Of the 514/1081 (47.5%) infants who met the PECARN low-risk criteria, 1/514 (0.2%, 95% confidence interval [CI] 0.005% to 1.1%), had clinically important traumatic brain injuries1/514 (0.2%, 95% confidence interval [CI] 0.005% to 1.1%)
CONCLUSIONS: Moderate to high certainty evidence shows that non-inhaled medical cannabis or cannabinoids results in a small to very small improvement in pain relief, physical functioning, and sleep quality among patients with chronic pain, along with several transient adverse side effects, compared with placebo. The accompanying BMJ Rapid Recommendation provides contextualised guidance based on this body of evidence.
Use a body bag (the same ones used to transport patients to the morgue) to cool patient rapidly in 20-30 minutes. Put patient in the bag and fill with ice and water.
Pulse ox waveform depends on perfusion index (ratio of pulsatile blood over non-pulsatile blood), <0.5 has a poor waveform.
Low cardiac output (cardiogenic shock) or vasoconstriction (hemorrhagic shock) cause lower perfusion index and poor waveform, while septic shock tends to be warm and hypotensive due to poor vasoconstriction.
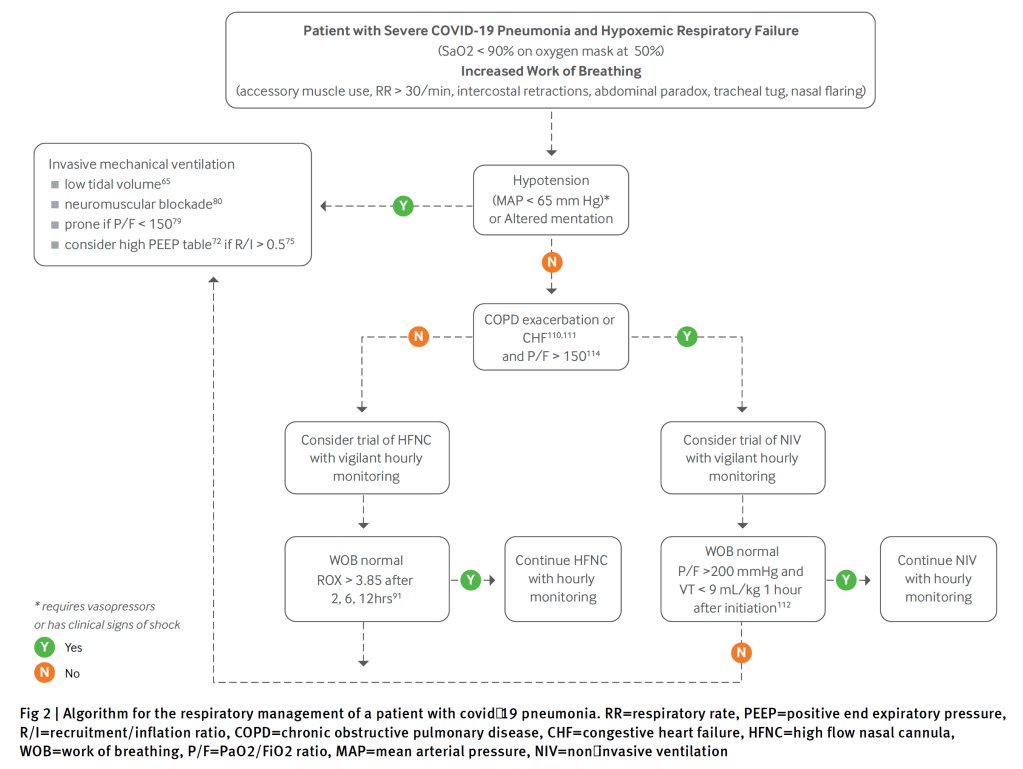
For patients with COVID-19 pneumonia and acute hypoxemic respiratory failure, CPAP reduced the need for intubation compared to conventional oxygen therapy. However, HFNO did not reduce the need for intubation compared to conventional oxygen therapy. Neither intervention showed a statistically significant mortality benefit compared to conventional oxygen therapy, however, the study was not powered for this outcome. Although the conclusion of the trial is CPAP > HFNO > COT, there may be some scenarios where HFNO > CPAP to reduce adverse events (i.e awake prone positioning, patient nutrition, etc).
This is the highest-level evidence we have to date on awake prone positioning. In this trial of patients with hypoxemic respiratory failure due to COVID-19, awake prone positioning reduced the incidence of treatment failure (intubation and death), which was primarily driven by decreased intubation compared to standard care. Not only was there no signal of harm from awake prone positioning, but even longer durations of awake prone positioning (>8hrs/day) were associated with a lower risk of treatment failure.
Abx reduce complications in culture positive asymptomatic bacteriuria, which is a subset of asymptomatic bacteriuria before culture performed.
Uptodate makes no mention of checking UA in pregnant patients with abnormal vaginal bleeding. I was taught in residency to do this to rule out occult UTI as a cause of threatened miscarriage, then the UA always comes back with a few wbcs or bacteria and I feel obliged to treat. I’m gonna stop!
ED clinicians had only moderate agreement with research HEART scores. Combined with uncertainties regarding accuracy in predicting major adverse cardiac events, we urge caution in the widespread use of the HEART score as the sole determinant of ED disposition.
Showed a benefit to therapeutic anticoagulation in non-critically ill but this benefit was small per Uptodate and other studies have not shown a benefit and the incidence of thromboembolic events in hospitalized patients are lower now than earlier in the pandemic, possibly related to the use of steroids and tocilizumab.
In CRITICALLY ILL patients with COVID-19, an initial strategy of therapeutic-dose anticoagulation is not associated with a greater probability of survival to hospital discharge or a greater number of days free of cardiovascular or respiratory organ support vs usual-care pharmacologic thromboprophylaxis
In NON-CRITICALLY ILL patients with COVID-19, an initial strategy of therapeutic-dose anticoagulation is associated with a greater probability of survival to hospital discharge or a greater number of days free of cardiovascular or respiratory organ support vs usual-care pharmacologic thromboprophylaxis
In NON-CRITICALLY ILL patients with COVID-19, there is a clear signal of benefit, however with all the protocol violations and variable treatment arms it would still be reasonable to discuss with the inpatient team to help guide the decision (Although, in my practice and at my institution most patients who are not critically ill and don’t have contraindications, we have changed our protocols to full dose anticoagulation).
In this retrospective study of patients receiving blood cultures at a hospital in The Netherlands, we found that 6.3% of patients with SARS- CoV-2 had positive blood cultures and all were considered contaminated. Overall bacterial coinfection using other diagnostics was 1.4%. This suggests that in patients known to have SARS- CoV-2, blood cultures are unlikely to be of use.
Procalcitonin and the Pneumonia Severity Index seem most promising to recognise patients at risk for severe outcome of COVID-19 when presenting to the ED.
A traumatic arthrotomy is a laceration that extends into the joint capsule exposing the intra-articular surface to the environment. It is important to identify, as operative washout, debridement and proper closure of the joint capsule is required.
Instill saline into the joint and see if it leaks out through the laceration. Leakage of saline means you have an arthrotomy.
For the knee, a load of 194 mL achieves 95% sensitivity.
Keese GR, Boody AR, Wongworawat MD, Jobe CM. The Accuracy of the Saline Load Test in the Diagnosis of Traumatic Knee Arthrotomies. Journal of Orthopaedic Trauma. 2007;21(7):442-443. doi: 10.1097/BOT.0b013e31812e5186.
Sensitivity of anterior nares is lower (82-88%) than nasopharyngeal (98%) but in a population with 10% positivity, the negative predictive value is still greater than 98%.
Evolving definition of the previously termed conversion disorder, now called functional neurological disorder (FND) in which there is loss of motor or sensory or presence of seizure activity without any evidence of structural pathology.
Can be thought of as a software problem rather than a hardware problem
Two useful tests are hip abductor sign (hip abduction felt on one side while and hoover’s sign
FI GURE 2 Hip abductor and Hoover’s sign of functional leg weakness. Top left: Hip abductor sign – weak left hip abduction. Top right: Hip abductor sign – strength in left hip returns to normal with abduction of right hip. Bottom left: Hoover’s sign – weak left hip extension. Bottom right: Hoover’s sign – strength in left hip extension returns to normal with right hip flexion.
Management errors were varied and remarkable for the frequency of patients with elevated troponin levels which were not repeated, and there was no indication that the elevated value was appreciated in the health record.
