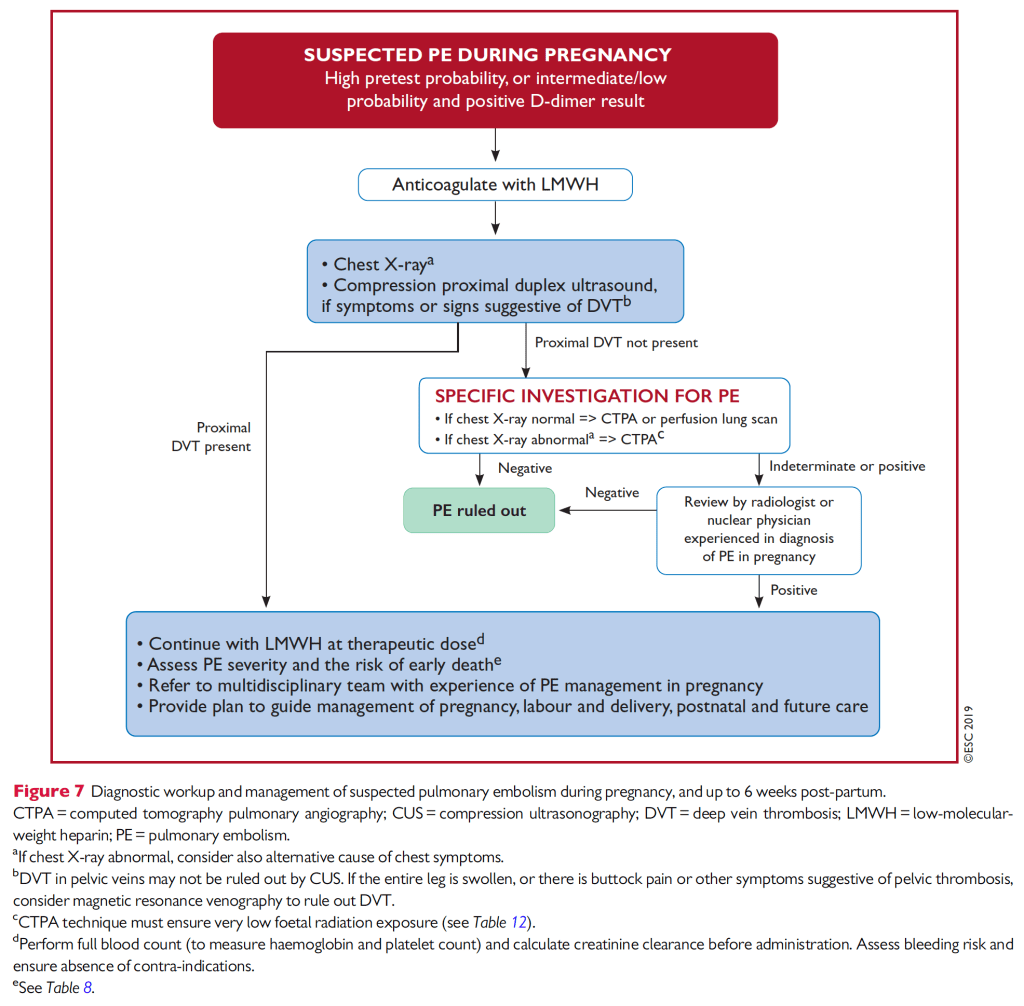
Despite physiologic reasons why pregnant women would be at increased risk for PE (hypercoagulable state, venous stasis ), they surprisingly have roughly the same rate of diagnosed PE (32/100k) as the general population of women under the age of 40 according to Olmsted County data published by Heit and referenced by Kline, as long as you remove isolated DVT and postpartum state. Early postpartum state, on the other hand, has roughly a 10 fold increased risk (421/100k). Normal physiologic changes of pregnancy such as dyspnea, leg swelling, increased resting heart rate can all mimic PE. For this reason, as well as the specter of missing potentially deadly PE that harms two patients simultaneously, physicians have been found to overtest for VTE, with a rate of positive VTE around 4% (Kline 2014 and van der Pol 2019), which is 1/3 the rate of positive workups in the general population. To make matters worse, the traditional workup, endorsed by American Thoracic Society and ACOG in 2011, did not use risk assessment or D-Dimer in pregnant patients due to lack of prospective trials and instead went directly to duplex and CT or VQ. As Kline breaks down in his 2015 review of the workup for PE, the risks to pregnant moms from CT not only include the 1 in 500 chance of a fatal cancer, but also the 26% chance of a non-diagnostic study study (higher cardiac output and higher plasma volume during pregnancy make the timing of the bolus less reliable), and the 6-10% chance of a false positive study in low risk populations which subjects the patient to 3-6 months of anticoagulation.
For many emergency clinicians, the NEJM publication of van der Pol’s Pregnancy-Adapted Years Algorithm for Diagnosis of Suspected Pulmonary Embolism in 2019 was all we needed to begin offering patients an alternative to mandatory CT for all low risk PE workup. Righini had already published a Pregnancy PE protocol that employed risk assessment with a normal D-Dimer but unfortunately this only reduced CT utilization in 22% of pregnant patients.
The challenge with using Years to guide management is that some leading expert guidelines (ACOG and ATS) which have not been updated since 2011 still recommend CT for all or, in the case of UpToDate, are calling for a second validation study before recommending the Years approach. Years was validated by the Righini group in a post-hoc fashion and showed a 0% miss rate but a prospective validation study is not yet published.
So what is a pregnant patient and a well-intentioned physician to do?
Shared decision-making!
Here is my attempt at a shared decision-making script to help patients decide what feels best for them.
COVID-19 is a potentially critical illness associated with a variety of ECG abnormalities, with up to 90%of critically ill patients demonstrating at least one abnormality.
The ECG abnormalities in COVID-19 may be due to cytokine storm, hypoxic injury, electrolyte abnormalities, plaque rupture, coronary spasm, microthrombi, or direct endothelial or myocardial injury.
While sinus tachycardia is the most common abnormality, others include supraventricular tachycardias such as atrial fibrillation or flutter, ventricular arrhythmias such as ventricular tachycardia or fibrillation, various bradycardias, interval and axis changes, and ST segment and T wave changes.