For patients with atrial fibrillation, unappreciated dual diagnoses (eg, acute heart failure, community-acquired pneumonia, exacerbation of chronic obstructive pulmonary disease), clinical severity, and missing the underlying cause contributed to diagnostic errors (eg, pulmonary embolism, community-acquired pneumonia).
3 cases of patients experiencing adverse drug effects related to warfarin and 3 related to direct oral anticoagulants.
Two patients with recent-onset atrial fibrillation and elevated Congestive Heart Failure, Hypertension, Age, Diabetes, previous Stroke scores were discharged without anticoagulation and returned with severe strokes.
Although patients discharged with syncope had fewer adverse events, the majority of events (10) were diagnostic errors, and 2 key contributing factor themes were failure to seek an underlying cause (eg, end-stage heart failure, community-acquired pneumonia, gastrointestinal bleeding) and lack of recognition of injuries related to the fall from syncope (eg, missed fractures)
Although intravascular temperature management does not improve survival compared with surface-cooling methods in post–cardiac arrest patients, it may improve neurologic outcomes.
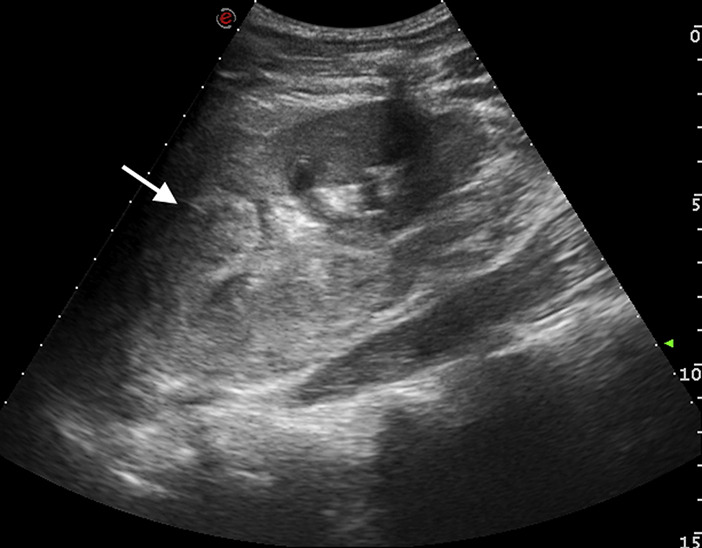
A 15-year-old previously healthy boy was admitted for a blunt abdominal trauma owing to a cycling crash. On admission he was alert; blood pressure and pulse rate were 145/95 mm Hg and 75 beats/min, respectively. Physical examination result was remarkable for severe left-sided flank pain with guarding. No others injuries were found. His urine was like blood and laboratory tests showed a normal hemoglobin level, at 13.5 g/dL, with hematocrit level 40.9%.
An abdominal ultrasonographic scan showed major left kidney trauma (Figure 1). A computed tomographic (CT) scan confirmed a grade IV renal laceration, according to the American Association for the Surgery of Trauma classification (Figure 2).
In patients with coma after out-of-hospital cardiac arrest, targeted hypothermia did not lead to a lower incidence of death by 6 months than targeted normothermia.
Conclusion: “Many risk stratification scores are not validated or not sufficiently accurate for clinical use. The CSRS is an accurate validated prediction score for ED patients with unexplained syncope. Its impact on clinical decision making, admission rates, cost, or outcomes of care is not known.”
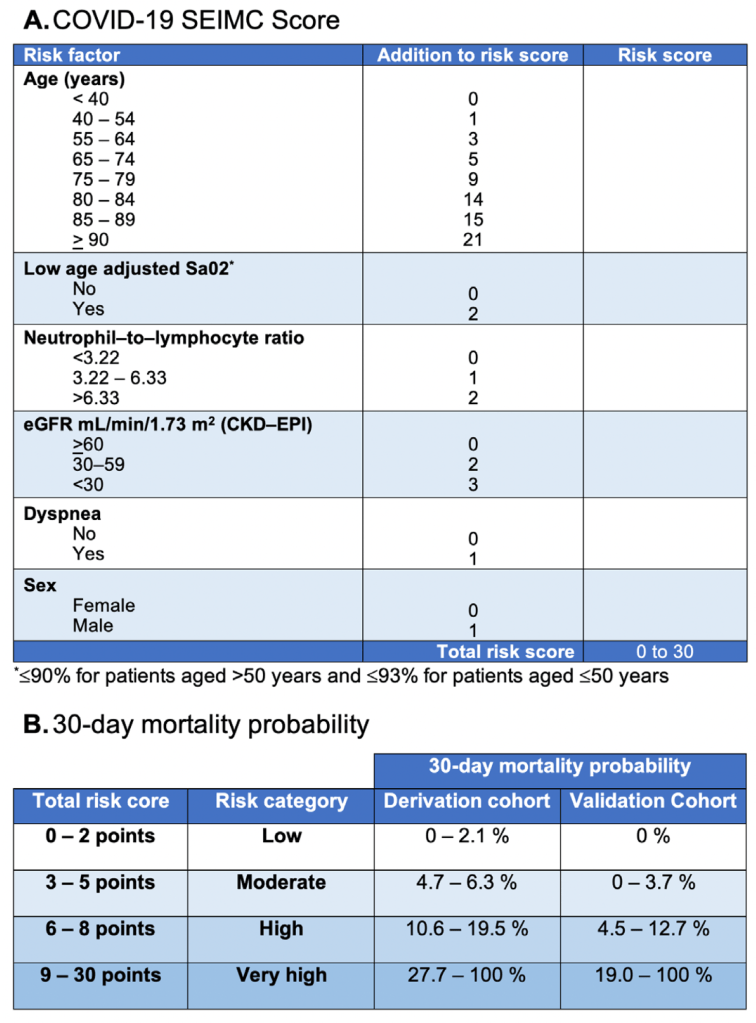
Of the 542 included patients, 46 (10%) required transfer to ICU within 24 hours of admission. The final composite model, adjusted for age and admission location, included history of heart failure and initial oxygen saturation of <93% plus either white blood cell count > 6.4 or glomerular filtration rate < 46. The odds ratio (OR) for decompensation within 24 hours was 5.17 (95% confidence interval [CI] = 2.17 to 12.31) when all criteria were present. For patients without the above criteria, the OR for ICU transfer was 0.20 (95% CI = 0.09 to 0.45).
Harm reduction for ED patients with injection drug use includes free dispensation of Naloxone (learn more about how EDs can get free naloxone to dispense here), and syringe services programs (find the SSP closest to you here).
2.6% of patients intubated patients recall an awareness of paralysis, with a two-fold risk among patients paralyzed with rocuronium (have your sedative ready to hang immediately after intubation).
Here’s the most important takeaway of the “HHS Practice Guidelines for the Administration of Buprenorphine for Treating Opioid Use Disorder”: All prescribers with a valid state license and DEA can register for an X wavier without mandatory training. It’s now a simple process. Get your X waiver TODAY!
PO Potassium Bicarbonate more palatable than KCl, dose is 50meq PO
Oral Magnesium Oxide 400-800mg tablet
Mag IV 4-8g if Mag<1, 2-4g if mag 1-1.4, 1-2g if Mag 1.5-1.9.
Calcium: 2g CaGluconate over 1 hour if sick.
Phosphate: typically replete if Phos<1, give Potassium Phos if K is low, give Sodium Phos if serum potassium is high, can give 15, 30 or 45 mmol depending on how low phosphate level is, typically 15 mmol/hr
Ask permission to share bad news: “I am afraid I have serious news. Would it be ok if I share?”
Align: “We need to work together quickly to make the best decisions for her care”.
Baseline function: “To decide which treatments might help her the most, I need to know more about her, what type of activities was she doing before her illness.”
“How much more would she be willing to go through for the possibility of more time?”
Preferred venous access is a 5f umbilical vein line, inserted in the little mouth of the umbilical stump face (umbilical arteries are the eyes, vein is the mouth). insert the 5f line 4-5cm until blood returns.
IO also an option but has a higher failure rate than in older kids.
Consider termination of CPR after 20 minutes with no detectable heart rate.