Several ECG presentations are associated with poor outcome, including atrial fibrillation, QT interval prolonga-tion, ST segment and T wave changes, and ventricular tachycardia/fibrillation.
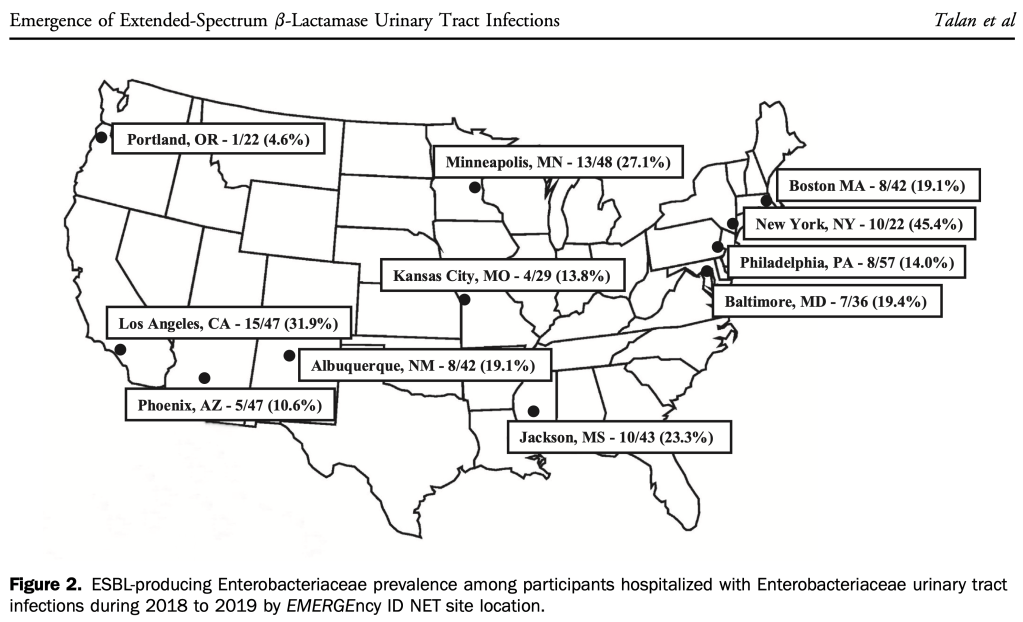
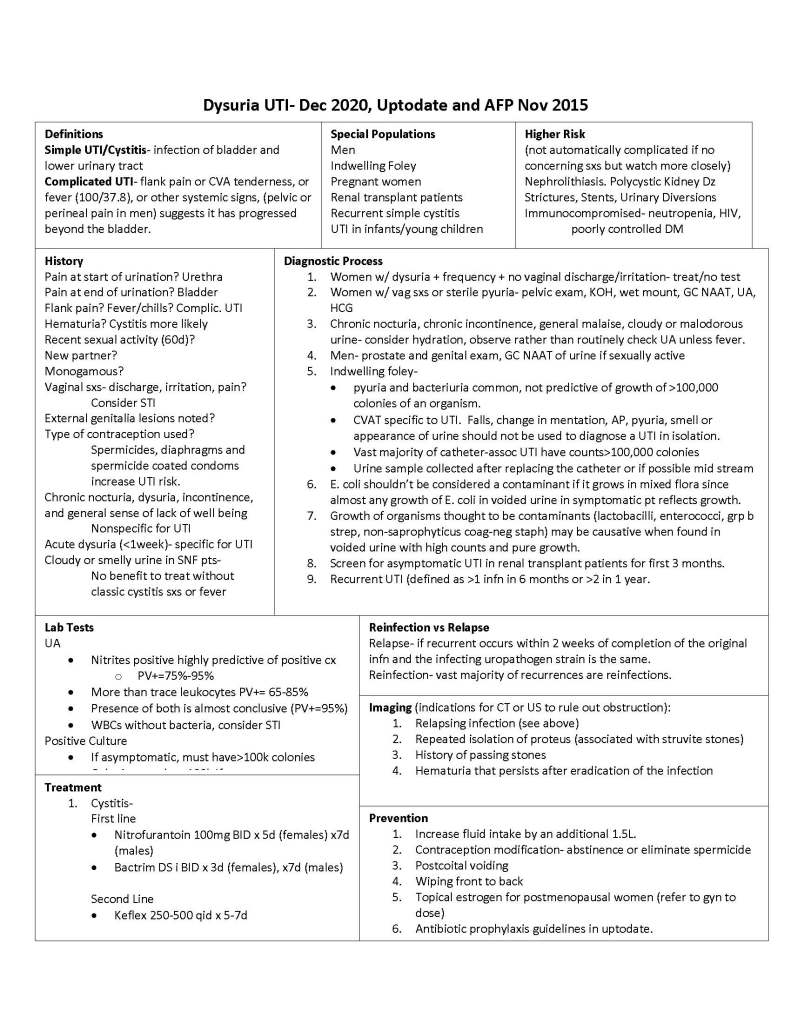
Growing percentage of hospitalized patients with UTI have resistance to ceftriaxone (17% overall during the study period of 2018-2019) but some areas of the country are much higher.
Authors cite a 2009 study by Kumar that showed a 5 fold reduction in survival for septic shock patients who received initial empiric antibiotics that lacked in-vitro activity against the offending pathogen.
24% resistance to Ceftriaxone among Enterobact. isolates, 3% resistance to Pip-Taz.
Among ESBL-confirmed isolates, resistance to Pip-Taz was 18%.
Resistance>10% is the recommended trigger to broaden coverage.
Authors recommend a carbapenem or amikacin for hospitalized UTI and acknowledge there is no PO option for outpatients.
Uptodate recommends a carbapenem for septic shock patients with suspected UTI.
Per Johnson, Acute Pyelonephritis in Adults (NEJM 2018), choose an antibiotic of a different class for initial empirical treatment of pyelonephritis when the local resistance rate to the antibiotic being considered exceeds 10%, with a lower threshold for critically ill patients.
Bottom-line: know your hospital’s antibiogram, upgrade from Ceftriaxome if resistance is >10%.
Although studies from NYC early in the pandemic showed a high prevalence of prior Covid infection (31.2% and 46%) among ED providers, this study from San Francisco showed a low seroprevalence of antibodies (1%).