A total of 2,309 patients met criteria for inclusion in the study. Physician uptake of the HINTS exam was high, with 450 (19.5%) dizzy patients receiving all or part of the HINTS. A large majority of patients (96.9%) did not meet criteria for receiving the test as described in validation studies; most often this was because patients lacked documentation of nystagmus or described their symptoms as intermittent. In addition, many patients received both HINTS and Dix-Hallpike exams, which are intended for use in mutually exclusive patient populations. In no case was dizziness due to a central cause identified using the HINTS exam.
Sensitivity only 55% for gonorrhea with urine or endocervical swab so authors recommend empiric treatment rather than waiting for results. There is a counter-argument in the same issue but this one makes more sense to me. Probably should incorporate population characteristics and patient shared-decision making.
A 30-year-old man presented to the emergency department with throat pain and oral intolerance of fluids for several hours. Earlier that day, an outpatient operation was aborted after multiple unsuccessful intubation attempts in the operating room. The patient had unremarkable vital signs, noting only odynophagia. Computed tomography (CT) of the neck and an esophagram with water-soluble contrast were acquired.
This small trial found a trend toward benefit for the non-lytic group when comparing between patients treated with EVT alone versus EVT plus IVT for acute CVA.
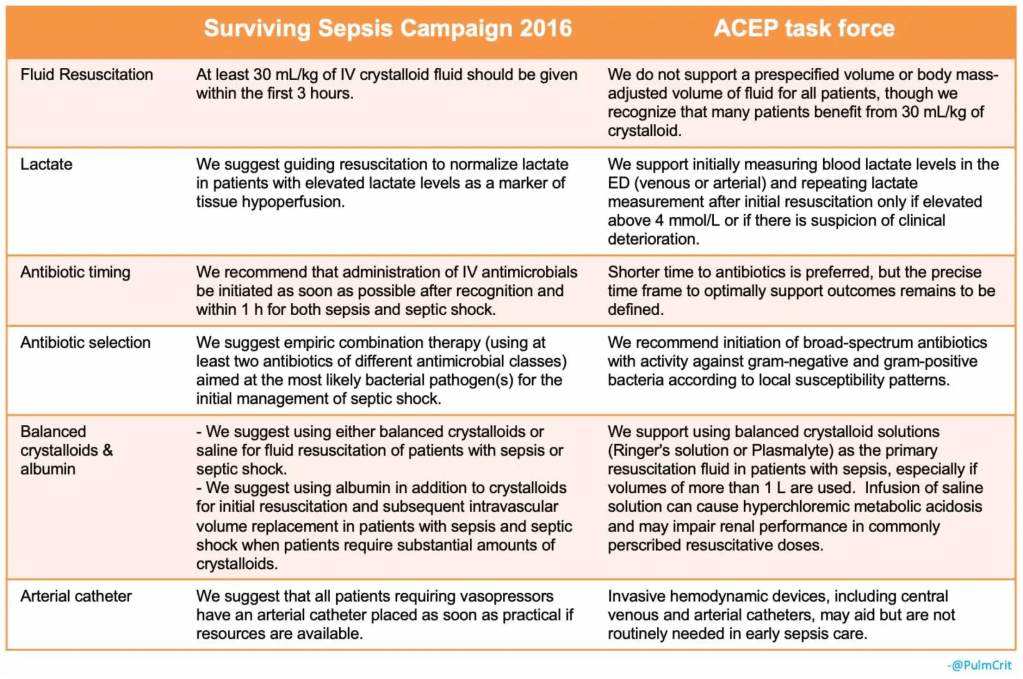
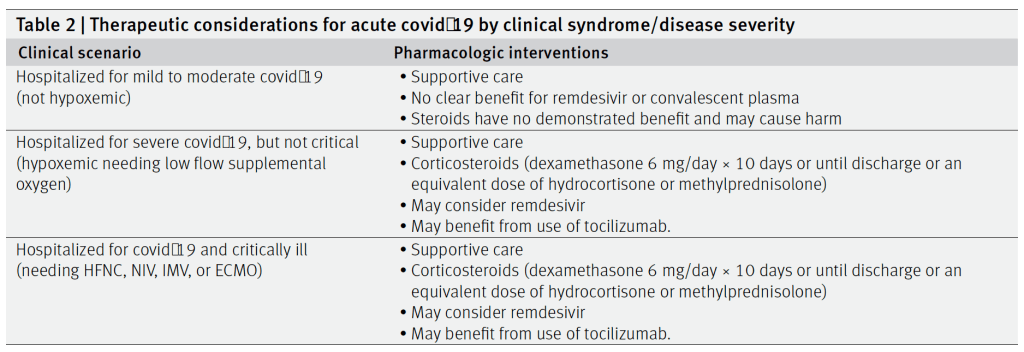
The ACEP consensus-based task force report was just published (see lead article in Annals of EM section above). Although spearheaded by ACEP, the report is also endorsed by the Society of Hospital Medicine (SHM) and the Society of Critical Care Medicine (SCCM).
In critically ill patients with Covid-19 receiving organ support in ICUs, treatment with the interleukin-6 receptor antagonists tocilizumab and sarilumab improved outcomes, including survival, at 90 days.
All patients with an adrenal mass that is discovered during diagnostic testing for another condition (an “incidentaloma”) should undergo biochemical testing to detect pheochromocytoma and excess cortisol secretion, and those who also have high blood pressure should undergo biochemical testing to detect primary hyperaldosteronism.
Patients with pheochromocytoma should undergo adrenalectomy after adequate presurgical alpha- blockade and beta-blockade, if necessary.
Patients with mild autonomous cortisol excess and primary hyperaldosteronism may benefit from adrenalectomy, but treatment should be individualized.
Nonfunctioning adrenal tumors that have an attenuation of 10 Hounsfield units or less on computed tomographic (CT) evaluation and that are smaller than 4 cm in greatest diameter generally do not warrant intervention or long-term follow-up.
All other adrenal incidentalomas with indeterminate features on imaging may warrant additional imaging with contrast-enhanced CT, magnetic resonance imaging with chemical-shift analysis, positron-emission tomography–CT with 18F-fluorodeoxyglucose, or all of these tests. The management of these masses should be individualized and should involve a multidisciplinary team consisting of an endocrinologist, an endocrine surgeon, and a radiologist.
Authors recommend replacing red man syndrome with infusion reaction for all non-immune mediated reactions.
Uptodate uses the term vancomycin flushing syndrome or vancomycin infusion reaction.
The two can be distinguished if it is the first time a patient has been exposed to vancomycin it will not be an IgE reaction.
Otherwise they can be difficult to distinguish and may require allergy consult/testing to distinguish.
Typically the infusion reaction is characterized by upper body, neck an face greater than lower body flushing, erythema and itching. Pain and muscle spasms in the back and chest as well as dyspnea and hypotension may occur.
In this methodologically novel trial (Goulden R et al. Association of Intravenous Radiocontrast With Kidney Function: A Regression Discontinuity Analysis. JAMA Intern Med 2021. [Link is HERE]) there was no association between IV contrast from CTPA and worsening eGFR up to 6 months after index ED visit. Although a randomized clinical trial would be great, this may be the highest-level evidence we achieve. This trial plus other observational trials on this topic all point to a change in protocols to allow for IV contrast in patients regardless of kidney function.
In summary, the evidence for using a patient’s GCS score is mixed. Recent review articles have highlighted the paucity of strong evidence behind the classic adage of “GCS less than 8, intubate”. Orso D et al. Endotracheal intubation to reduce aspiration events in acutely comatose patients: a systematic review. Scand J Trauma Resusc Emerg Med. 2020.
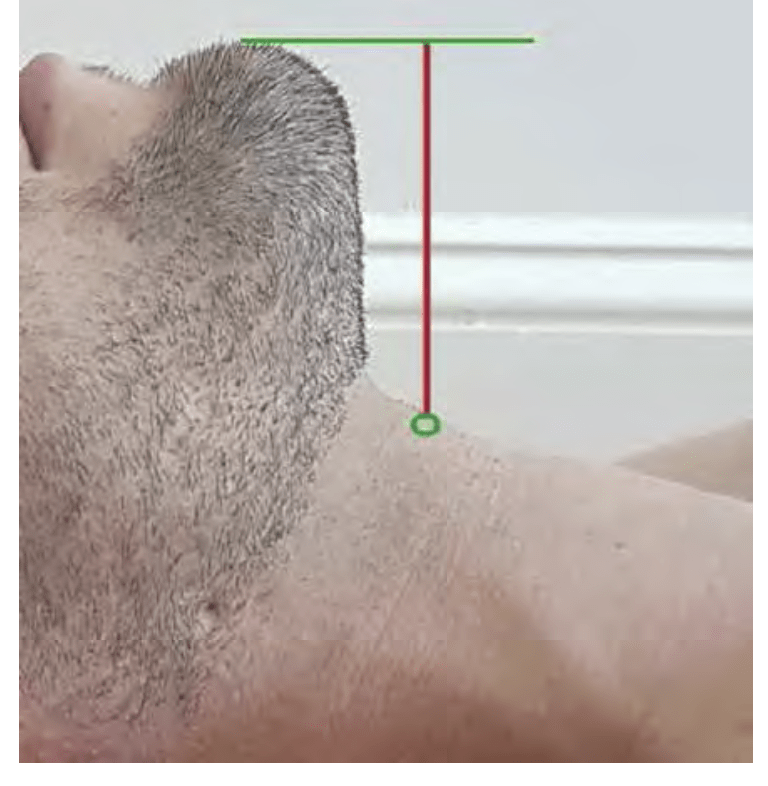
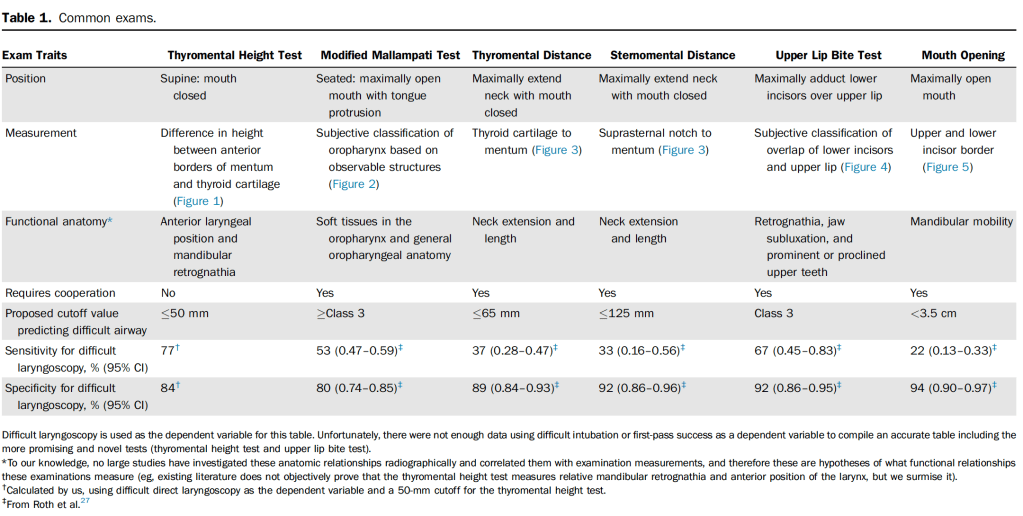
Several tools to assess airway difficulty but they require patient cooperation.
Thyromental height does not require patient cooperation and has both best sensitivity and moderate specificity.
Authors: “Early evidence on the thyromental height test is promising, given its higher sensitivity, reasonable specificity, and wider potential for application in the ED. However, to date no ED-, EMS-, or video laryngoscopy–based studies have been completed, to our knowledge.
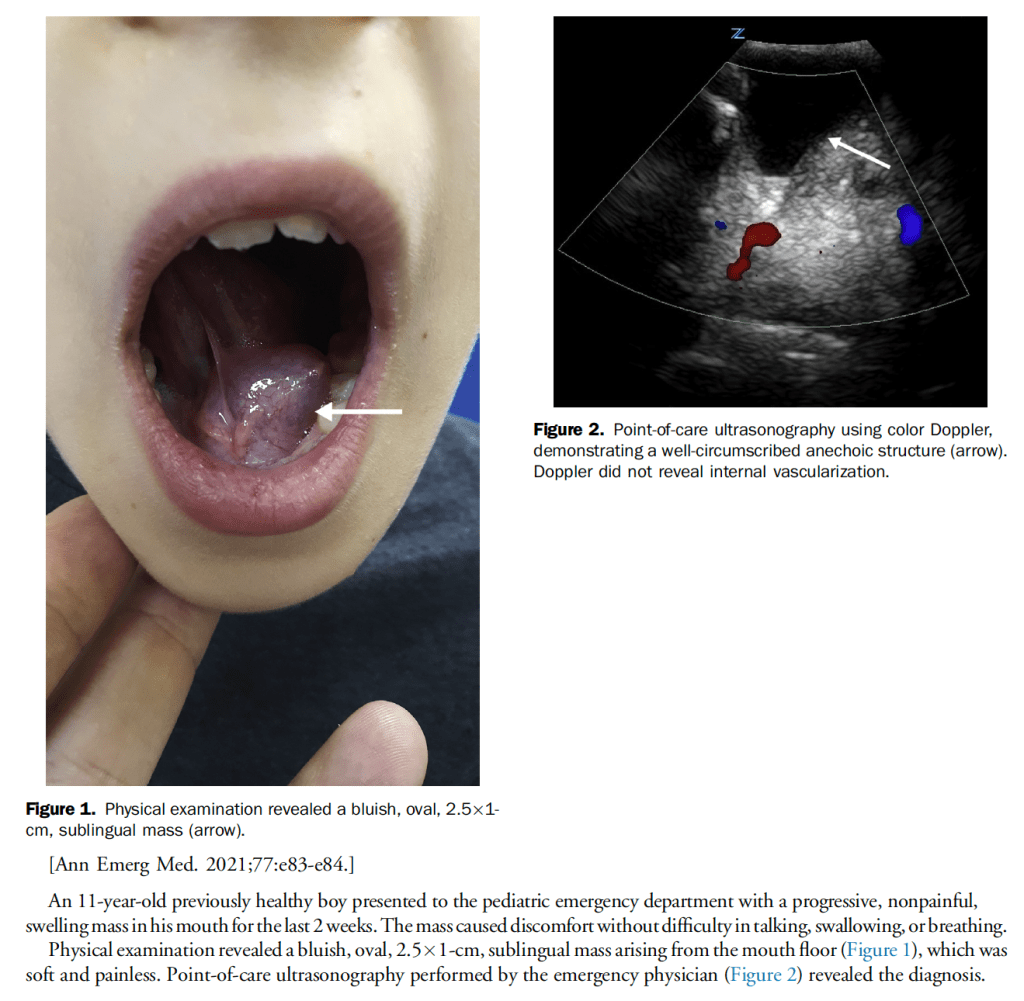
Sublingual ranula is a relatively common finding in the pediatric population, especially during the first and second decade of life, pseudocystic lesion, outpatient referral to ENT.
First and largest prospective multisite US cohort study to evaluate hs-cTnT strategies to date
NPV reached >99% with the combo 0 and 1 hour HS troponin plus a low heart score but using that approach only allowed 30.8% of patients to be discharged.
There was a high rate of MACE at 30 days (14.4%)
The study raises questions about whether HS-trop will improve efficiency if the discharge rate is 30.8%
Strawberry tongue seen in Strep but also in Kawasaki’s, this patient had 2 Kawasaki findings (tongue and lymphadenopathy) but needs fever for 5d and four additional findings (she had no rash, conjunctival injection or peripheral edema/erythema/desquamation).