The Pneumonia Severity Index (PSI) and CURB-65 decision aids can support clinical judgement by identifying patients at low risk of mortality who may be appropriate for outpatient treatment. Although both decision aids are acceptable, the PSI is supported by a larger body of evidence and is preferred by other society guidelines (ATS/IDSA 2019 guidelines).
Given the lack of evidence, the decision to administer a single dose of parenteral antibiotics prior to oral therapy should be guided by patient risk profile and preferences (Consensus recommendation).
Providers completed HEAR assessments on 4979 patients and HEAR scores<1 occurred in 9.0% (447/4979) of patients. Among these patients, MACE at 30 days occurred in 0.9% (4/447; 95% CI 0.2% to 2.3%) with two deaths, two MIs and 0 revascularisations. The sensitivity and negative predictive value for MACE in the HEAR <1 was 97.8% (95%CI 94.5% to 99.4%) and 99.1% (95% CI 97.7% to 99.8%), respectively, and were not improved by troponin testing. Troponin testing in patients with HEAR <1 correctly reclassifi ed two patients diagnosed with MACE, and was elevated among seven patients without MACE yielding an NRI of 0.9% (95%CI −0.7 to 2.4%).
Conclusion These data suggest that patients with HEAR scores of 0 and 1 represent a very low risk group that may not require troponin testing to achieve a missed MACE rate <1%.
“Patients with very low to low risk (-3 to 0 points) can be discharged home with a low event rate
Patients with intermediate risk (1-3 points) have an 8% risk of bad outcome at 30 days (0.1% risk of death). Shared decision making is appropriate here.
Patients with higher risk (> 4 points) probably should be admitted in consideration of their high rate of bad outcomes, despite the low diagnostic yield.”
Cranial Burr Hole (emergent epidural or subdural evacuation)- Jess Mason and David Beffa
“Steps of procedure (to be done on the side of the blown pupil) Knowing the anatomy from the CT head will be helpful. You can measure the thickness of the skull table so you know approximately how deep you need to go.
Prepare the site using sterile technique.
If no CT is available and the procedure is done blind, the entry site is 2 cm superior and 2 cm anterior to the tragus on the ipsilateral side of the blown pupil
Have an assistant hold the patient’s head hard and steady during the procedure.
Make a 3-5 cm vertical skin incision down to bone.
Insert self-retaining scalp retractor to expose periosteum.
Expose the skull and elevate the periosteum using the periosteal elevator.
Trephination technique varies by device. You may feel a change from smooth to rough as you move from outer to inner skull table.
An epidural hematoma will start to drain when you get through the inner table. If a subdural hematoma is present, an additional step is needed which involves a 3-sided incision to form a flap in the dura mater.
Place a sterile dressing.”
Eye vs Brain– Evie Marcolini, MD and Anand Swaminathan, MD
Diplopia easy to distinguish, monocular diplopia most likely ocular pathology, whereas binocular diplopia is usually CNS .
Cranial Nerve Palsy: 3, 4, 6 (think SAH when CN 3 palsy, abduction only -no adduction, supraduction or infraduction, with acute HA)
Internuclear Ophthalmoplegia
Hard to distinguish between ocular and CNS pathology with painless, non-red, non-post-op, atraumatic monocular vision loss!
ED patients being evaluated for acute coronary syndrome shows that HEART scores of 0–5 are generally at low risk for death or acute myocardial infarction within 30 days, but points obtained from different components of the score are associated with different risk elevations.
Specifically, any points obtained due to elevated troponin values (even in the intermediate range, cor-responding to troponin = 1 or 2 points) as well as ST deviations (cor-responding to ECG = 2 points) were predictive of higher risk than an equal number of points obtained from the other components.
Although the HEART score still reliably identifies low-risk ED patients, further research on refinements to the score (eg, allocating additional points to the troponin component and correspondingly recalibrating the cut-off score to better match a 1% acceptable risk threshold for further testing) may better assess the risks facing patients with suspected acute coronary syndrome, allow for better risk stratification of patients with chest pain, and merits further study.
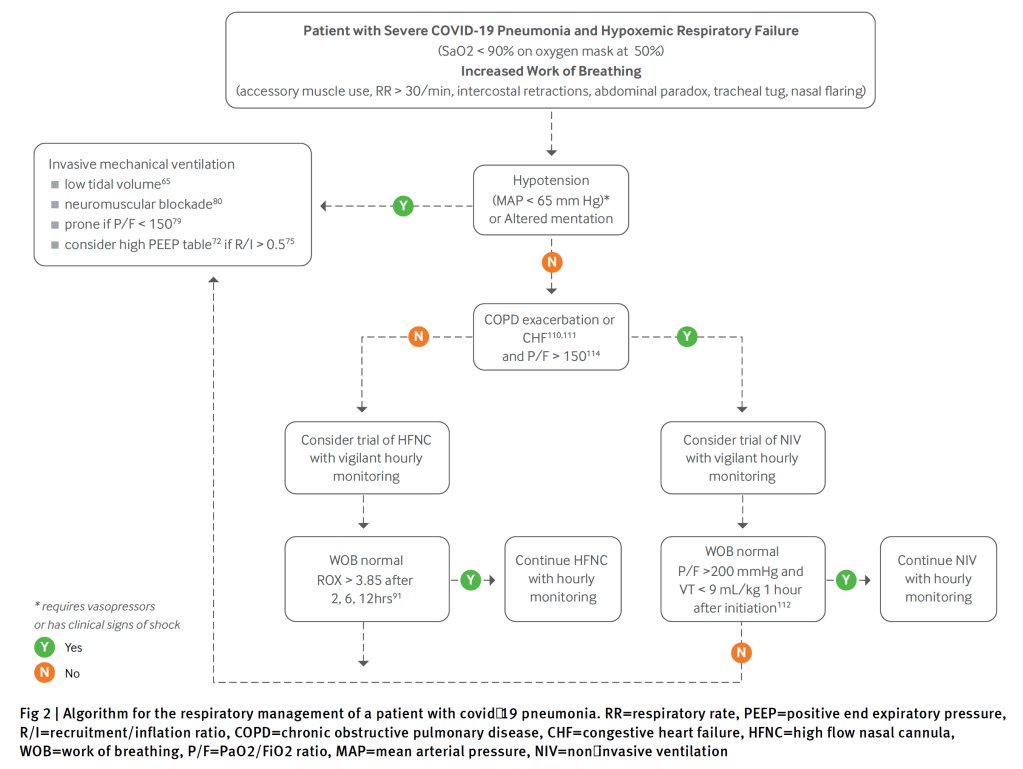
Awake prone positioning was not associated with lower intubation rates. Caution is necessary before widespread adoption of this technique, pending results of clinical trials.