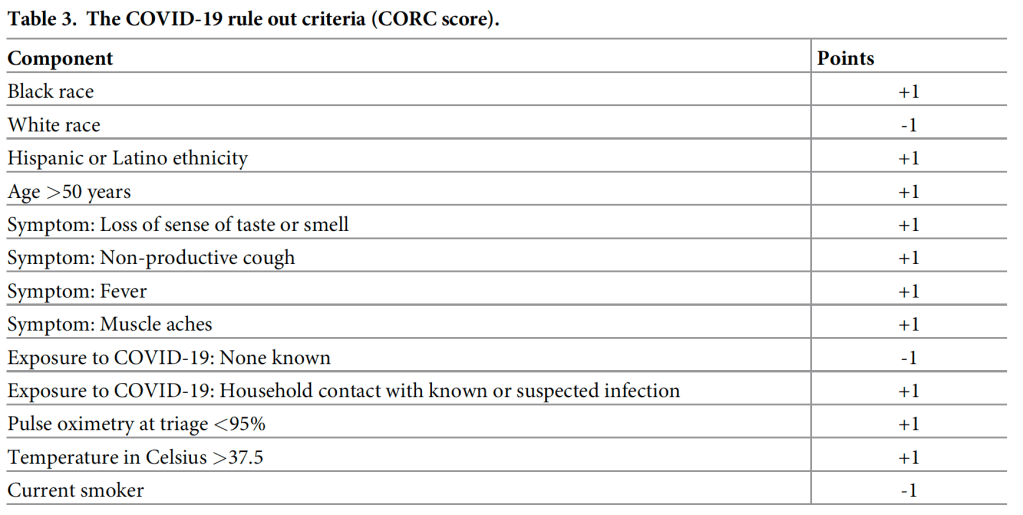
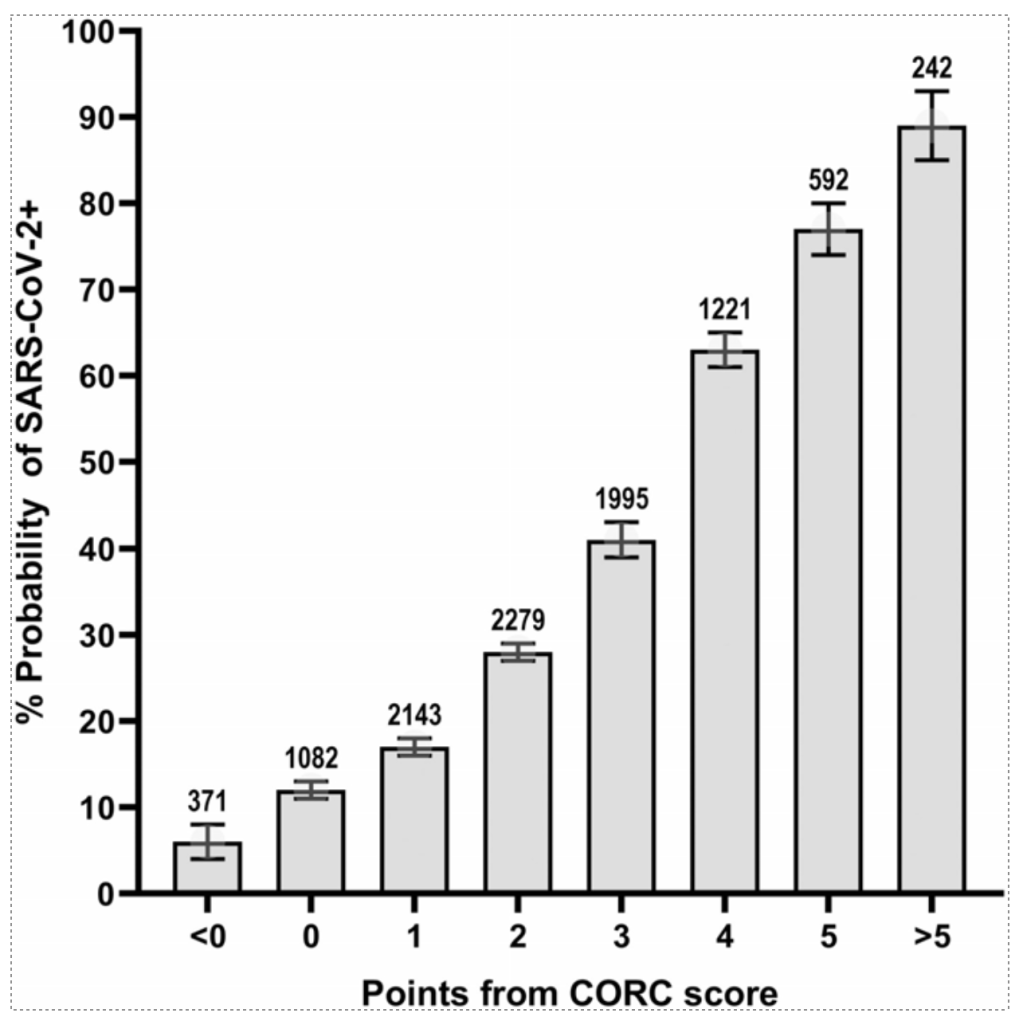
In the simplified score, a score of zero produced a sensitivity of 95.6% (94.8–96.3%), specificity of 20.0% (19.0–21.0%), negative likelihood ratio of 0.22 (0.19–0.26). Increasing points on the simplified score predicted higher probability of infection (e.g., >75%probability with +5 or more points).
We now have three randomized controlled trials (DIRECT-MT, DEVT, SKIP) as well as retrospective, non-randomized data (Phan 2017, Rai 2018) looking at this question.
In all three RCTs, the endovascular arm performed numerically better than the combination arm. This would appear to support a move towards endovascular therapy alone.
Addition of the HEART score to an initial hs-TnT below the limit of quantification improves sensitivity and NPV for cardiac events increasing patient safety, but this strategy does rule-out fewer patients (30.8%).
Clinical Take Home Point: Discharging patients presenting to the ED with chest pain after a single negative conventional troponin and proper risk stratification with the HEART score can be considered to be as safe as serial troponin testing while being less time consuming, less costly and therefore more patient oriented.
Paper: Wassie et al. Single versus serial measurements of cardiac troponin in the evaluation of emergency department patients with suspected acute myocardial infarction. JAMA Network Open 2021.
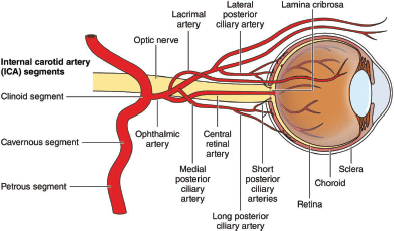
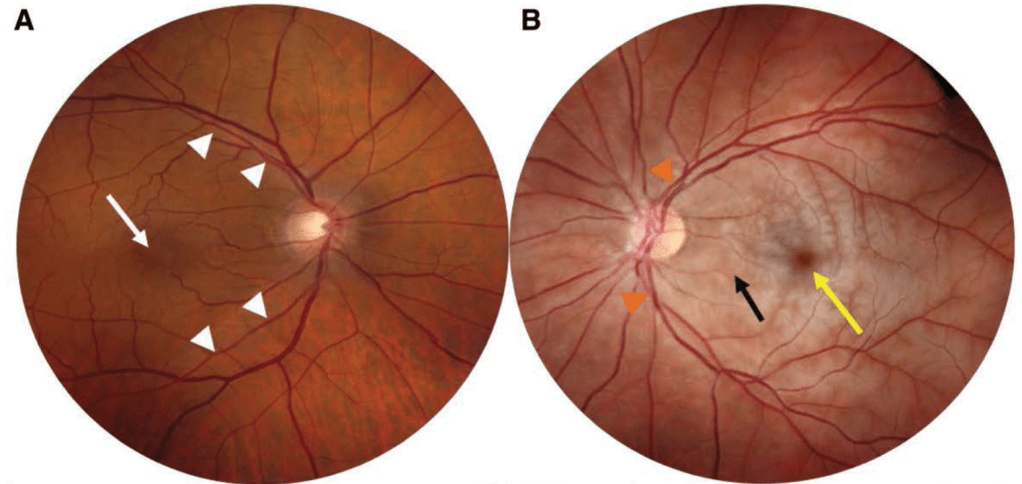
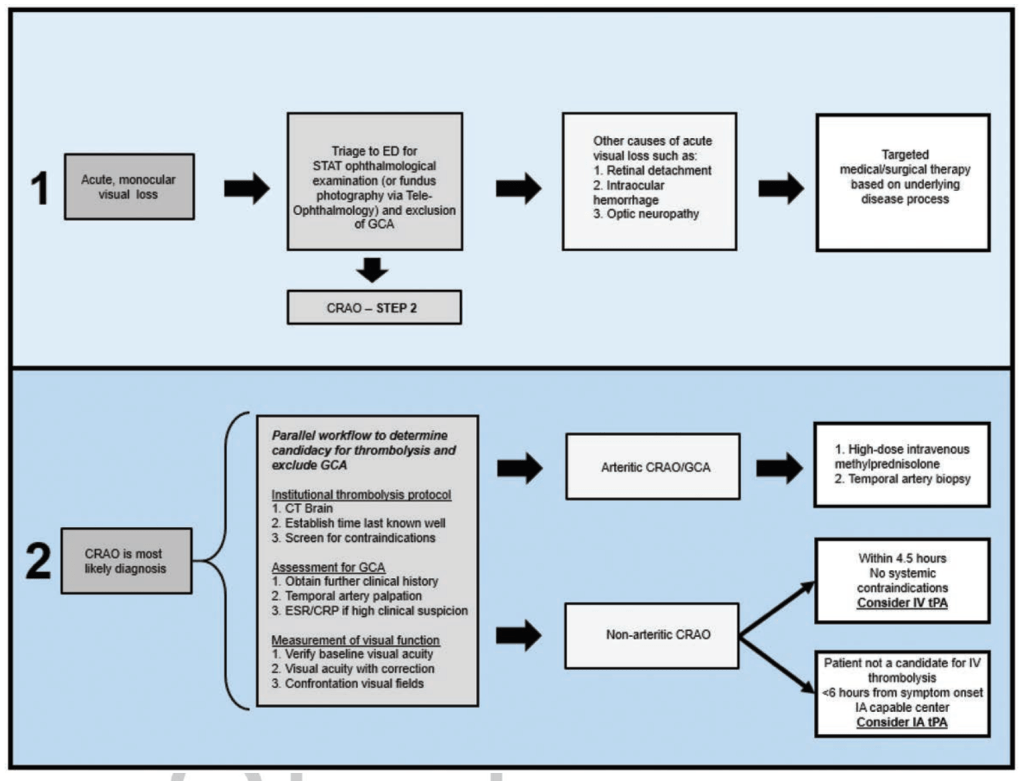
A, Fundus photograph of the normal right eye. Note the normal fovea (white arrow) and the normal retinal arteries (white arrowheads). B, Fundus photograph of a left CRAO showing diffuse retinal whitening (black arrow) with a cherry red spot (yellow arrow), attenuated arteries (orange arrowheads). Note the difference in color of the edematous retina compared with the normal right eye.
The success rates of the first attempt and the procedure time were statistically significant between the IO group and the CVC group (91.7% vs. 50.0%, P<0.001; 52.0 seconds vs. 900.0 seconds, P<0.001).
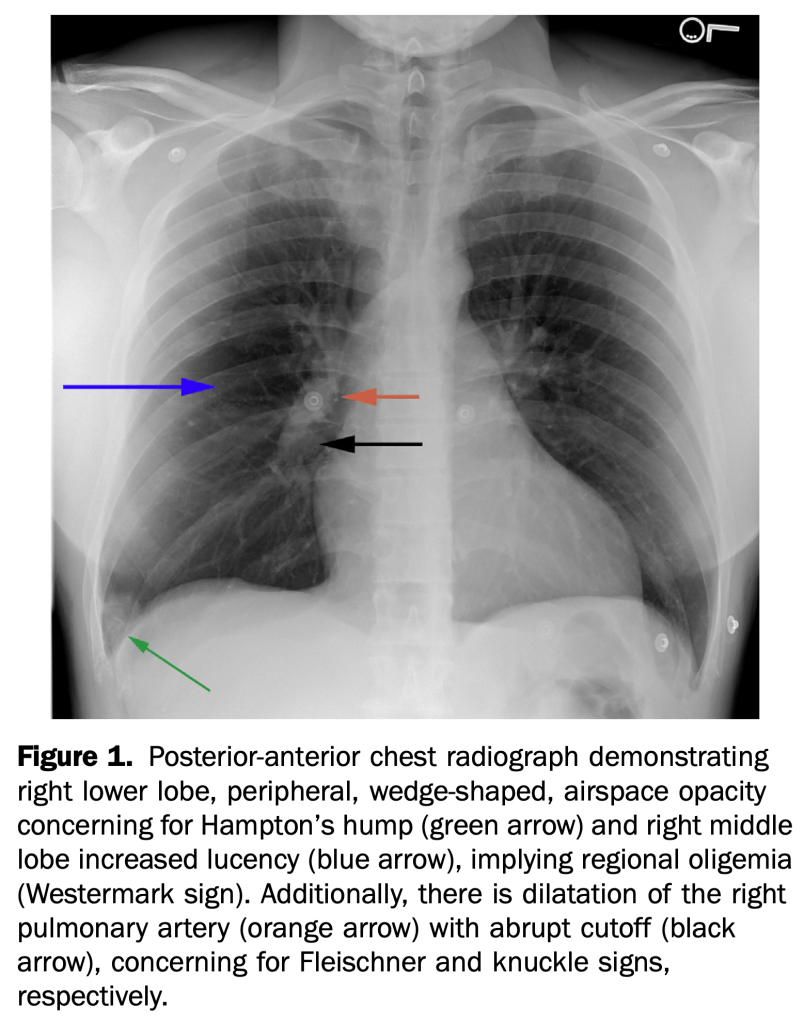
An otherwise healthy 35-year-old active duty military infantryman presented to the emergency department, complaining of intermittent dyspnea over one-week duration, which was worsened by exertion. He recalled some unusual left leg cramping three weeks before and reported an uncomplicated tooth extraction one week before, but denied any invasive surgeries.
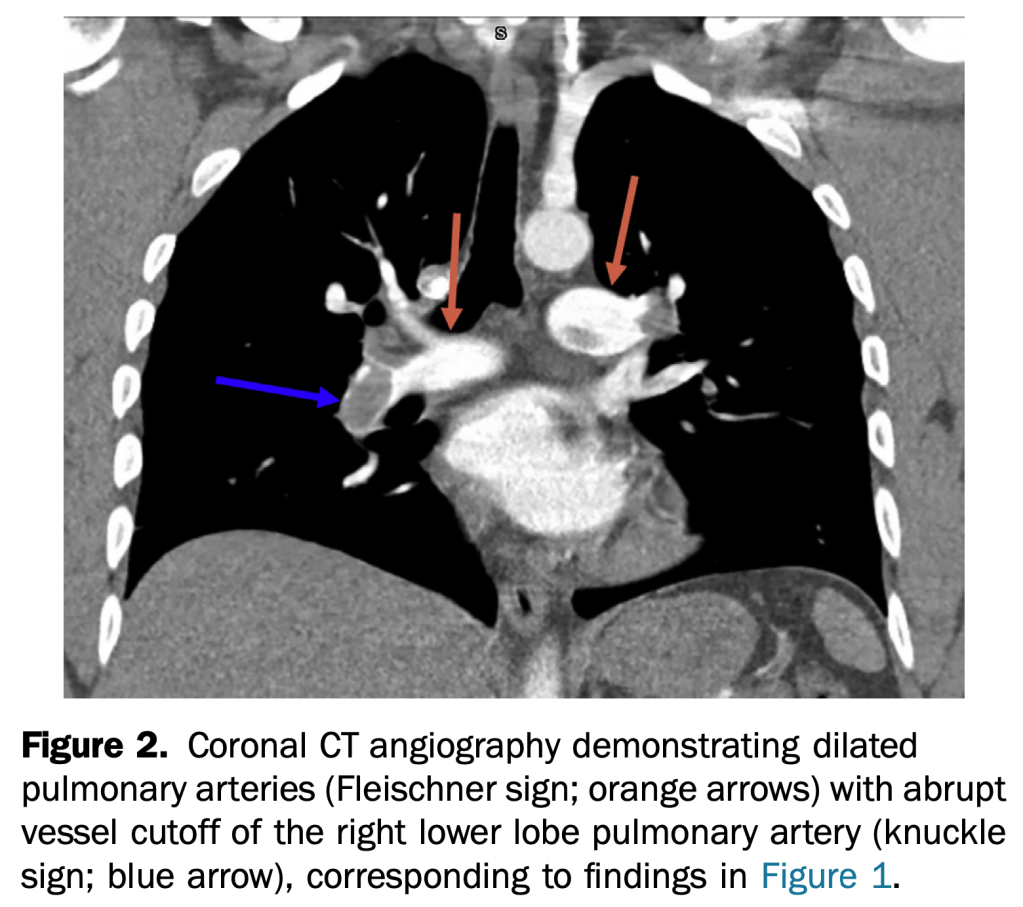
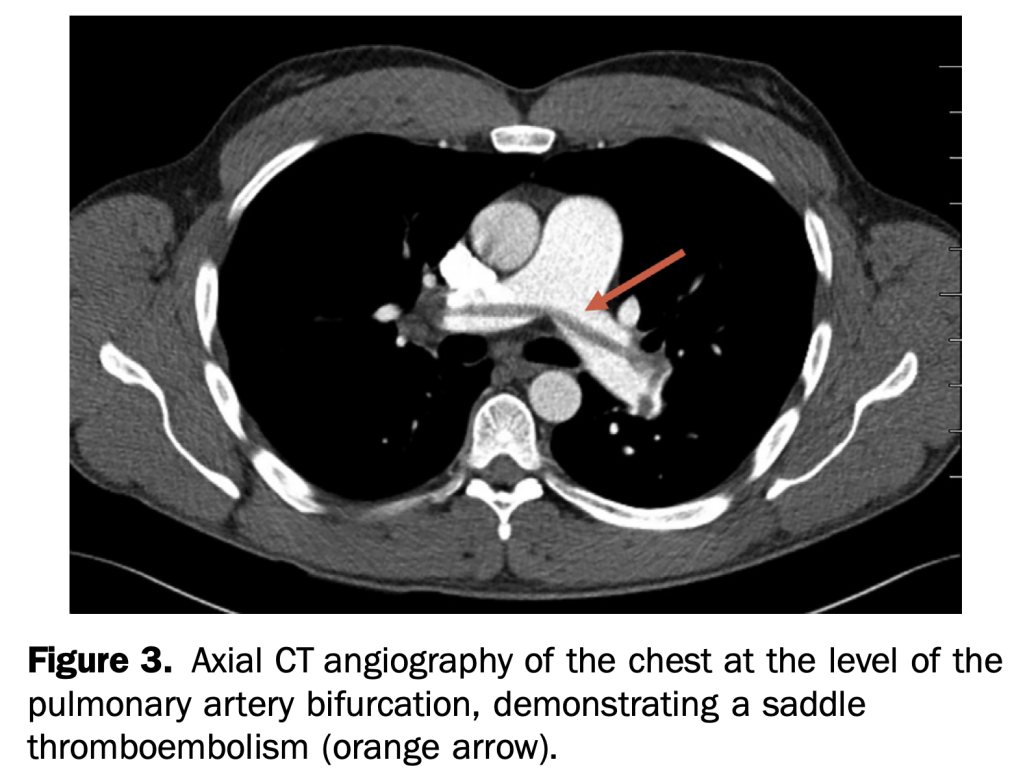
This case demonstrates multiple rare but specific radiographic findings of pulmonary embolism. These include the Westermark, knuckle, and Fleischner signs, in addition to Hampton’s hump.