“These data ought not change our current practice of obtaining blood cultures before antibiotic administration. As illness severity increases, the relative importance of early antibiotic administration likely takes precedence over the potential identification of a causative organism. The take-home point for ED clinicians is that timely antibiotic administration should not be delayed because of difficulties in obtaining appropriate samples for blood cultures.”
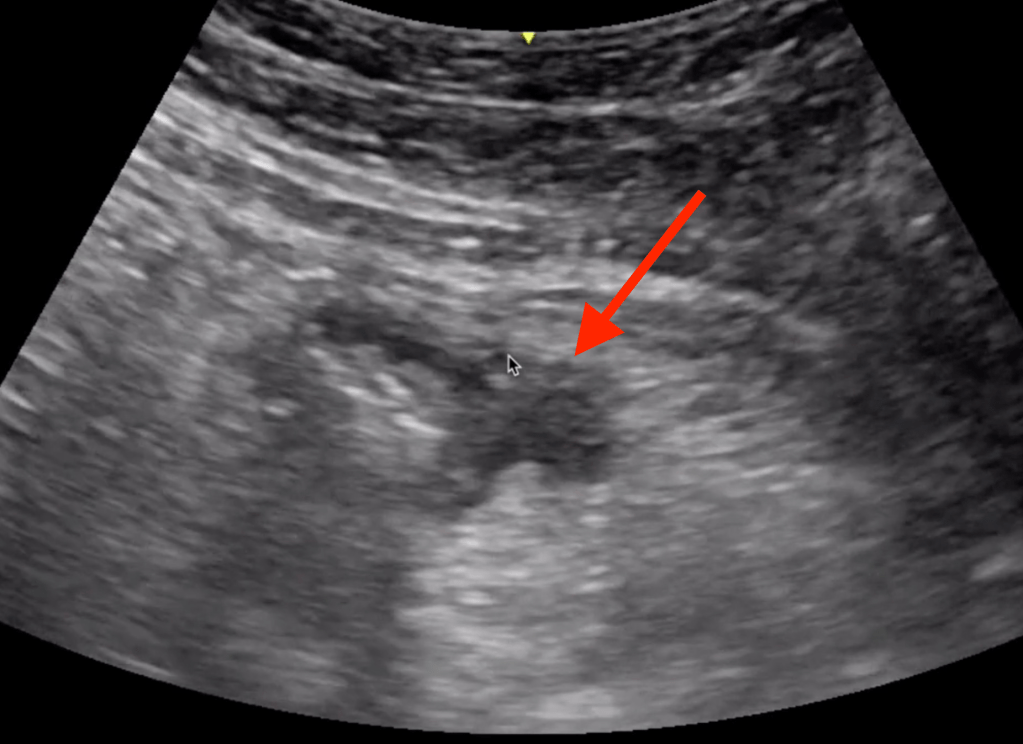
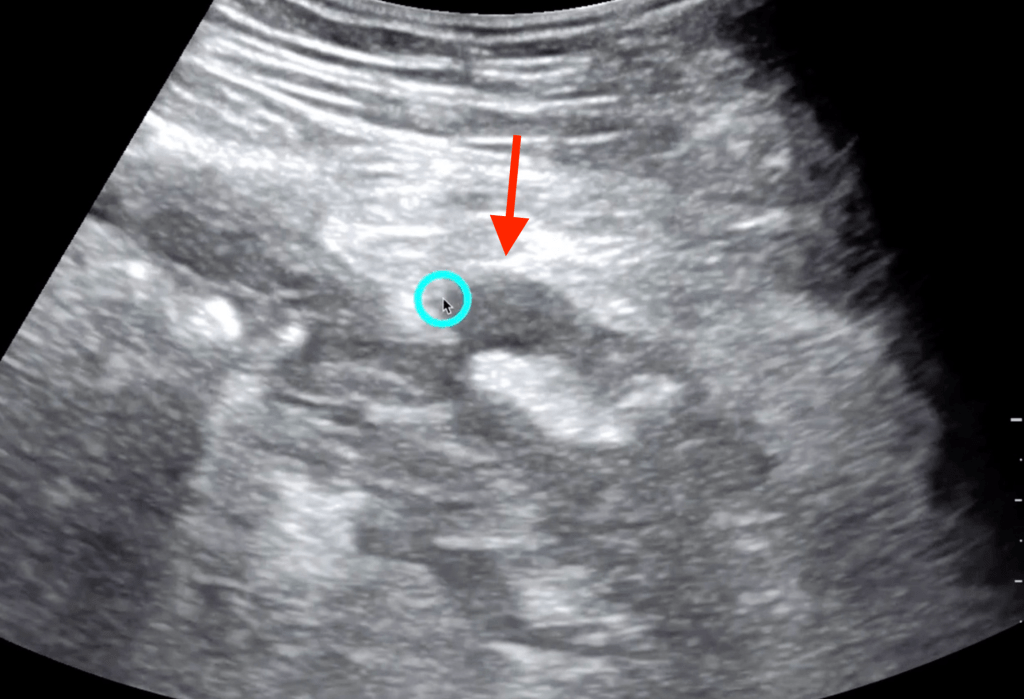
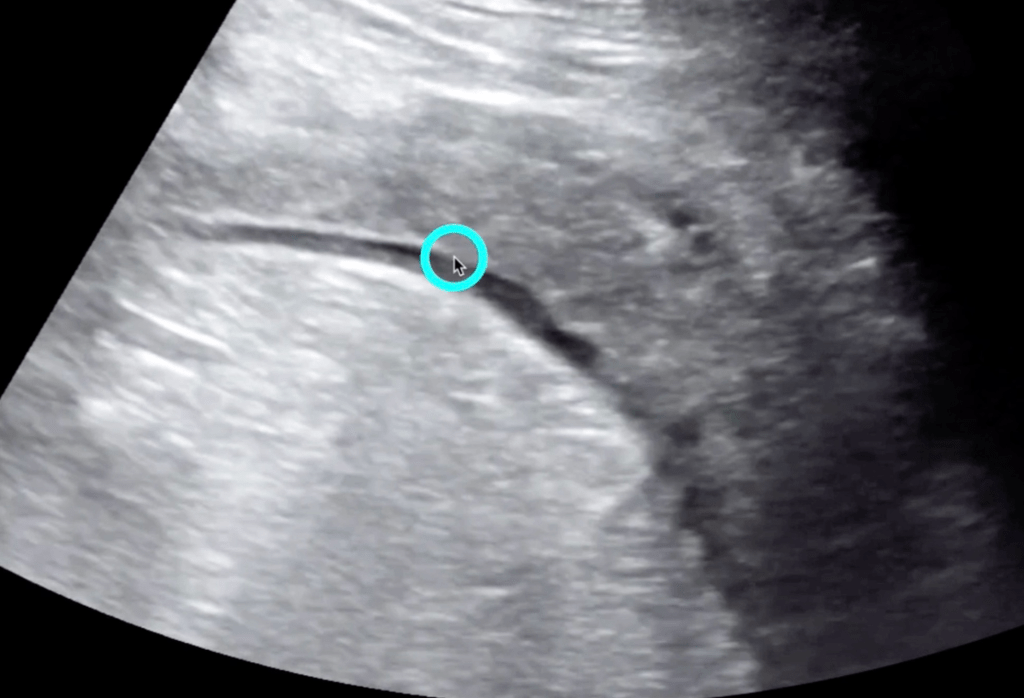
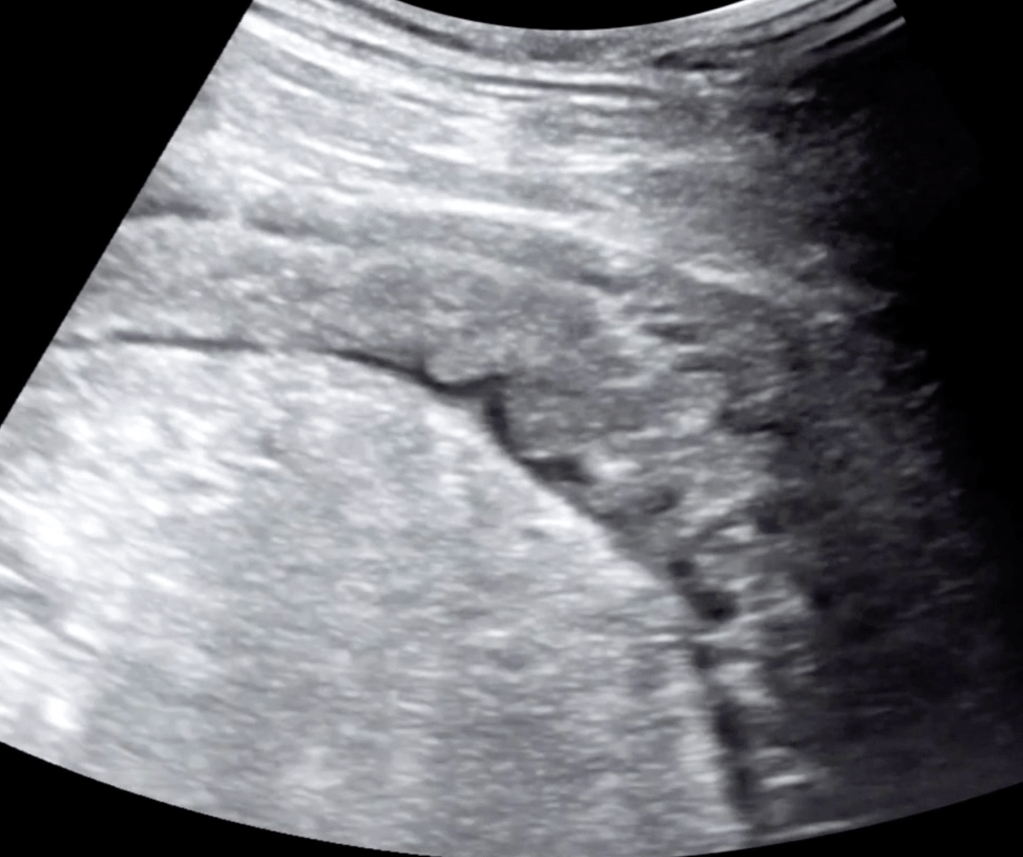
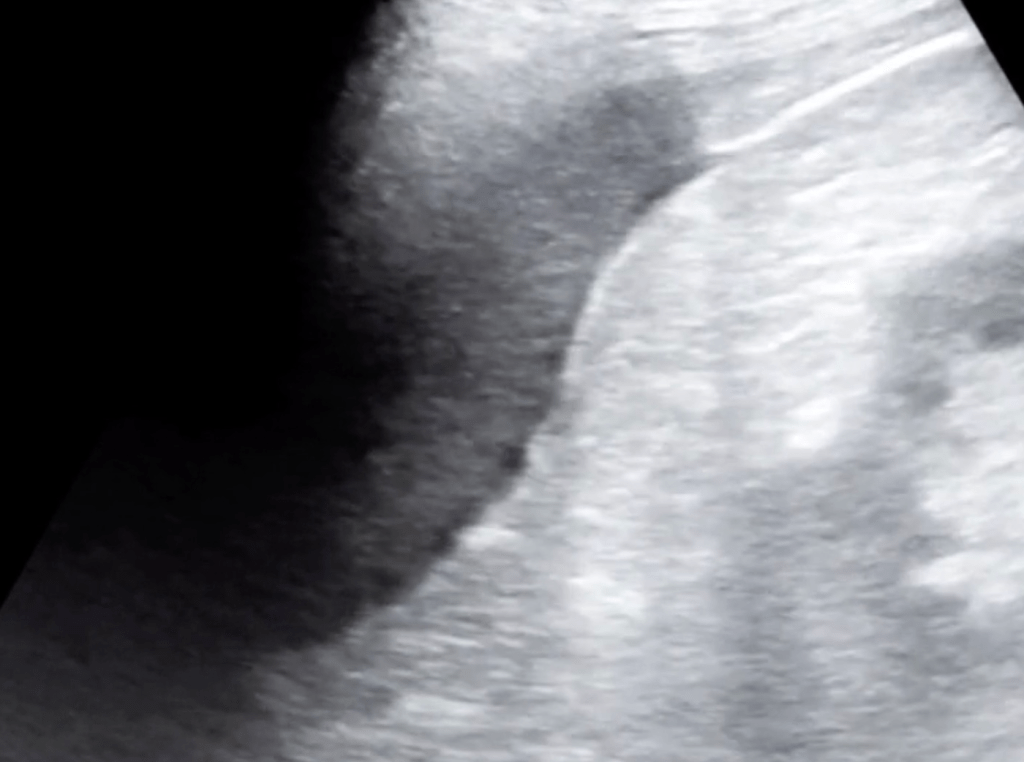
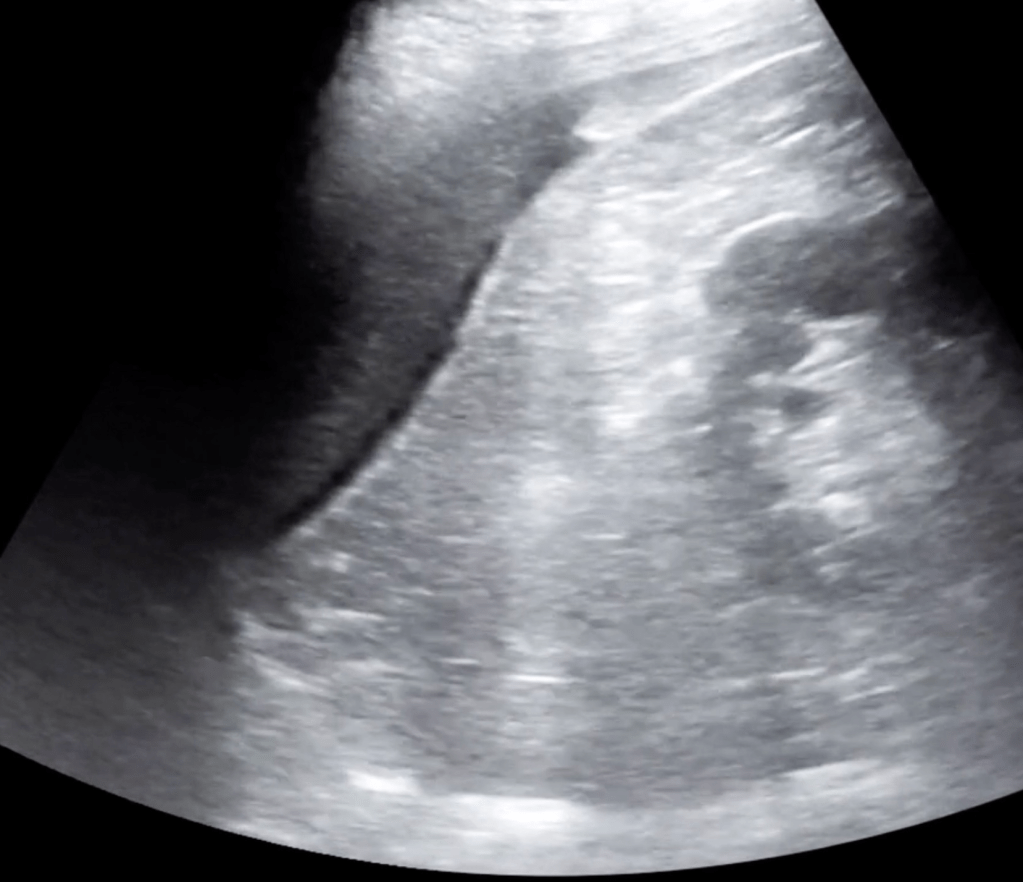
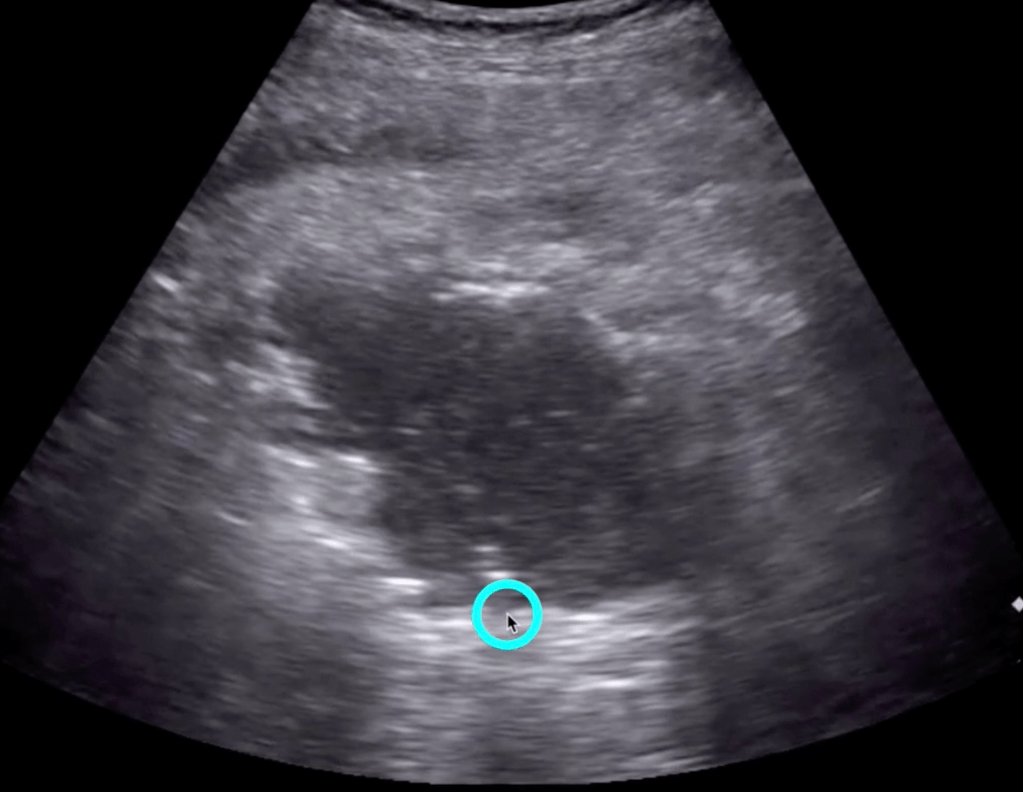
“Compared with CT, point-of-care ultrasonography had a sensitivity of 92% (95%confidence interval 88% to 96%), specificity of 97% (95% confidence interval 94% to 99%), positive predictive value of 94% (95%confidence interval 90% to 97%), and negative predictive value of 96% (93% to 98%) in the diagnosis of diverticulitis.”