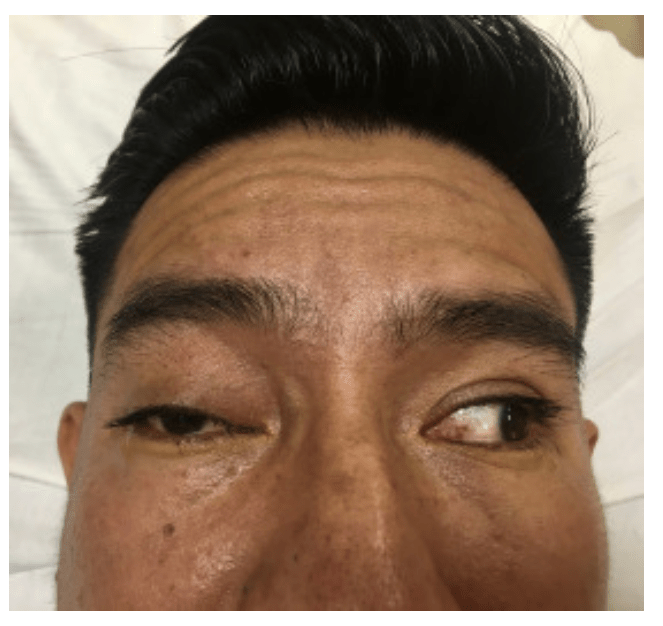
A 36-year-old man presented to the emergency department with double vision. Four weeks before, he had been struck in the face and he underwent open reduction and internal fixation of a mandibular fracture. He had intact cranial nerves in the immediate postoperative period. On examination, he displayed preserved visual acuity, a right-sided cranial nerve III palsy with an inferiorly abducted right eye, loss of medial and upward gaze, significant right-sided ptosis, and asymmetric mydriasis (Figure 1 and Video E1 [available online at http://www.annemergmed.com]). A bruit was auscultated over the affected eye.
Computed tomographic angiography of the brain revealed arterial filling of the cavernous sinus, consistent with a right-sided carotid-cavernous fistula and a dilated right ophthalmic vein.
Between January 1, 2010, and May 31, 2017, 205 pregnant patients presented to the ED with a neurologic chief complaint. The majority of patients had a normal neurologic examination result. Patients with an abnormal examination result were not more likely to have clinically significant imaging findings.
Within our population, 28% underwent imaging, and noncontrast magnetic resonance imaging was the most common modality. Five patients had clinically significant imaging findings. Specifically, 3.3% of patients with abnormal examination result had significant findings and 2.3% of those with a normal examination result had significant findings.
A normal examination result does not adequately exclude serious intracranial pathology, and diagnostic vigilance is justified.
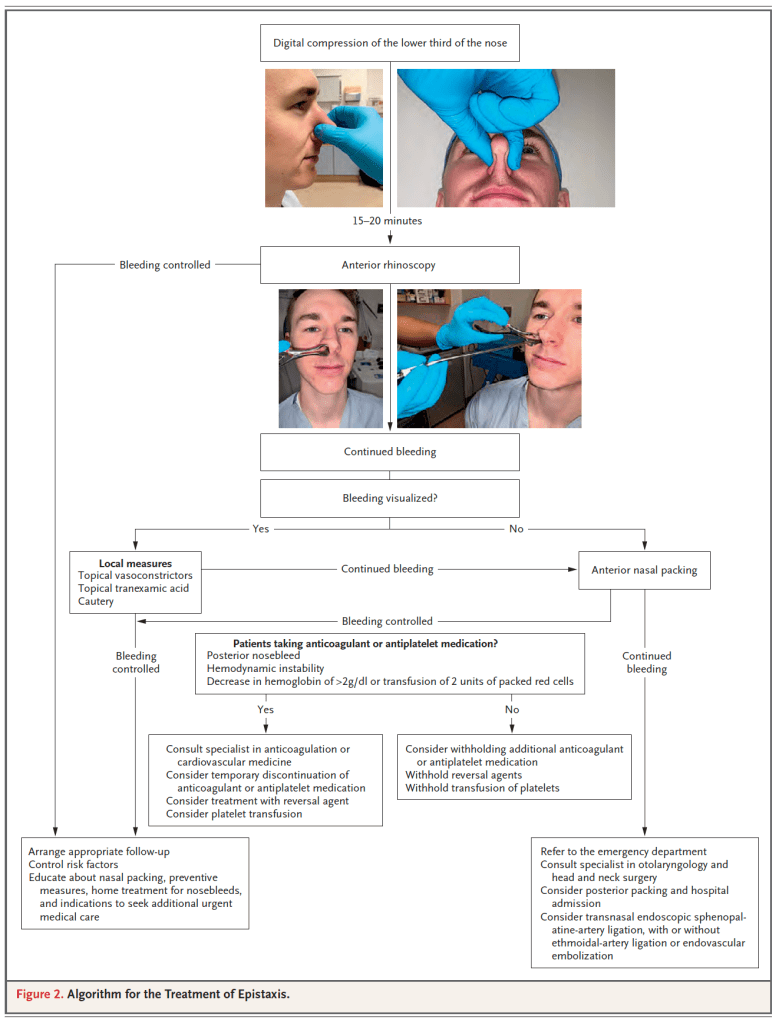
In patients presenting to an ED with atraumatic epistaxis that is uncontrolled with simple first aid measures, topical tranexamic acid applied in the bleeding nostril on a cotton wool dental roll is no more effective than placebo at controlling bleeding and reducing the need for anterior nasal packing.
The Canadian TIA Score stratifies patients seven day risk for stroke, with or without carotid endarterectomy/carotid artery stenting, and is now ready for clinical use.
Incorporating this validated risk estimate into management plans should improve early decision making at the index emergency visit regarding benefits of hospital admission, timing of investigations, and prioritization of specialist referral.