Check out the new 5 minute Sono Diverticulitis video later in this post
In the studies limited to emergency physicians, ocular point-of-care ultrasonography had a pooled sensitivity of 92% (95% CI 67% to 99%) and specificity of 91%(95% CI 85% to 95%).
The authors found emergency practitioner diagnosis of other posterior chamber abnormalities, including lens dislocation, globe rupture, intraocular foreign body, and vit-reous hemorrhage, using point-of-care ultrasonography to be accu-rate, but with wide CIs.
The safety of point-of-care ultrasonography for assessment of a ruptured globe or an intraocular foreign body through a penetrating injury has not been established, and using it is not recommended.
The two key interventions were pharmacist review of medications and physical therapy consult.
Compared with usual care participants (n=55), intervention participants (n=55) were half as likely to experience a subsequent ED visit (adjusted incidence rate ratio 0.47 [95% CI 0.29 to 0.74]) and one third as likely to have fall-related ED visits (adjusted incidence rate ratio 0.34 [95% CI 0.15 to 0.76]) within 6 months.
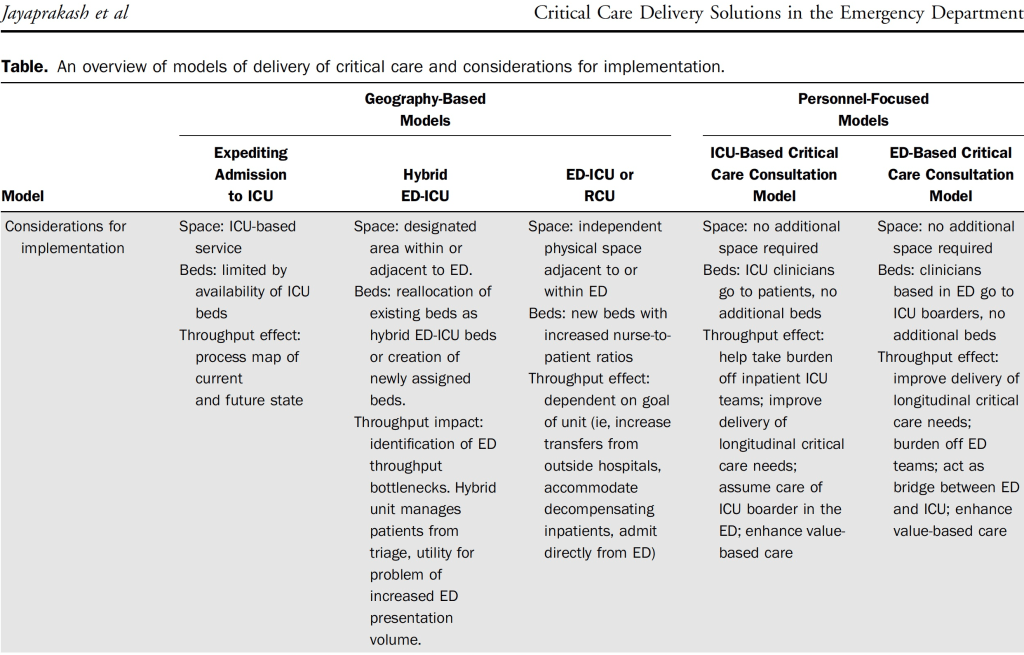
An ED length of stay of greater than 6 hours is estimated to be associated with a 10% increase in hospital mortality.
A primary determinant (of ICU boarding) is ineffective throughput, reflective of a limited supply of beds, inadequate staffing for the available beds, or ineffective use of beds.
5 models to respond to boarding, easiest is the far right Ed-Base Critical Care Consultation Model.
In 96% of cases (335/349) in which one or more modifiable risk factors were present, they were not diagnosed. The most commonly missed risk factors were high-risk medications and visual acuity deficits.
Overall, 19 studies (11 randomized; 8 nonrandomized) of 241 138 participants from 7 countries and various health care settings (hospital-based and community-based) were included.
In this study, use of ibuprofen vs acetaminophen for the treatment of fever or pain in children younger than 2 years was associated with reduced temperature and less pain within the first 24 hours of treatment, with equivalent safety.
Another study showing the superiority of Droperidol for agitation: adequate sedation in 15 minutes better with Droperidol (64%) than Ziprasidone (35%) or Lorazepam (29%) and lower incidence of respiratory depression with Droperidol (12%) than with Ziprasidone (36%) or Lorazepam (48%).
In a low prevalence setting (pretest probability 5%) ADD-RS >/=1 has a failure rate of 0.8% and an ADD-RS of 2 plus a normal D-dimer has a failure rate of 0.1%.
For a higher prevalence of AD (20% pretest probability), failure rate of ADD-RS alone would be 3.8%, but when adding a negative D-Dimer, the failure rate of 1 is 0.2% and 2 is 0.5%.
In summary, in a 5% pretest probability group, ADD-RS=0 rules out AD or ADD-RS=1 plus a negative D-Dimer rules out AD and in a 20% pretest probability group, an ADD-RS=0 or 1 plus a negative D-Dimer rules out AD.
HS-troponin will replace traditional older troponin assays.
This synopsis of a study in Heart showed better than 98% sensitivity for MI with a 0/1 hour protocol if pain was ❤ hours or a single troponin if pain was >3 hours.
The authors cite that a 2% miss rate may not be acceptable in the US but it is just one more study which reinforces the inevitable move toward high-sensitivity troponin.
Both pieces agree NSAIDS work well for pain, equivalent to opiates in multiple studies.