Excluded: had neurological deficits for more than 24 hours (that is, a stroke according to the World Health Organizationí s definition), had a decreased level of consciousness from their baseline (that is, Glasgow Coma Scale <15 in previously cognitively normal patients), had an alternative diagnosis (for example, hypoglycemia, seizure, electrolyte imbalance, or migraine), presented more than seven days after onset of the neurological symptoms, or were treated with tissue plasminogen activator or embolectomy for an acute stroke.
7607 consecutively enrolled adult patients (80.6% of all potentially eligible patients)108 (1.4%) had a subsequent stroke within 7d
83 (1.1%) had carotid endarterectomy/carotid artery stenting within 7d
9 patients had both within 7d leaving 182 with outcomes
Low risk: 16.3% of patients, 7d risk of CVA or carotid procedure ≤0.5%;
Medium risk: 72.1% of patients, 7drisk of CVA or carotid procedure 2.3%;
High Risk: 11.6% of patients, 7drisk of CVA or carotid procedure: 5.9%;
Authors recommend Head CT and routine follow-up for low risk patients, CTA head/neck for medium risk and with rapid follow-up.
BIG PEARL: avoid intubation in severe metabolic acidosis patients, if possible, allow them to continue their compensatory breathing until you can correct underlying problem (especially true for easily fixable problems like DKA, less so for severe sepsis).
Smaller pearl: cause of acidosis as important as the actual number in determining prognosis, low pH from COPD, DKA or even salicylate poisoning easier to resuscitate and better prognosis than septic shock.
Scant evidence for bicarb boluses but Weingart doesn’t use because if patient is already maxed out on respiratory compensation, the added bicarb simply gets converted to CO2 that can no longer be blown off.
Weingart does use 3 amps of NaBicarb in D5W drip for salicylate poisoning, but not for DKA
Place on Vent with NIV mask with pressure support to augment respiratory drive before intubation to determine the minute ventilation that needs to be matched after intubation.
Once patient is induced but before paralysis occurs, patient should be switch to vent settings RR 12, TV 8cc/kg, this lower RR should reduce risk of gastric dissension and vomiting.
Once patient is intubated, empiric settings RR 30, TV 8cc/kg.
Ask RT to confirm patient is exhaling whatever they are inhaling and not air stacking due to the high RR.
If patient is air stacking, switch to the square breathing curve with a high inspiratory flow rate.
27 918 patient encounters (16 212 women [58.1%]; mean [SD] age, 58.7 [15.2] years) were included in the study.
Of patients with an initial troponin measurement below the level of detection, 14 459 (51.8%) were discharged after a single troponin measurement, and 13 459 (48.2%) underwent serial troponin tests.
After adjustment for cardiac risk factors and comorbidities, there was no statistically significant difference in the primary outcome of acute myocardial infarction or cardiac mortality within 30 days between the 2 groups (single troponin, 56 [0.4%] vs serial troponin, 52 [0.4%]; adjusted odds ratio, 1.41 [95% CI, 0.96-2.07]).
Patients discharged after a single troponin test had lower rates of coronary artery bypass graft (adjusted odds ratio, 0.24 [95% CI, 0.11-0.48]) and invasive coronary angiography (adjusted odds ratio, 0.46 [95% CI, 0.38-0.56]).
This study suggests that patients are routinely discharged from the ED after a single negative troponin test result, and when compared with serial troponin testing, a single troponin test appears safe based on current physician decision-making, with no difference in rates of 30-day cardiac mortality and acute myocardial infarction, which are low in both groups.
Didn’t realize that addition of anticoagulant therapy to anti platelet therapy has been shown to improve outcomes after ACS but is not routinely done due to increased risk of bleeding.
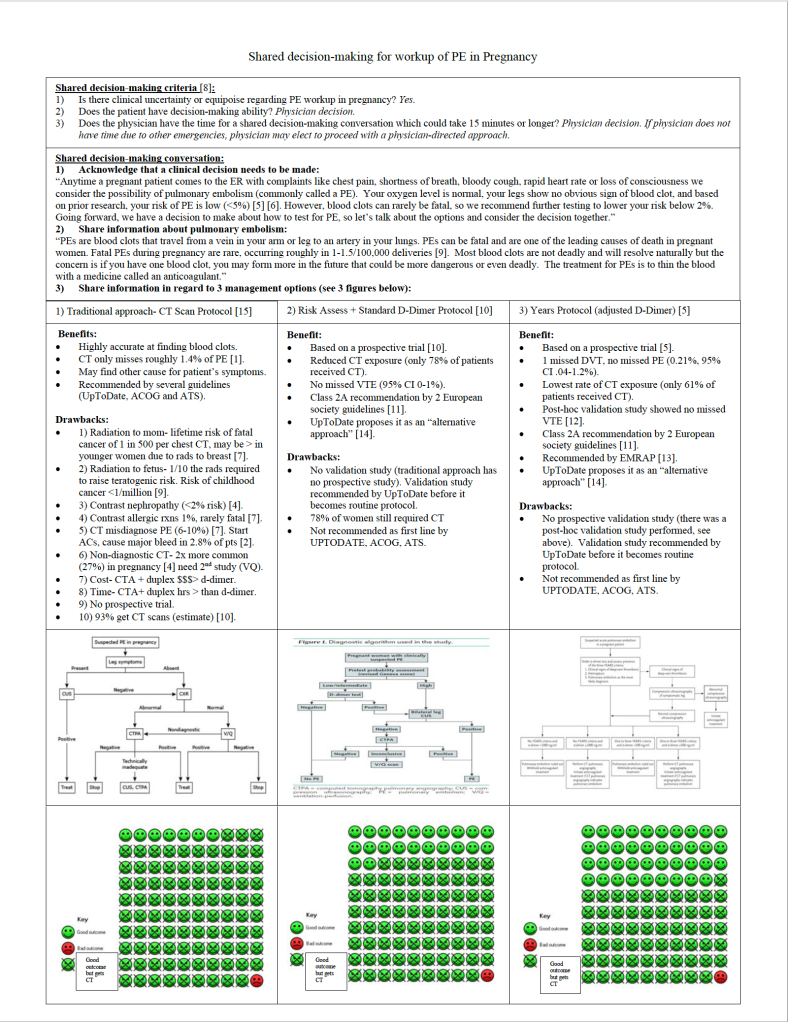
Despite physiologic reasons why pregnant women would be at increased risk for PE (hypercoagulable state, venous stasis ), they surprisingly have roughly the same rate of diagnosed PE (32/100k) as the general population of women under the age of 40 according to Olmsted County data published by Heit and referenced by Kline, as long as you remove isolated DVT and postpartum state. Early postpartum state, on the other hand, has roughly a 10 fold increased risk (421/100k). Normal physiologic changes of pregnancy such as dyspnea, leg swelling, increased resting heart rate can all mimic PE. For this reason, as well as the specter of missing potentially deadly PE that harms two patients simultaneously, physicians have been found to overtest for VTE, with a rate of positive VTE around 4% (Kline 2014 and van der Pol 2019), which is 1/3 the rate of positive workups in the general population. To make matters worse, the traditional workup, endorsed by American Thoracic Society and ACOG in 2011, did not use risk assessment or D-Dimer in pregnant patients due to lack of prospective trials and instead went directly to duplex and CT or VQ. As Kline breaks down in his 2015 review of the workup for PE, the risks to pregnant moms from CT not only include the 1 in 500 chance of a fatal cancer, but also the 26% chance of a non-diagnostic study study (higher cardiac output and higher plasma volume during pregnancy make the timing of the bolus less reliable), and the 6-10% chance of a false positive study in low risk populations which subjects the patient to 3-6 months of anticoagulation.
For many emergency clinicians, the NEJM publication of van der Pol’s Pregnancy-Adapted Years Algorithm for Diagnosis of Suspected Pulmonary Embolism in 2019 was all we needed to begin offering patients an alternative to mandatory CT for all low risk PE workup. Righini had already published a Pregnancy PE protocol that employed risk assessment with a normal D-Dimer but unfortunately this only reduced CT utilization in 22% of pregnant patients.
The challenge with using Years to guide management is that some leading expert guidelines (ACOG and ATS) which have not been updated since 2011 still recommend CT for all or, in the case of UpToDate, are calling for a second validation study before recommending the Years approach. Years was validated by the Righini group in a post-hoc fashion and showed a 0% miss rate but a prospective validation study is not yet published.
So what is a pregnant patient and a well-intentioned physician to do?
Shared decision-making!
Here is my attempt at a shared decision-making script to help patients decide what feels best for them.