Both agree that risk of fracture healing is not significant when NSAIDS are used for first 72 hours.
Pro NSAID article argues the risk of fracture healing occurs if NSAIDS are used for>30 days, Con article says risk occurs after 3 days.
Annals explanation: “Tubercular lymphadenitis presents as a nontender, slowly progressive, unilateral swelling most commonly in the cervical region, classically named scrofula. Because of softer cartilage in children’s airways, mediastinal lymphadenitis can cause significant morbidity and even mortality owing to mass effect on the esophagus and tracheobronchial tree.”
Annals explanation: “Pott’s puffy tumor. A subperiosteal abscess with associated osteomyelitis of the frontal bone, often referred to as a Pott’s puffy tumor, is a rare entity in children. It can affect children of all ages, but most frequently affects adolescents. It is often a complication of acute bacterial rhinosinusitis, but has also been associated with trauma, surgery, drug use, mastoiditis, and dental infections. Clinical features include fever, headache, and forehead or scalp swelling and tenderness. Patients may also present with vomiting, lethargy, seizures, or altered mental status, depending on the extent of intracranial involvement. Diagnosis is clinical and radiographic, most commonly with CT, magnetic resonance imaging, or both. Management includes antimicrobials in addition to surgical drainage of the abscess, which is commonly polymicrobial with streptococcal, staphylococcal, and anaerobic organisms. The patient underwent operative drainage shortly after diagnosis and was maintained with broad-spectrum antibiotics for several days. She has since made a full recovery.”
Randomized trial where control group got usual fluid care strategy and intervention arm got a restrictive fluid strategy driven by passive leg raise and measurement of stroke volume with a noninvasive bioreactance electrode system. The restrictive fluid group had half as many patients requiring mechanical ventilation and one third as many patients requiring dialysis.
Currently many EDs don’t have the SV technology but it is a good reminder that less fluid is probably better.
Poor man’s PLR is to measure the pulse pressure (systolic bp-diastolic bp) 30-90 seconds after performing PLR. PLR done by starting patient in 45 degree upright position and then laying them flat and raising legs to 45 degrees.
Another study showing the benefit of hypertonic saline bolus to treat symptomatic hyponatremia. Unfortunately many hospitals do not allow hypertonic saline boluses, instead insisting on slow infusions of hypertonic saline not to exceed 30ml/hr, or they insist on using a central line despite studies cited by UPTODATE showing peripheral infusion is safe (Incidence of Adverse Events During Peripheral Administration of Sodium Chloride J Intensive Care Med. 2018 and Safety of Continuous Peripheral Infusion of 3% Sodium Chloride Solution in Neurocritical Care Patients Am J Crit Care. 2016).
I was able to get my hospital to agree to the 100cc hypertonic saline bolus after citing the articles and blog posts referenced here, citing that UPTODATE recommends rapid intermittent bolus therapy for severe symptomatic hyponatremia, and explaining that without the bolus option physicians are forced to use normal saline which can paradoxically lower the already low sodium concentration in SIADH patients because the saline infusion induces a diuresis of concentrated urine which (read the explanation in this UPTODATE chapter).
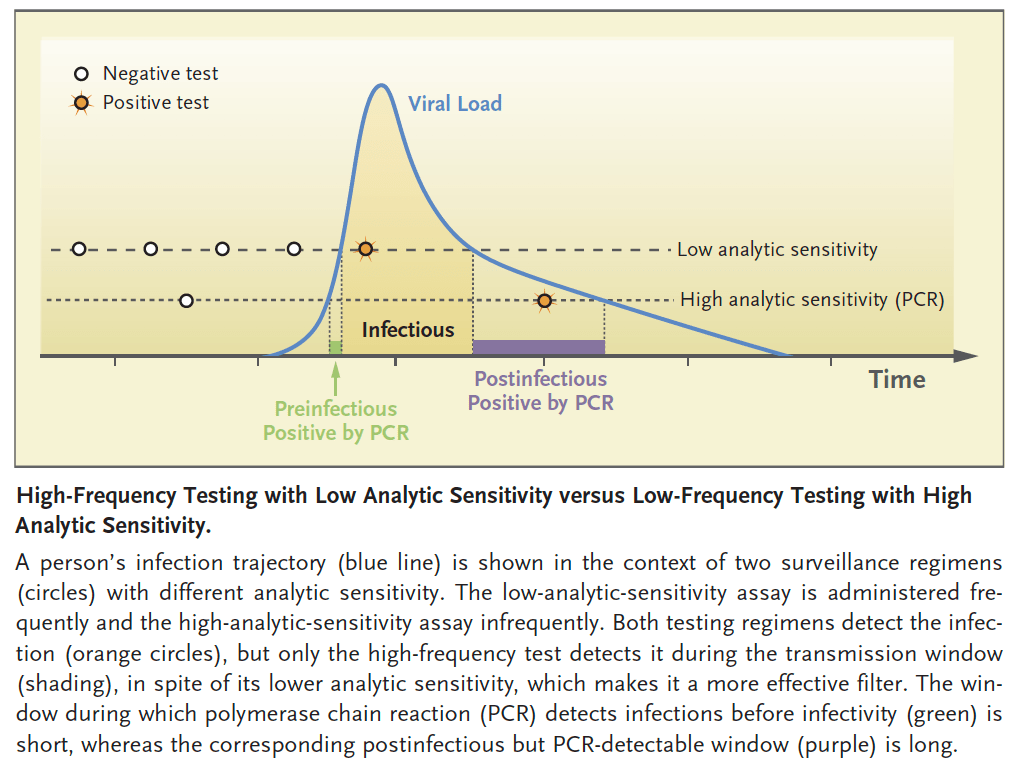
rather than focus on super sensitive PCR tests that are more expensive and have a slower turnaround, choose less sensitive antigen tests which cost <$5 and can be done at home or point of care with quick results.
the key is frequent testing to catch someone early in their period of transmissibility to break chain of spread.
since the trajectory of virus replication is exponential at beginning, the difference in time between when a low sensitivity and high sensitivity test become positive could be a matter of hours.
Proactively stating, “before we go on, I need to tell you something about me, I don’t do guilt,” can help ease a patient’s anxiety about answering questions of health behaviors (e.g. drugs, tobacco, alcohol, etc).